-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4294-4297
doi:10.5923/j.ajmms.20251512.20
Received: Oct. 12, 2025; Accepted: Nov. 26, 2025; Published: Dec. 8, 2025

Clinical Features of Negative Disorders and Cognitiv Deficit in Paranoidal Schizophrenia in the Aral Sea
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPalvanov Ravshan Otamuratovich1, Sharipova Farida Kamilovna2, Kevorkova Marina Anatolevna3
1Assistant Lecturer, Department of Psychiatry and Narcology Urgench State Medical Institute, Urgench, Uzbekistan
2PhD, Associate Professor, Department of Psychiatry, Narcology, Child Psychiatry, Medical Psychology and Psychotherapy, Tashkent State Medicine University, Tashkent, Uzbekistan
3PhD, Senior Lecturer, Department of Psychiatry and Narcology, Tashkent State Medicine University, Tashkent, Uzbekistan
Correspondence to: Palvanov Ravshan Otamuratovich, Assistant Lecturer, Department of Psychiatry and Narcology Urgench State Medical Institute, Urgench, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Paranoid schizophrenia is commonly accompanied by negative symptoms and cognitive impairment, which significantly limit social functioning. Environmental stress factors may intensify these disturbances. Objective. To evaluate negative symptoms and cognitive deficits in patients with paranoid schizophrenia living in the Aral Sea region and determine the association between them. Materials and methods. The study included 226 patients aged 28 – 45 years from Khorezm, Karakalpakstan, and Tashkent. Negative symptoms were measured using CAINS and cognitive performance using BACS at three 30 – day intervals. Results. Patients in Khorezm and Karakalpakstan showed a significant increase in negative symptoms and a decline in cognitive function (p<0.01), while values in Tashkent remained stable. A strong negative correlation was found between CAINS and BACS scores in the total sample (r≈–0.70, p<0.001). Conclusion. Progressive negative and cognitive disturbances in the Aral Sea region require early and targeted rehabilitation strategies.
Keywords: Paranoid schizophrenia, Negative symptoms, Cognitive deficit, CAINS, BACS
Cite this paper: Palvanov Ravshan Otamuratovich, Sharipova Farida Kamilovna, Kevorkova Marina Anatolevna, Clinical Features of Negative Disorders and Cognitiv Deficit in Paranoidal Schizophrenia in the Aral Sea, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4294-4297. doi: 10.5923/j.ajmms.20251512.20.
1. Introduction
- Paranoid schizophrenia is a long – standing psychiatric disorder in which alterations in emotional expression, motivational capacity, and interpersonal functioning gradually develop, eventually causing patients to limit their social communication to a small and restricted circle [1,2]. According to a number of clinical and psychological studies, individuals with schizophrenia frequently experience impaired self – awareness and an increased tendency toward self – stigmatization, which is accompanied by chronic feelings of guilt, shame, and reduced self – worth [3-6]. The persistence of such internalized negative experiences leads to avoidance of social interaction and further narrows opportunities for functional integration into society.As the illness progresses, deep disruptions occur within the patient’s motivational systems, hierarchy of needs, and meaning – formation processes. These pathological changes negatively affect adaptive behavior and significantly complicate psychosocial adjustment [7]. Epidemiological research shows that the major negative symptoms of schizophrenia – such as avolition, anhedonia, alogia, asociality, and diminished emotional expressivity – are observed in roughly one – fifth to one – third of patients, and both primary and secondary deficit syndromes worsen long – term outcomes while imposing a notable socioeconomic burden on families and healthcare services [8-10]. Furthermore, remission phases characterized by persistent negative symptoms are reported to occur more often than those dominated by positive symptoms, highlighting the decisive role of negative features in predicting rehabilitation potential and long – term functioning [11-13].Cognitive impairment represents the second key dimension of schizophrenia. Deficiencies in attention, verbal fluency, working memory, processing speed, and executive functioning make a substantial contribution to disability, social dysfunction, and reduced treatment efficacy [14-17]. Importantly, these cognitive problems often persist even during periods of relative clinical stability and remain one of the strongest predictors of functional prognosis.Another important component of the disorder is the distortion of psychological defense mechanisms – automatic processes that normally help preserve emotional equilibrium. In schizophrenia, these mechanisms frequently become rigid, maladaptive, and poorly integrated, resulting in inaccurate interpretations of internal experiences and external events, which further complicate coping behavior and stress regulation [18]. Environmental factors also play a considerable role: long – term ecological deterioration in the Aral Sea region, including chronic environmental stressors and socioeconomic instability, is known to intensify psychological strain and may exacerbate the course of psychiatric disorders [19].Understanding how ecological adversity, negative symptom progression, and cognitive dysfunction interact in vulnerable populations remains an essential scientific and clinical task. Such knowledge provides deeper insight into disease mechanisms and offers practical guidance for improving diagnosis, monitoring, and rehabilitation strategies.The aim of the present study was therefore to examine the clinical characteristics and interaction between negative symptoms and cognitive deficits in individuals diagnosed with paranoid schizophrenia living in the Aral Sea region.
2. Material and Methods
- The study involved 226 patients diagnosed with paranoid schizophrenia (PSh) who were treated in Khorezm Region, the Republic of Karakalpakstan, and the city of Tashkent. The cohort consisted of patients aged 28 to 45 years, with a mean age of 36.5 ± 8.5 years. Among the respondents, 51.7% (n=117) were men and 48.3% (n = 109) were women. The clinical diagnosis of paranoid schizophrenia in patients was established by the attending psychiatrist in the psychiatric ward according to clinical protocols (ICD-10 and DSM-5 criteria). To exclude chronic somatic pathology, in addition to the psychiatric examination, patients were also evaluated by a neurologist and a cardiologist.All patients were examined in three comparative groups:Group I – 124 patients diagnosed with paranoid schizophrenia (PSh) from the Khorezm Region;Group II – patients with PSh from the Republic of Karakalpakstan (n = 109);Group III (comparative group) – patients with PSh from the city of Tashkent (n = 51).For the purpose of psychodiagnostic evaluation, a set of standardized psychological assessment tools was utilized to obtain an objective picture of the progression of negative symptoms and cognitive disturbances identified during the clinical interview. In this context, the Clinical Assessment Interview for Negative Symptoms (CAINS), a specialized instrument developed to measure various domains of negative symptomatology [20,21], as well as the Brief Assessment of Cognition in Schizophrenia (BACS), a widely recognized tool for evaluating overall cognitive performance [22], were administered. The psychodiagnostic procedures were carried out in a dynamic format, meaning that each patient underwent repeated assessments three times at 30-day intervals.
3. Results
- Throughout the research, several notable findings were recorded. The evaluation of negative symptom progression in patients with paranoid schizophrenia residing in the Aral Sea region was performed using the CAINS scale (Table 1) [20], and the analysis revealed the following outcomes.
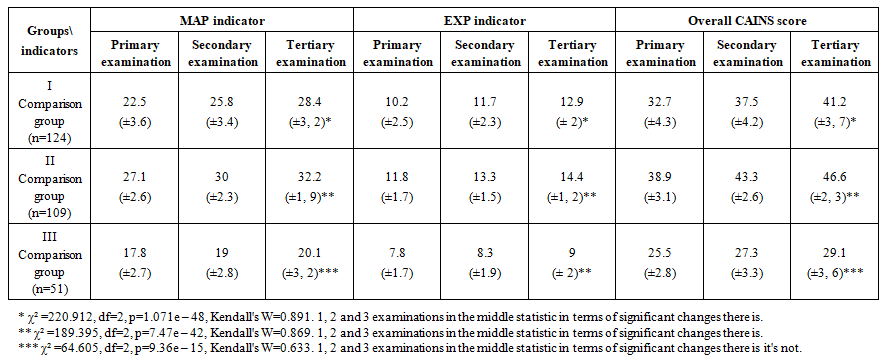 | Table 1. CAINS scale in 3 reviews on average points and standard deviation |
|
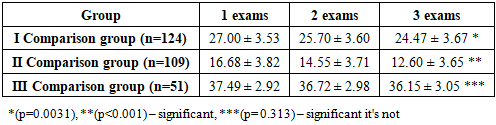
 | Figure 1. Comparison of BACS and CAINS indicators regions according to correlation analysis |
4. Discussion
- The findings of the present study conducted in the Aral Sea region demonstrate that, among individuals diagnosed with paranoid schizophrenia, negative symptom severity – measured through the CAINS scale – and cognitive performance – assessed via the BACS instrument – are functionally interconnected. Moreover, the magnitude and direction of these changes differed markedly across the examined geographical areas, reflecting the influence of environmental and regional factors on the clinical manifestation of the disorder.Analysis of CAINS scores revealed that patients residing in both the Khorezm Region and the Republic of Karakalpakstan exhibited a steady and statistically significant increase in all domains of negative symptomatology, including motivational deficits, emotional expressivity, and overall total scores (p < 0.001). This upward trajectory aligns with existing research suggesting that chronic environmental stressors and ecological instability may aggravate deficit-related psychopathology and intensify negative emotional–motivational states [23].In contrast, evaluation of cognitive performance using the BACS scale indicated a progressive decline in cognitive functioning in the same two regions. Scores significantly decreased across repeated assessments (p < 0.01), implying an intensification of cognitive impairment over time. Meanwhile, in the Tashkent group, changes in BACS indicators were minimal and did not reach statistical significance, which may reflect comparatively more favorable ecological and psychosocial living conditions – consistent with patterns described in other populations exposed to less environmental adversity [24].Correlation analysis across all regions further revealed a pronounced inverse association between CAINS and BACS scores in the combined sample (r = – 0.696; p ≪ 0.001). This relationship indicates that improvements in cognitive functioning correspond with a reduction in negative symptom severity. However, when each region was analyzed independently, the correlations were weak or non-significant. This discrepancy can be understood through the lens of Simpson’s paradox, whereby a strong overall association arises due to substantial intergroup differences rather than uniform within-group trends. Thus, while regional variability drives the aggregate relationship, the internal dynamics within each region reflect distinct and largely independent processes influencing cognitive and negative symptom domains.
5. Conclusions
- Overall, the study results indicate that in the Aral Sea region, patients with paranoid schizophrenia experience a simultaneous deepening of negative symptoms and cognitive deficits. This progression leads to social dysfunction, a slowdown in the rehabilitation process, and a decline in quality of life. Therefore, a comprehensive assessment of cognitive and negative impairments, along with the early implementation of rehabilitative interventions, is of great importance for improving the prognosis of the disorder.