-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4289-4293
doi:10.5923/j.ajmms.20251512.19
Received: Nov. 6, 2025; Accepted: Nov. 29, 2025; Published: Dec. 8, 2025

Characteristics of the Development of Cardiorenal Syndrome in Salt-Sensitive Arterial Hypertension in the Population of the Aral Sea Region
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAtaniyazov Khurshid Khamidovich1, Khamidullaeva Gulnoz Abdusattarovna2
1PhD., Head of the Department of "Arterial Hypertension" of the Regional Branch of the Republiс of Karakalpakstan of the Republican Specialized Scientific and Practical Medical Center for Cardiology of the Republic of Uzbekistan, City Nukus, Uzbekistan
2DSc., Associate Professor, Head of the "Arterial Hypertension" Department of the Republican Specialized Cardiology Scientific and Practical Medical Center, City Tashkent, Uzbekistan
Correspondence to: Ataniyazov Khurshid Khamidovich, PhD., Head of the Department of "Arterial Hypertension" of the Regional Branch of the Republiс of Karakalpakstan of the Republican Specialized Scientific and Practical Medical Center for Cardiology of the Republic of Uzbekistan, City Nukus, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Characteristics of the development of cardiorenal syndrome in patients with arterial hypertension in the population of the Aral Sea region remains a problem that has not been scientifically studied and has not been thoroughly studied. Background: Study of the characteristics of the development of cardiorenal syndrome in the course of salt-sensitive arterial hypertension in the inhabitants of the Aral Sea region. Methods: The study included 1021 patients aged 40–70 years who were diagnosed with hypertension in district family clinics. The results of laboratory-instrumental analysis of all patients included in the study were analyzed. Results: It was found that cardiorenal syndrome in patients with salt-sensitive arterial hypertension in the Aral Sea region is due to the interrelated development of cardiac and renal dysfunction. Conclusions: The results of the study suggest that patients with salt-sensitive arterial hypertension in the Aral Sea region should receive combined cardioprotective and nephroprotective therapy.
Keywords: Arterial hypertension, Remodeling, Creatinine, Urea, Uric acid, Microalbuminuria, Cardiorenal syndrome, Cardioprotective and nephroprotective therapy
Cite this paper: Ataniyazov Khurshid Khamidovich, Khamidullaeva Gulnoz Abdusattarovna, Characteristics of the Development of Cardiorenal Syndrome in Salt-Sensitive Arterial Hypertension in the Population of the Aral Sea Region, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4289-4293. doi: 10.5923/j.ajmms.20251512.19.
1. Introduction
- Cardiorenal syndrome (CRS) is a pathological process in which the heart and kidneys are interconnected and one causes the development of acute or chronic dysfunction of the other. CRS includes a variety of acute and chronic diseases, in which the primary affected organ may be the heart or kidneys. The kidneys participate in important metabolic processes, in the regulation of the humoral system, and in microcirculation, and are susceptible to acute and chronic effects in various cardiovascular diseases (CVD), influencing the origin and development of cardiovascular pathologies. The development of renal dysfunction is associated with recurrent myocardial ischemia, myocardial infarction (MI), stroke, and acute and chronic heart failure. Even a slight decrease in kidney function significantly worsens cardiac pathology, simultaneously increasing the frequency of complications and the risk of death, while a decrease in myocardial contractility has a very negative effect on kidney function.The need for early identification of the risk of kidney damage in cardiovascular diseases, as well as the development of strategies and methods for monitoring patients, led to the emergence of concepts such as "cardiorenal anemia syndrome" and later "cardiorenal continuum". In recent years, the terms "cardiorenal" or "renocardial syndrome" have emerged. This is a syndrome caused by the effect of different pathogenesis factors on the development of the disease in a common mechanism [8,9].The modern classification of cardiorenal syndrome was adopted at the World Congress of Nephrology (Acute Dialysis Quality Initiation) held in Venice in September 2008.According to it, 5 types of CRS are distinguished:Type 1. Acute cardiorenal syndrome: - acute heart failure leads to impaired kidney function.Type 2. Chronic cardiorenal syndrome: - chronic heart failure leads to the development of renal failure.Type 3. Acute renocardial syndrome: - acute heart failure occurs as a result of acute renal failure.Type 4. Chronic renocardial syndrome: - in which chronic heart failure develops due to chronic kidney disease.Type 5. Secondary cardiorenal syndrome: - systemic diseases cause the development of cardiorenal syndrome [8,10].The Framingham Study found that cardiovascular risk factors (age, body mass index, diabetes, smoking, hypertension) contribute to the development of primary signs of renal failure [3].In addition to participating in the pathogenesis of arterial hypertension (AH), the kidneys are also considered as a target organ in the disease. AH simultaneously affects the cardiovascular system and kidney function as target organs. In hypertension, the dysfunction of the heart and kidneys exacerbates each other's damaging processes. This causes interdependent development of chronic cardiorenal and chronic renocardial syndromes. For the stratification of patients with acute and chronic renal dysfunction, the most common biological markers measured in plasma and urine are creatinine, glomerular filtration rate (GFR), and albuminuria [1,6,7]. Of these markers, creatinine and urea lead to contractile damage to cardiomyocytes and increase oxygen demand [5]. Uric acid is considered to be important in the development of heart failure, atrial fibrillation, and hypertension [11]. In addition, it is known from scientific studies that creatinine levels do not adequately reflect small changes in GFR and are also influenced by various extrarenal factors, including diet, body weight, gender, age, and ethnic differences [4].As a result of the drying up of the Aral Sea, many salty compounds of calcium, sodium, and chlorine minerals, which are toxic for the body, are spreading into the environment.There is a direct relationship between high dietary salt intake, including sodium accumulation in the body, and high blood pressure [2]. Currently, AH and its salt-sensitive type are widespread in the population of the Aral Sea region, which is considered an ecological disaster.In patients with AH in the Aral Sea population, the features of the development of cardiorenal syndrome in AH remain a problem that has not been scientifically studied and has not been thoroughly studied.Taking into account the above, we aimed to conduct a scientific study in the real activities of family clinics in order to study the development of cardiorenal syndrome in hypertensive patients in the Aral Sea region.
2. Materials and Methods
- The scientific study was conducted in family polyclinics (FP) in the Ellikkala district medical association of Karakalpakstan. A total of 1021 patients aged 40-70 years diagnosed with hypertension at district FP were included in the study.All patients included in the study underwent laboratory-instrumental examinations.Echocardiography was performed to determine target organ damage (TOD), and ultrasound was performed to determine the intima-media thickness (IMt) of the common carotid artery and brachiocephalic artery; general clinical blood and urine tests, blood biochemical tests - creatinine, urea, fasting glucose, lipid spectrum, blood sodium (Na+), serum uric acid; urine biochemical tests - urine creatinine, urine Na+, and microalbuminuria (MAU) were performed. GFR was calculated according to the EPI formula (ml/min/1.73m2).Taste sensitivity threshold for table salt (TSTTS) was tested using the R. Henkin method by instilling a drop of a sodium chloride (NaCl) solution with increasing concentration from 0.02% to 5.12% onto the anterior third of the tongue. The test began with a low-concentration (0.02%) NaCl solution and the concentration was increased by 2 times until the patient first felt a salty taste. The threshold is defined as the amount of NaCl at which a person first experiences a salty taste. TSTTS was divided into 3 groups and analyzed: low threshold ≤0.08%, middle threshold TSTTS =0.16% and high threshold TSTTS ≥0.32%.Blood pressure of all participants included in the study was measured by the N.S. Korotkov method and physiometric examination (anthropometry, waist circumference measurement) was performed.The results of patient screening according to the modified World Health Organization (for Central Asia and the Caucasus region) PEN protocol were analyzed in district FP.Cardiovascular risk (CVR) in patients with hypertension was assessed by nursing staff and family physicians based on the PEN protocol. We analyzed the PEN protocol's calculated risk of exposure using a mobile app calculator, divided into four groups: "low risk", "medium risk", "high risk", and "very high risk".Statistical processing of the results was carried out using the Statistica 6.0 program.The main characteristics are presented as mean (M) and standard deviation (SD). The frequency of symptoms in the study group was estimated using the Pearson χ² method. The Pearson correlation test was used to determine whether there was a correlation between two quantitative indicators, as well as to assess its closeness and statistical significance. For all analyses, p values <0.05 were considered statistically significant.
3. Result and Discussion
- The average age of 1021 patients included in the study was 57.68±8.06 years, of which n=627 (61.4%) were women and n=394 (38.6%) were men. The duration of AH was 7.88±3.35 years. In order to study the effect of TOD risk factors and the nature of the development of cardiorenal syndrome, we divided patients into 2 groups according to the size of the left ventricular myocardial weight index. The first group included 511 hypertensive patients with a left ventricular myocardial weight index (LVMWI) smaller than the median. The median size of LVMWI of all patients was 166.1 g/cm2 [143.2; 198.8] was organized. The second group included 510 patients with hypertension whose mean systolic blood pressure was greater than the median systolic blood pressure. The average age of 511 hypertensive patients included in group 1 was 55.61±8.19 years, the duration of AH was 6.39±3.26 years, and the average age of 510 hypertensive patients included in group 2 was 59.76±7.36 years, the duration of AH was 9.39±2.72 years (corresponding respectively, p1=0.0001; p2=0.0001). Of the patients in group 1, 191 (37.4%) were men and 320 (62.6%) were women, while of the patients in group 2, 203 (39.8%) were men and 307 (60.2%) were women.In patients of group 1, systolic arterial pressure (SAP) was 159.12±11.32 mm.Hg, diastolic arterial pressure (DAP) was 93.58±5.69 mm Hg, average arterial pressure (AAP) was 115.43±7.02 mm Hg, and SAP in patients in group 2 178.69±17.26 mm Hg, DAP 105.06±10.16 mm Hg, AAP 129.6±12.15 mm Hg, significantly different from patients in group 1 (respectively, p1=0.0001; p2=0.0001; p3=0.0001). The heart rate (HR) in patients in the first group was 79.76±5.99 beats/min, and in patients in the second group it was 88.39±5.52 beats/min (р1=0.0001).Differences between groups according to levels of AH are as follows, that is, 150 patients in group 1 have 1st level of AH, 326 have 2nd level of AH, and 35 have 3rd level of AH, and 9 patients of group 2 have 1st level of AH, 232 have 2nd level, 269 have grade 3 AH was observed (respectively, p1=0.0001; p2=0.0001; p3=0.0001).Body weight index (BWI) was equal to 29.01±4.79 kg/m2 in group 1 patients, and 30.72±5.61 kg/m2 in group 2 patients (p=0.0001). There were no significant differences between the groups in the prevalence of the first and third degrees of obesity, but the second degree of obesity was observed to be more common in group 2 patients (p=0.0001).Of the patients in group 1, 22 had coronary heart disease (CHD), 20 had type 2 diabetes mellitus (DM), and of the patients in group 2, 138 had CHD and 96 had DM (respectively, p1=0.0001; p2=0.0001).It was found that 12 patients belonging to the second group have post-infarction cardiosclerosis (PICS) and post-acute cerebrovascular accident (PACA). In group 1, there were no patients with such complications.When analyzing the PEN protocol for CVR, it was observed that 92 patients in group 1 had low CVR, 270 patients had moderate CVR, 138 patients had high CVR, and 11 patients had very high CVR. Also, in group 2, 1 patient had low CVR, 27 patients had moderate CVR, 239 patients had high CVR, and 243 patients had very high CVR (respectively, χ²1=97.77, p1=0.0001; χ²2=279.7, p2=0.0001; χ²3=43.21, p3=0.0001; χ²4=282.68, p4=0.0001).Persuasive differences between groups were also observed in comorbidity of anemia, including 77 patients in group 1 with grade 1 anemia, 3 patients with grade 2 anemia, 291 patients in group 2 with grade 1 anemia, and 85 patients with grade 2 anemia (respectively, χ²1=195.23, p1=0.0001; χ²2=83.79, p2=0.0001). Hemoglobin content was equal to 125.49±8.26 g/l in patients belonging to group 1, and 107.76±14.12 g/l in patients belonging to group 2 (p=0.0001).The results of laboratory-instrumental analysis of patients are shown in table 1.
|
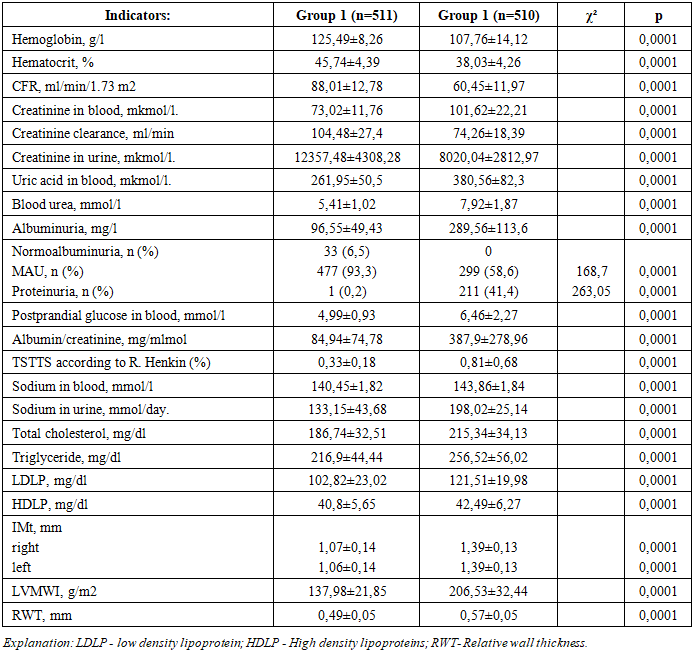
4. Conclusions
- For the first time, a large-scale scientific study was conducted to study the characteristics of the development of cardiorenal syndrome in patients with salt-sensitive AH in the Aral Sea population. The results of our study showed that in patients with salt-sensitive hypertension in the Aral Sea region, cardiovascular and renal dysfunction develop in an interdependent manner.Patients with pronounced cardiovascular remodeling have been found to have elevated renal markers: blood creatinine, urea, uric acid, and MAU. It was also observed that patients with high LVH had low CFR.It was found that cardiorenal syndrome in patients with salt-sensitive AH in the Aral Sea region is due to the interrelated development of cardiac and renal dysfunction.The results of the study suggest that patients with salt-sensitive arterial hypertension in the Aral Sea region should be treated with both cardioprotective and nephroprotective therapy.The results of this study will be a basis for effective prevention and treatment of salt-sensitive AH and its complications.