-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4272-4278
doi:10.5923/j.ajmms.20251512.16
Received: Nov. 11, 2025; Accepted: Dec. 2, 2025; Published: Dec. 8, 2025

Comprehensive Prevention of Dental Complications in Patients with Chronic Kidney Disease and After Transplantation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSabirov Maksud Atabaevich1, Akbarov Avzal Nigmatullaevich1, Shoakhmedova Komola Nazrullaevna2
1Doctor of Medical Sciences, Professor, Tashkent State Dental Institute, Tashkent, Uzbekistan
2Doctoral Student, Tashkent State Dental Institute, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic kidney disease (CKD) is accompanied by significant changes in the oral mucosa and periodontium, including gingivitis, gingival hyperplasia, candidiasis, dental hypersensitivity, and aphthous stomatitis. These complications reduce the effectiveness of dental rehabilitation and worsen patients' quality of life. The study included 320 patients divided into groups: kidney transplant recipients, patients on hemodialysis, patients with CKD without replacement therapy, and a control group. The developed prevention program included personalized selection of oral hygiene products (toothbrushes, toothpastes, mouthwashes, dental flosses), professional dental cleaning, and regular check-ups every 1-3 months. After just 2 weeks, a significant decrease in the frequency of inflammatory complications was observed: elimination of severe forms of gingivitis, a reduction in gingival bleeding by more than 60%, a 2-3 fold decrease in the severity of hypersensitivity, and an improvement in OHI-S and PMA indices (p<0.05). The most pronounced effect was observed in patients with CKD without replacement therapy, while the least effect was seen in patients on hemodialysis, indicating a need for more frequent monitoring of this category. The program's economic efficiency was demonstrated by a ~30% reduction in dental treatment costs due to a decrease in the number of complications and repeat visits. Thus, the implementation of comprehensive preventive measures in patients with CKD improves the medical effectiveness of dental care, promotes social adaptation, and offers proven economic benefits.
Keywords: Chronic kidney disease, Kidney transplantation, Hemodialysis, Dental rehabilitation, Oral mucosa, Periodontium, Prevention, Individualized hygiene therapy, Gingivitis, Dental hyperesthesia
Cite this paper: Sabirov Maksud Atabaevich, Akbarov Avzal Nigmatullaevich, Shoakhmedova Komola Nazrullaevna, Comprehensive Prevention of Dental Complications in Patients with Chronic Kidney Disease and After Transplantation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4272-4278. doi: 10.5923/j.ajmms.20251512.16.
Article Outline
1. Introduction
- In recent decades, kidney transplantation has become the gold standard for treating end-stage chronic kidney disease (CKD), not only significantly extending patients' lives but also improving their quality of life. Advances in surgical techniques and the development of immunosuppressive therapy have led to an increase in the number of recipients with good functional transplant status who require comprehensive medical and dental rehabilitation. [9]However, therapy with immunosuppressants (glucocorticoids, cyclosporine, tacrolimus, mycophenolates, etc.) is accompanied by the development of a wide range of complications, among which changes in the oral mucosa occupy a special place. In dental practice, patients after kidney transplantation often experience chronic recurrent aphthous stomatitis, candidal infections of the mucous membrane, cyclosporine-induced gingival hyperplasia, xerostomia associated with medication side effects, and secondary bacterial and viral infections. [7]Disorders of the oral mucosa not only cause pronounced discomfort (pain, burning sensation, difficulty eating) but also significantly worsen the quality of life, affecting the nutritional status and psychological well-being of patients. [17]Moreover, inflammatory and infectious processes in the oral cavity of immunosuppressed patients can serve as an entry point for systemic complications, posing a threat to both health and graft survival. [1,5]An important aspect is the presence of concomitant somatic diseases in this category of patients - arterial hypertension, diabetes mellitus, anemia, osteoporosis - which exacerbate dystrophic changes and impair mucosal repair processes. [2,14]All this creates a unique clinical picture, necessitating the development of specialized approaches to the prevention and treatment of oral mucosal lesions.Despite numerous studies on transplantology and nephrological aspects of therapy, the dental care of kidney transplant recipients remains insufficiently explored. Existing recommendations are fragmentary and fail to account for the complex effects of immunosuppression, changes in microbiocenosis, and local immune responses of the mucous membrane. [3,15]The absence of standardized treatment and prevention protocols results in a high recurrence rate of inflammatory and infectious diseases of the oral cavity in this patient group. [2,18]Several authors note that poor dental health in patients with chronic kidney disease (CKD) contributes to the progression of systemic complications. [6] Therefore, for CKD patients scheduled for kidney transplantation, it is especially crucial to rule out the presence of odontogenic infection foci. [10,20]Nevertheless, dental treatment and preventive measures for this patient category often do not receive priority attention amid more pressing medical issues related to their overall health status. [8]Moreover, ongoing renal replacement therapy (RRT) does not fully resolve the pathological processes in the oral cavity and may even exacerbate them in some cases. [10,19]The lack of proper oral care in patients after kidney transplantation is considered a risk factor for developing complications, including graft rejection. [11,16]Overall, this can negatively impact the prognosis of the underlying disease and transplantation outcomes. [12] In this context, dental rehabilitation aimed at improving oral health and reducing the risk of CKD complications becomes particularly important.Thus, research aimed at evaluating the effectiveness of various treatment methods for oral mucosa lesions in patients after kidney transplantation is relevant and in demand. Its results will allow for: optimization of dental care for transplant recipients, reduction of infectious complication risks, improvement of patients' quality of life and overall rehabilitation, and indirectly increasing graft survival.Research objective. To improve the effectiveness of oral hygiene care for patients with chronic kidney disease compared to traditional management in orthopedic treatment with partial removable dentures.
2. Materials and Methods of Research
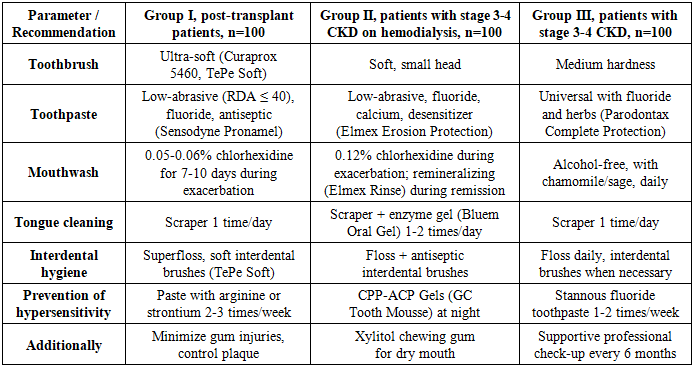
- The study included 320 patients (100 kidney transplant recipients, 100 patients on hemodialysis, 100 patients with stage III-IV CKD without replacement therapy, and 20 people in the control group). All patients underwent dental examination using OHI-S, PMA, and TMI indices. The main group received a comprehensive prevention program, including professional oral hygiene every 3 months, individual selection of toothbrushes, toothpastes, mouthwashes, and flosses, training in tooth brushing techniques, and regular monitoring every 1-3 months. Comparative effectiveness was assessed after 2 weeks, 1, 3, and 6 months. Statistical data analysis was performed using Student's t-test and analysis of variance (ANOVA), with p<0.05 considered statistically significant.Taking into account the research data, an individualized prevention and maintenance therapy program was developed, adapted to the specific oral cavity conditions of each patient category. The development of recommendations considered the degree of inflammatory changes, the level of microbial contamination, the severity of hypersensitivity, and functional limitations due to nephrological status.
|
3. Results and Discussion
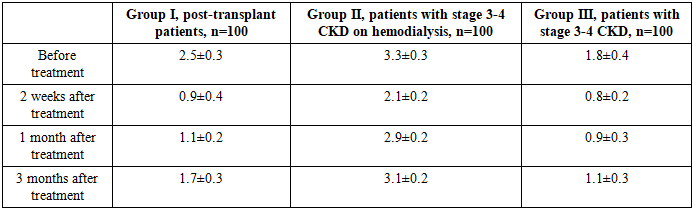
- The following presents the dynamics of changes in oral hygiene status in patients with periodontitis in two groups (comparison group and main group) based on the Green-Vermillion Oral Hygiene Index - Simplified (OHI-S) at different time intervals during treatment.At the initial stage of the study upon admission, no cases of good oral hygiene were recorded in patients of all three groups (OHI-S≤1.2). In group I, consisting of kidney recipient patients receiving immunosuppressive therapy, satisfactory oral hygiene was observed in 31.0% of patients with an average value of 1.7±0.4, while poor hygiene was noted in 69.0% - 4.7±0.3. Compared to group III, the proportion of patients with poor hygiene in group I was 30.2% higher, and compared to group II, it was 23.3% lower. In group II, comprising patients with chronic kidney disease undergoing programmed hemodialysis, satisfactory hygiene was recorded in only 10.0% of patients with an average OHI-S value of 2.8±0.3 for the group, while 90.0% had poor hygiene (5.5±0.2), which is the highest indicator among all three groups. In group III, satisfactory hygiene was most prevalent, observed in 47.0% of patients with an average OHI-S score of 1.1±0.3 for the group, while poor hygiene was found in 53.0% (5.1±0.2).Two weeks after the start of treatment, a significant improvement in oral hygiene was observed in all groups, with no cases of poor hygiene recorded. In group I, the proportion of patients with good hygiene reached 85.0%, with an average OHI-S value of 0.7±0.2 for the group, which is 54.0% higher than the initial level. Satisfactory hygiene was maintained in 15.0% of patients, with an average OHI-S value of 1.5±0.4 for the group. In group II, the indicator of good hygiene was 70.0%, with an average OHI-S value of 1.0±0.3 for the group, which is 60.0% higher than the initial value. However, compared to group I, this indicator was 17.6% lower, and compared to group III, it was 22.2% lower. Group III showed the highest proportion of patients with good hygiene - 90.0%, with an average OHI-S value of 0.9±0.2 for the group, which is 43.0% higher than the baseline.Thirty days after the start of treatment, further improvement in indicators was noted in all three study groups, with no cases of poor hygiene observed. In group I, the proportion of patients with good hygiene reached 95.0%, with an average OHI-S value of 0.8±0.3 for the group, which is 64.0% higher than the value obtained upon admission. Satisfactory hygiene was recorded in only 5.0% of patients, with an average OHI-S value of 1.8±0.4 for the group.In group II, 95.0% of cases demonstrated good hygiene with an average OHI-S value of 0.9±0.4 for the group, which is 85.0% higher than the initial level. The remaining 5.0% of cases showed satisfactory hygiene with an average OHI-S value of 2.3±0.3 for the group. These indicators were similar to group I and only slightly lower than the values obtained in group III. As for patients in group III, they achieved a 100% rate of good hygiene level with an average OHI-S value of 1.0±0.3 for the group, which is 53.0% higher than the initial level.By the end of the 90th day, there was a slight decrease in the proportion of patients with good hygiene compared to the study conducted 1 month after treatment; however, the indicators remained significantly better than the initial ones. In group I, good hygiene was maintained in 78.0% of patients with an average OHI-S value of 1.1±0.2 for the group, which is 47.0% higher than the initial level. Satisfactory hygiene was noted in 22.0% with an average OHI-S value of 2.5±0.3 for the group. In group II, the proportion of patients with good hygiene was 67.0% with an average OHI-S value of 1.1±0.3 for the group, which is 57.0% higher than the initial level. However, compared to group III, this indicator was 18.3% lower, and compared to group I, it was 14.1% lower. Satisfactory hygiene was recorded in 33.0% with an average OHI-S value of 2.9±0.2 for the group. In group III, good hygiene was observed in 82.0% of patients with an average OHI-S value of 0.9±0.2 for the group, which is 35.0% higher than the initial value, while satisfactory hygiene was noted in 18.0% with an average OHI-S value of 2.7±0.3 for the group.Comprehensive treatment and oral hygiene education for patients with chronic kidney disease (CKD) lead to significant improvement in oral hygiene status in the short term (p<0.05 for all groups). The highest and most stable result was observed in group III (conservative treatment), which is associated with less pronounced systemic disorders. Patients in group II require more frequent maintenance procedures (at intervals not exceeding 1-1.5 months) to maintain the achieved level of oral hygiene. For group I, it is necessary to consider the effects of immunosuppression and an increased risk of inflammatory complications when planning preventive visits.Assessment of the K. Kojima index to determine the degree of tongue coating in patients across study groups before treatment showed the following results. In group I, consisting of kidney recipients receiving immunosuppressive therapy, 43.0% of patients had a thick layer of coating covering less than 1/3 of the tongue surface, while 47.0% had a thin layer of coating covering more than 2/3 of the tongue surface, totaling 90.0% of patients. This indicates the presence of significant coating, more often in the form of a thin layer covering more than one-third of the tongue. Thick coating covering more than 2/3 of the tongue surface was observed in 10.0% of patients. No cases of minimal tongue coating were detected.The most unfavorable picture was observed in patients of group II with stage 3-4 CKD who were undergoing regular hemodialysis. In 60.0% of these patients, more than 2/3 of the tongue surface was covered with a thin layer of coating, and in 16.0%, more than 2/3 of the tongue surface was covered with a thick layer of coating, totaling 76.0% with heavy tongue coating. A thin layer of coating covering less than 2/3 of the tongue surface was found in 24.0% of patients. This indicates a high degree of microbial contamination of the tongue, associated with dryness of the mucous membrane, uremic coating, and a decrease in the self-cleaning function of the oral mucosa.In patients of group III with stage 3-4 CKD receiving therapeutic treatment, a more favorable picture was observed - in 14.0% of patients, a thin layer of coating was detected covering less than 1/3 of the tongue surface; in 56.0%, a thick layer of coating covered less than 1/3 of the tongue surface; in 22.0%, more than 2/3 of the tongue surface was covered with a thin layer of coating; and only in 8.0%, more than 2/3 of the tongue surface was covered with a thick layer of coating.When assessing the degree of tongue coating in the study groups 2 weeks after treatment, a pronounced clinical effect was achieved in all groups - indicators with values of 3 and 4 points were completely absent. In patients of group I - kidney recipients - 96.0% of patients had minimal coating - a thin layer covering less than 1/3 of the tongue surface. In the remaining 4.0%, the coating corresponded to 2 points - a thin layer covering less than 2/3 of the surface or a thick layer covering less than 1/3 of the tongue surface. In 95.0% of patients in group II, a score of 1 was recorded, in 5.0% - 2 points, with no severe forms detected. This indicates a pronounced positive trend and almost complete elimination of the coating in a short period of time. In all patients of group III (100.0%), a score of 1 was noted, which indicates complete cleansing of the tongue from significant coating.One month after treatment, a high percentage of patients in all groups maintained minimal coating, however, some patients showed signs of more pronounced forms returning. In 90.0% of patients in group I, a thin layer of coating covering less than 1/3 of the tongue surface persisted, while in 10.0%, a thin layer of coating covering less than 2/3 of the tongue surface or a thick layer of coating covering less than 1/3 of the tongue surface was observed. In group II patients, the proportion of those with a thin layer of coating covering less than 2/3 of the tongue surface decreased to 77.0%, with 13.0% showing a score of 2, and 10.0% presenting a thin layer of coating on more than 2/3 of the tongue surface. This indicates an early recurrence of severe forms in some patients. In 94.0% of patients in group III, a thin layer of coating persisted, covering less than 1/3 of the tongue surface, while in 6.0%, a thin layer of coating covered less than 2/3 of the tongue surface. No severe forms were detected in this group.Three months after treatment, a further loss of the achieved effect was observed, especially in the group of patients with chronic kidney disease (CKD) undergoing programmed hemodialysis. Specifically, 60.0% of patients maintained a score of 1, 17.0% had a score of 2, 20.0% had a score of 3, and 3.0% had a score of 4 (thick coating on more than 2/3 of the tongue surface). Consequently, 23.0% of patients reverted to the category with a visible abundant coating on the tongue surface. In 80.0% of patients in group I, a thin layer of coating persisted, covering less than 1/3 of the tongue surface, while in 20.0%, a thin layer of coating covered less than 2/3 of the tongue surface. In 88.0% of patients in group III, a thin layer of coating remained on less than 1/3 of the tongue surface, while in 12.0%, a thin layer of coating covered less than 2/3 of the tongue surface.Prior to treatment, severe forms of plaque (3-4 points) were prevalent in patients with chronic kidney disease undergoing regular hemodialysis (76.0%), which is associated with systemic factors (uremia, mucosal dryness, weakened local defense). A two-week treatment course effectively eliminated severe forms of plaque in all groups (p < 0.05). After 1 month, the effect persisted, but patients in group II showed initial signs of severe plaque recurrence (10.0%). After 3 months, the proportion of severe plaque forms in group II reached 23.0%, while in groups I and III, no severe forms were detected. For patients with chronic kidney disease undergoing regular hemodialysis, it is necessary to reduce the interval between preventive courses to 1-1.5 months.The results of the papillary-marginal-alveolar index (PMA) assessment during the initial evaluation of gum condition revealed significant differences between the groups.In group I, consisting of kidney transplant recipients on immunosuppressive therapy, mild gingivitis was observed in 25.0% of patients, moderate in 65.0%, and severe in 10.0%. The prevalence of moderate gingivitis in this group is associated with chronic inflammation caused by local factors, such as plaque and dental calculus, and systemic factors, including immunosuppression and gingival hyperplasia. In group II, comprising patients with stage 3-4 chronic kidney disease (CKD) on programmed hemodialysis, the most severe initial gum condition was observed - mild gingivitis was found in only 1.0% of patients, moderate in 38.0%, and severe in 61.0%. The predominance of severe forms is linked to uremic intoxication, thrombocytopathy, impaired microcirculation, and mucosal dryness. In group III, consisting of patients with stage 3-4 CKD receiving therapeutic treatment, mild gingivitis was detected in 67.0% of patients, moderate in 25.0%, and severe in 8.0%, indicating a more favorable initial state compared to other groups.After 2 weeks of treatment, significant improvement in gum condition was noted in all groups, with a complete absence of severe forms of gingivitis.In group I, consisting of kidney transplant recipients on immunosuppressive therapy, mild gingivitis was detected in 87.0% of patients, and moderate gingivitis in 13.0%. In group II, comprising patients with stage 3-4 chronic kidney disease (CKD) on programmed hemodialysis, a significant decrease in the proportion of moderate and severe forms was noted; mild gingivitis occurred in 81.0% of patients, and moderate in 19.0%. In group III, consisting of patients with stage 3-4 CKD receiving conservative treatment, mild gingivitis was detected in 93.0% of patients, and moderate in 7.0%.One month after the treatment course, a high percentage of patients with mild gingivitis persisted across all groups; however, the dynamics of changes compared to the initial data revealed pronounced intergroup differences.The proportion of patients in group I with mild gingivitis increased from 25.0% to 92.0%, accompanied by a decrease in the frequency of moderate gingivitis from 65.0% to 8.0% and complete elimination of severe forms. This indicates the high effectiveness of the therapy and the stability of the achieved result after one month.In group II, mild gingivitis increased from 1.0% to 78.0%, moderate gingivitis decreased from 38.0% to 22.0%, and severe gingivitis completely disappeared. Despite a significant increase in the mild form, the result in this group was less stable: compared to the 2-week mark, a decrease in mild cases and an increase in moderate cases were observed, reflecting an early tendency towards partial recurrence of inflammation.In group III, the proportion of patients with mild severity increased by 27%, moderate severity decreased by 19%, and severe cases were completely eliminated. This group showed the greatest preservation of results, with minimal changes compared to the 2-week mark.A study conducted 3 months after treatment revealed that the treatment effect partially diminished, especially in the group of patients with stage 3-4 CKD and those on programmed hemodialysis, where severe forms of gingivitis reappeared. In group I, mild gingivitis was observed in 78.0% of patients (a 14% decrease compared to the 1-month mark), moderate in 22.0%, and no severe forms were detected. In group II, mild gingivitis was noted in 52.0% of patients, moderate in 33.0%, and severe in 15.0%. This reflects a marked regression of the achieved effect, with severe forms returning in every sixth patient in this group. The best and most stable result was observed in group III, as after 3 months, a high proportion (81.0%) of patients maintained mild gingivitis, and there was a complete absence of severe forms.Assessment of gingival bleeding in patients across study groups before treatment showed the following results.
|
4. Conclusions
- The application of the prevention program ensured a significant improvement in oral cavity condition. After 2 weeks, the main group showed a 52% (p<0.05) decrease in the PMA index, a 60-65% reduction in gingival bleeding, a 2-3-fold decrease in hyperesthesia, and an improvement in the OHI-S index by more than 40%. The greatest effectiveness was observed in patients with CKD without replacement therapy; in patients on hemodialysis, positive changes were less pronounced. In patients with CKD, inflammatory and dystrophic changes in the oral mucosa are more common than in the general population and complicate dental treatment. The developed prevention program ensures a significant improvement in dental status, reduces the frequency of complications, and enhances the quality of life of patients.