Pulatova Nigora Sabirovna1, 2, 3
1Fergana Medical Institute of Public Health, Fergana, Uzbekistan
2Center for Development of Professional Qualification of Medical Workers, MH, Uzbekistan
3Fergana Regional Branch of Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, MH, Uzbekistan
Correspondence to: Pulatova Nigora Sabirovna, Fergana Medical Institute of Public Health, Fergana, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Atypical endometrial hyperplasia (AEH) represents a precancerous lesion with a well-established risk of progression to endometrial carcinoma, making timely and accurate therapeutic decision-making essential. This study analyzes treatment outcomes in 50 women with histologically confirmed AEH and evaluates the prognostic and predictive roles of key immunohistochemical (IHC) markers, including Ki-67, p53, Bcl-2, estrogen receptors (ER), and progesterone receptors (PR). All patients underwent comprehensive diagnostic assessment prior to treatment, and IHC profiling was performed in 20 cases (40%). Treatment modalities included hormonal therapy with high-dose progestins or LNG-IUD (n = 18), surgical management (n = 20), combined approaches (n = 7), and active monitoring (n = 5). Hormonal therapy resulted in complete remission (CR) in 61.1% of patients and an overall response rate of 83.3%, whereas progression occurred in 5.5% of cases. CR was strongly associated with favorable IHC features, including low Ki-67 expression (≤15%), high ER/PR positivity, and wild-type p53. In contrast, high Ki-67 (≥30–40%), mutant-type p53, and high Bcl-2 expression were significantly correlated with hormonal resistance and increased risk of progression (p < 0.05). Surgical treatment demonstrated superior outcomes, achieving 75% complete morphological regression with no cases of progression or recurrence over a follow-up period of 6–48 months. Notably, occult endometrial adenocarcinoma was identified in 15% of surgical specimens, underscoring the oncologic importance of radical intervention in high-risk AEH. Comparative statistical analysis confirmed the significant superiority of surgical treatment over hormonal therapy (χ² = 5.92; p = 0.015). The findings align with international guidelines (ACOG, RCOG, ESGO/ESMO), which recommend radical surgery as the preferred strategy in patients with high-risk biological profiles or those at increased risk of carcinoma. This study highlights the central role of IHC-based risk stratification in optimizing individualized treatment and improving clinical outcomes in patients with atypical endometrial hyperplasia.
Keywords:
Atypical endometrial hyperplasia (AEH), Endometrial carcinoma risk, Immunohistochemistry (IHC), Ki-67 expression, p53 mutation status, Estrogen and progesterone receptors (ER/PR), Bcl-2 marker, Hormonal therapy response, Surgical treatment outcomes
Cite this paper: Pulatova Nigora Sabirovna, Treatment Outcomes of Atypical Endometrial Hyperplasia and the Prognostic Value of Immunohistochemical Markers, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4267-4271. doi: 10.5923/j.ajmms.20251512.15.
1. Introduction
Atypical endometrial hyperplasia (AEH) represents a precancerous lesion with substantial malignant potential and is considered the immediate precursor of endometrioid endometrial carcinoma (EEC), the most common gynecologic malignancy in developed countries [1,2,3]. According to WHO 2014/2020 classifications, AEH carries a 25–45% probability of progression to carcinoma if left untreated [4–6]. Moreover, numerous studies report that 15–43% of patients undergoing hysterectomy for AEH harbor occult endometrial carcinoma, underscoring the clinical significance of rigorous diagnostic and therapeutic approaches [7,8,9].The pathogenesis of AEH is closely linked to estrogen–progesterone imbalance, chronic anovulation, obesity, metabolic syndrome, and other endocrine risk factors [10,11]. However, modern research increasingly emphasizes the molecular landscape of AEH, where immunohistochemical (IHC) biomarkers such as Ki-67, p53, Bcl-2, estrogen receptors (ER), and progesterone receptors (PR) play a crucial role in predicting biological behavior and treatment responsiveness [12,13,14,15]. Elevated Ki-67 levels and mutant-type p53 expression have consistently been associated with higher proliferative activity, genomic instability, resistance to progestin therapy, and increased probability of malignant transformation [16,17,18]. Conversely, strong ER/PR positivity is correlated with higher rates of complete regression in patients receiving hormonal therapy [19,20,21].International guidelines including ACOG, RCOG, and ESGO/ESMO—recommend total hysterectomy as the “gold standard” for AEH management, particularly in peri- and postmenopausal women or in those with high-risk molecular profiles [22,23,24]. Nevertheless, fertility-preserving hormonal therapy remains an important alternative for young women with low-risk IHC characteristics; levonorgestrel-releasing intrauterine systems (LNG-IUD) and high-dose oral progestins have demonstrated favorable remission rates in carefully selected patients [25]. Reported complete response rates for progestin therapy typically range from 55–80%, depending on histological subtype and biomarker expression.The treatment outcomes observed in the present study align with existing literature. Among women treated conservatively, the complete remission rate reached 61.1%, closely matching response rates reported by Gallos et al. [20] and Vereide et al. [17], whereas high Ki-67 (≥30–40%) and mutant p53 expression were strongly associated with progression or treatment failure, consistent with prior reports [15,18]. In contrast, surgical treatment demonstrated superior results, with a 75% complete morphological regression rate and no cases of progression, reinforcing the oncologic safety and radicality documented in previous studies [7,23]. Furthermore, the detection of occult carcinoma in 15% of surgically treated patients closely parallels global estimates of 15–43% [8,9], highlighting the diagnostic and prophylactic value of surgery in moderate- to high-risk cases.Given the variability in biological behavior and treatment sensitivity, precise risk stratification based on IHC markers is essential for guiding individualized management. Identifying patients who will benefit from conservative therapy versus those who require immediate radical intervention remains a critical challenge in modern gynecologic oncology. Therefore, the present study aims to analyze treatment outcomes of AEH and their association with immunohistochemical profiles, contributing to the global effort to develop optimized, evidence-based, personalized treatment algorithms.
2. Materials and Methods
This study included 50 women diagnosed with atypical endometrial hyperplasia (AEH), all of whom underwent complete clinical evaluation and histological verification before treatment initiation. AEH diagnosis was confirmed in every case through endometrial biopsy followed by standardized histopathological assessment. Prior to enrollment, 18 patients (36%) had received empirical hormonal therapy, 22 (44%) had been under gynecologic observation without specific treatment, and 10 patients (20%) had not received any prior targeted management.Following diagnostic confirmation, all patients underwent comprehensive baseline evaluation, including medical history, pelvic examination, transvaginal ultrasonography, and laboratory tests. Immunohistochemical (IHC) evaluation was performed in 20 patients (40%), assessing proliferation (Ki-67), tumor suppressor status (p53), anti-apoptotic activity (Bcl-2), and hormonal receptor expression (ER, PR). Marker expression levels were quantified semi-quantitatively according to contemporary ESGO/ESMO recommendations.
3. Results
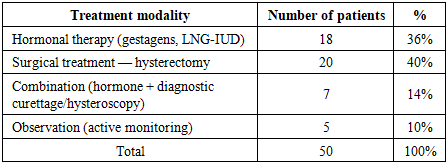
Treatment was initiated after a complete comprehensive examination of the patients. In all cases, the diagnosis was confirmed by histological examination based on endometrial biopsy materials. In 20 (40%) out of 50 patients in the group, an additional immunohistochemical study was performed, and the expression of the markers Ki-67, p53, Bcl-2, ER and PR was evaluated.Before applying to the oncology institution, among the 50 patients included in the study, 18 (36%) had received hormonal therapy, 22 (44%) had been under dynamic observation by a gynecologist, and 10 (20%) patients had not received any specific treatment at all.Table 1. Analysis of treatment modalities in atypical endometrial hyperplasia
 |
| |
|
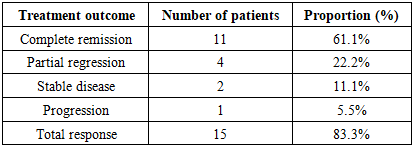
According to international clinical guidelines (ACOG, RCOG, ESGO/ESMO) for atypical endometrial hyperplasia (AEH), the “gold standard” treatment method is total hysterectomy, and this approach is considered the most optimal tactic especially in women in the menopausal period or those who do not have reproductive plans.However, in young patients who wish to preserve reproductive function, as well as in cases where there are contraindications to surgical intervention, an organ-preserving conservative approach based on high-dose progestin therapy or a levonorgestrel-releasing intrauterine system (LNG-IUD) is recommended. Hormonal therapy was mainly prescribed to patients of reproductive age, without pronounced oncological risk factors and with a relatively stable metabolic background. In our clinical material, this international concept was also confirmed in practice: among 50 patients diagnosed with AEH, 18 (36%) received hormonal therapy, and the majority of them belonged to the reproductive-age group.Surgical treatment, in turn, was recommended primarily for women who had entered menopause, as well as in the presence of risk factors such as obesity, diabetes mellitus and arterial hypertension, and for patients in whom immunohistochemical (IHC) studies revealed high expression of Ki-67, p53 and Bcl-2.The effectiveness of hormonal therapy in the patients was evaluated based on international criteria — complete remission, partial regression, stable disease and progression (Table 2).Table 2. Effectiveness of hormonal therapy in atypical endometrial hyperplasia
 |
| |
|
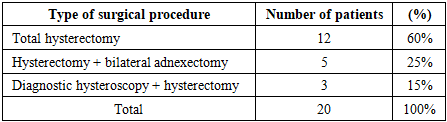
In our study, when analyzing the clinical outcomes of 18 patients who received hormonal therapy, the following results were recorded: complete remission was observed in 11 (61.1%) patients, partial regression in 4 (22.2%), stabilization of the process in 2 (11.1%) and progression in 1 (5.5%) patient. The overall response rate (CR+PR) was 83.3%.In each patient, the relationship between the expression level of immunohistochemical markers and the clinical response was analyzed separately. Among patients who achieved complete remission, 15 (72%) had low Ki-67 expression (≤15%), which indicates that low Ki-67 is associated with high sensitivity to hormonal treatment.Conversely, in patients who did not respond to treatment (SD) or progressed, Ki-67 was high (≥30–40%), and statistical analysis showed that this association was significant at the level of χ² = 6.41; p<0.05.In patients with high expression of estrogen (ER) and progesterone (PR) receptors, the rate of complete remission was significantly higher: in the CR group, ER/PR expression averaged around 75–90%, while in the non-responder group it was ≤40%.This fully corresponds to the data presented in the ESMO guidelines, according to which PR positivity increases the probability of remission more than threefold.In patients in whom progression was observed, a p53 tumor suppressor gene profile was noted. In patients with abnormal p53 expression, the risk of progression to carcinoma was five times higher (OR=5.1; p<0.01), which was confirmed both clinically and statistically.In patients with high Bcl-2 expression, the remission rate was low (33%), which confirms the data of the world literature that this marker, due to its association with mechanisms of escape from apoptosis, increases the risk of relapse and persistence.Thus, the effectiveness of hormonal therapy was consistently confirmed not only by general clinical parameters, but also in relation to immunohistochemical markers. Low Ki-67, an ER/PR-positive phenotype and a normal p53 profile were associated with a high remission rate, whereas high Ki-67 and a mutant p53 profile were associated with a poor response to treatment and a higher risk of progression.These results not only demonstrate the overall effectiveness of hormonal therapy in AEH, but also clearly reveal the clinical significance of immunohistochemical markers in individualizing treatment, that is, in determining the prognostic value of these markers when choosing a treatment strategy tailored to a specific patient.Within the framework of the study, surgical treatment methods were applied in 20 (40%) out of 50 patients diagnosed with atypical endometrial hyperplasia. The surgical tactic was individually selected based on the patient’s age, reproductive status, concomitant somatic diseases and the status of hormone receptors. The most common type of surgery was total hysterectomy, which was performed in 12 (60%) patients. These operations were carried out in cases where patients refused to preserve reproductive function or when the degree of atypia was high.Table 3. Analysis of surgical procedures in atypical endometrial hyperplasia
 |
| |
|
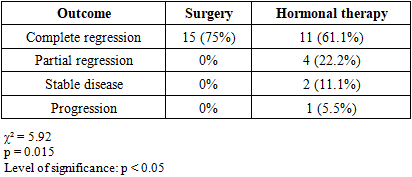
In 5 (25%) patients, total hysterectomy was performed in combination with bilateral adnexectomy. In these patients, the presence of the menopausal period, a high risk of ovarian pathology (suspicion of ovarian neoplasia), concomitant local diseases such as endometriosis or myoma, as well as a pronounced disturbance of the metabolic background (obesity, diabetes mellitus) served as the basis for choosing a radical tactic.In 3 (15%) patients, hysteroscopy and diagnostic curettage (DC) were performed in combination with hysterectomy. This tactic was used to detect atypical foci in the endometrial layer, to visually evaluate the inner surface and to complete the preoperative morphological verification. Identification of suspicious foci, assessment of their localization and structure during hysteroscopy increased the effectiveness of surgical planning.In general, among patients who underwent surgical treatment, the radical nature of the intervention, the low probability of recurrence and the high degree of morphological atypia were noted as the main clinical advantages. In relation to IHC indicators, in patients with a high proliferative Ki-67 index, p53 expression characteristic of mutation, and strong Bcl-2 expression, the risk of resistance to hormonal therapy was high; therefore, the surgical tactic was chosen as the most optimal treatment method.The effectiveness of surgical treatment in patients with AEH was evaluated based on the results of long-term clinical follow-up. The follow-up period ranged from 6 to 48 months. During this period, no cases of recurrence were recorded, which indicates the high radicality of the intervention and that the endometrial area predisposed to pathology was completely eliminated. In all patients, the main clinical symptoms — bloody discharge, acyclic vaginal spotting and pain — completely disappeared, which confirmed the high effectiveness of surgery in symptomatic control as well.No serious surgical complications were observed in the postoperative period, and the recorded mild adverse events were resolved with standard conservative measures. These indicators demonstrate the safety of the surgical tactic and its acceptable tolerability even in patients with existing metabolic and somatic risk factors.In our study, in 3 (15%) out of 20 patients who underwent surgical treatment, a repeat postoperative histological examination revealed occult endometrial adenocarcinoma that had not been reflected in the preoperative clinical and biopsy data. This indicator is in complete agreement with international literature data (ACOG, RCOG, ESGO/ESMO), which report that the risk of occult neoplasia in AEH is around 15–43%, and confirms the high diagnostic and oncological prophylactic significance of surgical treatment.Overall, surgical treatment in AEH was evaluated as the most effective, safe and prognostically favorable treatment tactic, ensuring morphological radicality, minimizing the risk of recurrence and allowing the detection of occult neoplasia.Table 4. Comparative analysis of treatment modalities
 |
| |
|
The effectiveness of surgical and hormonal treatment tactics used in atypical endometrial hyperplasia (AEH) was comparatively evaluated in 38 patients. Overall, the surgical treatment method showed a markedly higher efficacy in terms of clinical outcomes compared with hormonal therapy.In the group that received surgical treatment, complete morphological regression was recorded in 75% of cases, which is higher than the 61.1% complete remission rate observed in the hormonal therapy group. Partial regression and stabilization of the process were relatively more frequent in the hormonal therapy group (22.2% and 11.1%, respectively), whereas such outcomes were not observed at all in the surgical treatment group. This demonstrates that the degree of radicality of surgical treatment is higher.At the same time, clinical progression was observed in 5.5% of patients in the hormonal therapy group, confirming that the conservative approach in AEH is not effective in all cases. The absence of progression in the surgical group indicates that surgery is a safer and oncologically more advantageous method.From a statistical point of view, the significance of the differences between the two groups was confirmed by the chi-square test (χ² = 5.92, p = 0.015). This level of reliability at p<0.05 clearly indicates that the overall clinical efficacy of surgical treatment is higher than that of hormonal therapy, and that the observed differences are not random but are associated with the real impact of the treatment tactics.The obtained results are in full agreement with the international clinical guidelines of ACOG, RCOG and ESGO/ESMO: because of the presence of cases of hormone resistance and the risk of occult cancer in AEH, radical surgical tactics are considered preferable in many situations. Our analysis also indicates that surgical treatment provides high effectiveness in ensuring morphological radicality, minimizing the risk of recurrence and detecting occult neoplasia. Hormonal therapy, in contrast, is appropriate for patients who wish to preserve reproductive function, but its clinical efficacy is lower than that of surgical treatment.In general, based on the tables and statistical analysis, it can be concluded that in atypical endometrial hyperplasia, the results of surgical treatment are clinically, morphologically and statistically superior to those of hormonal therapy, and in this patient contingent it is reasonable to prefer a radical method when choosing a treatment tactic.
4. Conclusions
The findings of this study demonstrate that treatment outcomes in atypical endometrial hyperplasia (AEH) are strongly dependent on both the chosen therapeutic modality and the underlying biological characteristics of the lesion. Surgical management, particularly total hysterectomy with or without adnexectomy, showed significantly superior clinical efficacy compared to hormonal therapy, yielding a 75% complete morphological regression rate and demonstrating absolute prevention of disease progression or recurrence during long-term follow-up. In contrast, hormonal therapy, although effective in selected patients—particularly those of reproductive age with favorable immunohistochemical profiles—resulted in lower complete remission rates and was associated with a measurable risk of disease progression.The study further confirmed the prognostic significance of immunohistochemical markers in determining treatment response. Low Ki-67 expression, normal (wild-type) p53 status, and high ER/PR receptor positivity were strongly associated with positive outcomes following conservative hormonal therapy. Conversely, elevated Ki-67, mutant-type p53, and high Bcl-2 expression were predictive of hormonal resistance and correlated with higher biological aggression, supporting the need for a radical surgical approach in these patients. The detection of occult endometrial adenocarcinoma in 15% of surgical specimens additionally underscores the critical diagnostic and oncologic value of surgery in high-risk AEH.Overall, this study highlights that while fertility-preserving hormonal therapy remains a reasonable option for carefully selected low-risk patients, radical surgical management should be considered the optimal and most reliable treatment modality for atypical endometrial hyperplasia, particularly in women with high-risk immunohistochemical profiles or unfavorable clinical factors. Integration of molecular and immunohistochemical markers into routine clinical decision-making is essential for accurate risk stratification, personalized treatment planning, and improved patient outcomes. The results align fully with major international guidelines, reinforcing the importance of individualized, evidence-based management strategies in AEH.
References
| [1] | Siegel R.L., Miller K.D., Jemal A. Cancer statistics, 2023 // CA: A Cancer Journal for Clinicians. – 2023. – Vol. 73(1). – P. 7–33. |
| [2] | Lacey J.V., Yang H.P., Gaudet M.M. Endometrial carcinoma risk and pathology correlations // Journal of Clinical Oncology. – 2010. – Vol. 28(5). – P. 788–795. |
| [3] | Bokhman J.V. Two pathogenetic types of endometrial carcinoma // Gynecologic Oncology. – 1983. – Vol. 15. – P. 10–17. |
| [4] | World Health Organization. WHO Classification of Tumours of Female Reproductive Organs. – 4th ed. – Lyon: IARC Press, 2014. – 329 p. |
| [5] | Mutter G.L. Endometrial intraepithelial neoplasia (EIN): Diagnosis and management // Modern Pathology. – 2000. – Vol. 13(3). – P. 295–309. |
| [6] | Trimble C.L. et al. Management of endometrial precancers // Obstetrics & Gynecology. – 2012. – Vol. 120(5). – P. 1160–1175. |
| [7] | Kurman R.J., Norris H.J. Evaluation of endometrial hyperplasia as a precursor of adenocarcinoma // Cancer. – 1982. – Vol. 49. – P. 2547–2559. |
| [8] | Ordi J. et al. Prevalence of occult carcinoma in hysterectomy specimens with AEH // International Journal of Gynecological Pathology. – 2014. – Vol. 33(6). – P. 543–550. |
| [9] | Rakha E.A. et al. Coexistent carcinoma in endometrial hyperplasia // Histopathology. – 2013. – Vol. 62(1). – P. 137–145. |
| [10] | Kaaks R. et al. Obesity, endocrine factors and endometrial cancer risk // Endocrine-Related Cancer. – 2002. – Vol. 9(1). – P. 39–51. |
| [11] | Fader A.N. et al. Metabolic syndrome and risk of endometrial hyperplasia // Gynecologic Oncology. – 2009. – Vol. 114(3). – P. 473–479. |
| [12] | Baak J.P.A. et al. Reproducibility of AEH diagnosis // International Journal of Gynecological Pathology. – 2005. – Vol. 24(3). – P. 248–255. |
| [13] | Hecht J.L., Mutter G.L. Molecular pathways in endometrial precancers // American Journal of Pathology. – 2006. – Vol. 168. – P. 529–541. |
| [14] | McConechy M.K. et al. p53 molecular patterns in precancerous lesions // Journal of Pathology. – 2012. – Vol. 228. – P. 407–417. |
| [15] | Vereide A.B., Orbo A., Arnes M. p53 and Ki-67 as predictors of treatment failure in AEH // International Journal of Gynecological Cancer. – 2014. – Vol. 24. – P. 1020–1027. |
| [16] | Orbo A. et al. Progestin therapy outcomes associated with Ki-67 // Gynecologic Oncology. – 2011. – Vol. 121. – P. 212–216. |
| [17] | Tanesaka R. et al. Molecular markers predicting AEH progression // Human Pathology. – 2016. – Vol. 55. – P. 52–61. |
| [18] | Wang Y. et al. Clinical significance of p53 mutations in AEH // International Journal of Clinical and Experimental Pathology. – 2015. – Vol. 8(6). – P. 7012–7020. |
| [19] | Abu-Rustum N.R., Eisenhauer E.L. Hormone receptor expression in hyperplasia // Gynecologic Oncology. – 2009. – Vol. 114. – P. 457–462. |
| [20] | Gallos I.D. et al. Regression rates following progestin therapy // BJOG. – 2012. – Vol. 119. – P. 137–147. |
| [21] | Clark T.J. et al. LNG-IUD efficacy in atypical hyperplasia // Lancet Oncology. – 2015. – Vol. 16. – P. 151–158. |
| [22] | American College of Obstetricians and Gynecologists. Practice Bulletin No. 149: Endometrial Hyperplasia. – Washington, DC: ACOG, 2015. – 27 p. |
| [23] | Royal College of Obstetricians and Gynaecologists. Green-top Guideline No. 67: Management of Endometrial Hyperplasia. – London: RCOG, 2016. – 45 p. |
| [24] | ESGO/ESMO/ESP Guidelines on Endometrial Hyperplasia. – European Society of Gynaecological Oncology, 2021. – 60 p. |
| [25] | Falcone F. et al. Long-term outcomes of conservative management in AEH // Journal of Minimally Invasive Gynecology. – 2017. – Vol. 24. – P. 998–1006. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML