Abdusalomov Mukhammadyusufkhuja Abdujabbor ogli, Turaev Feruz Fatkhullaevich
Republican Specialized Scientific and Practical Medical Center for Surgery named after Academician V. Vakhidov, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article presents a comparative analysis of the long-term clinical outcomes of the mitral valve after plasticity and prosthetics operations. The study involved 60 patients who underwent surgery between 2010 and 2023: 30 who underwent valve-retaining plasticity and 30 who underwent pastprophilic mechanical prosthetics. Clinical, instrumental and laboratory indicators of patients, quality of life (SF-36, MLHFQ), as well as the frequency of special complications (thromboembolism, bleeding, prosthetic dysfunction, infectious processes) were evaluated. The study examined the effects of routine dispensary follow-up on long-term outcomes. The results showed that regular follow–up leads to decreased thromboembolic and infectious complications in patients, higher survival rates, stable maintenance of the functional class (NYHA I-II), and improved labour return rates. According to Kaplan–Meier and multi-factor regression analysis, nonspecific observation has been identified as an independent enhancing factor for the risk of complications. The results obtained confirm the strategic importance of the dispensary monitoring system in improving long-term outcomes after mitral valve operations and improving the quality of life of patients.
Keywords:
Mitral valve, Plastics, Prosthetics, Pastprophilic mechanical valves, Dispensary monitoring, Thromboembolic complications, Prosthetic dysfunction, Infectious endocarditis, Rehabilitation, Quality of life
Cite this paper: Abdusalomov Mukhammadyusufkhuja Abdujabbor ogli, Turaev Feruz Fatkhullaevich, Ways to Assess the Quality of Life and Improve Long-Term Results After Heart Valve Operations, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4748-4753. doi: 10.5923/j.ajmms.20251512.120.
1. Introduction
Surgical treatment of heart valves in modern cardiology is one of the most important ways to save lives and improve the patient's quality of life. Numerous studies show that long-term results after surgery depend not only on the method of operation, but also on the patient's rehabilitation, as well as the effectiveness of the dispensary monitoring system [1-4,7,10,15]. The number of patients living with artificial valves in the world is increasing every year. At the same time, studies showing the benefits of mitral and aortal valve plastic are also increasing [5,6,8,9,17]. Unfortunately, the basic principles, advantages and methods of Valve reconstruction operations were introduced in 1983 by Carpentier A. although developed by, many newly established non-specialized cardio centers have little valve maintenance operations [11-14,16]. Therefore, determining the importance of quality of life, level of rehabilitation and dispensary control after reconstructive operations – today is an urgent scientific and practical task.The purpose of the study is valves study long-term clinical course and quality of life of patients after plasticity and prosthetics operations, identify specific risk factors, assess the effectiveness of the dispensary monitoring system, and develop an advanced algorithm.
2. Materials and Methods
This study included 60 patients who underwent mitral valve surgery between 2010 and 2023. They were divided into two groups based on the type of operation performed: 30 patients were fitted with mitral valve plasticity practice (valve holder operation), and 30 patients with low-profile disc mechanical prostheses (ATS, SJM, EMA, MedEng). The age of patients ranged from 24 to 65 years, with an average age of 45.7±4.3 years. The gender makeup was 53.3% male and 46.7% female. The groups are tied in demographics.Criteria for inclusion in the study included moderate to severe mitral insufficiency (regurgitation), suitable valve morphology for plasticity (Type I–II under Carpentier classification), availability of complete documentary data on surgery, and a minimum one-year follow-up period (3.6±1.2 years on average). Patients with spherical or semi-spherical prostheses were excluded from the study.In Mitral valve plastic, methods of annulloplasty (Carpentier ring), reconstruction in the papillary choir and segmental reconstruction were used. In the pastprophilic prosthetic group, however, modern mechanical prostheses such as ATS Medical, SJM, and EMA were implanted via a transeptal or right-branch entrance. Additional pathologies included compartment xylpyrashi (63%), chronic heart failure (NYHA III–IV FS, 68%), hypertension (45%), diabetes mellitus (15%) and dyslipidemia (22%).Before the operation, all patients were given transthoracic and transesophageal exocardiography, ECG and Holter monitoring, a 6-minute walk test, SF-36 and MLHFQ questionnaires, as well as laboratory analyzes (NT-proBNP, creatinine, general blood and hormonal indicators). In the systolic function assessment, 42 of the patients (70%) had a release fraction of >55% and were assessed as having normal systolic efficiency; while 18 (30%) had a release fraction of <55%, and a reduced contraction was observed. The plasticity group included patients with higher hemodynamic indicators, while the prosthetics group included patients with higher decompensation rates.In assessing the results, the dynamics of clinical, instrumental and laboratory indicators, as well as quality of life questionnaires, were taken as a basis. Statistical analysis was performed in Microsoft Excel 2019 and SPSS Statistics 26. The Normal distribution was examined by the Kolmogorov–Smirnov test, with quantitative markers being compared to the t-test or Mann–Whitney U-test, with qualitative indicators being compared to the χ2 test. For the correlation, the Pearson and Spearman coefficients were applied. Long-term survival was evaluated by the Kaplan–Meier method, with complication and lethal factors analyzed based on the Cox proportional risk model. Statistical significance was accepted at P<0.05.
3. Results and Discussions
The long-term prognosis of patients with heart valve prosthetics is directly dependent not only on the operating technique and prosthetic model, but also on the quality of dispensary observation. Many scientific studies (Yuan et al., 2018; Iung et al., 2022; Özkan et al., 2020) noted that regular and systematic dispensary monitoring plays an important role in the quality of life of patients, timely identified complications, and their prevention.The main objectives of dispensary surveillance include:• Early diagnosis and Prevention of specific complications (thromboembolism, fistula, prosthetic dysfunction, endocarditis) that can develop against the background of Valve prostheses and plastic corrections;• Stabilization of heart failure, cardiac rhythm disturbances and hemodynamic dysbalance;• Monitoring of anticoagulant therapy, especially in patients with surgery with disc prostheses;• Strengthening the rehabilitation effect and returning patients to socially active life;• Maintain and improve quality of life indicators (on SF-36 and MLHFQ).In our analysis, two main groups were formed: patients with regular dispensary follow-up (Group I) and patients with non-specific or episodic Control (Group II). In both groups, only patients with a pastprophilic (disc) prosthesis installed on the mitral valve or who underwent mitral plasticity were included. Spherical and hemispherical prostheses were excluded from the analysis, since their use in practice today is not recommended.The dispensary surveillance system consisted of the following components:• Clinical trials: ECG, cardiac auscultation, arterial pressure monitoring;• Laboratory analyzes: general blood analysis, biochemical markers, XNN control;• Visual assessment: transthoracic and transesophageal Echo, spiroveloergometry;• Individual adjustment of drug therapy: anticoagulants, beta-blockers, cardiac glycosides, diuretics, angiotensin-converting enzyme inhibitors;• Supplement: immunocorrection, vitamins, metabolic therapy and antibiotic prophylaxis.Long-term results and patient survival rates depending on the level of dispensary observation.Long-term clinical observations indicate that the quality of dispensary control and rehabilitation measures after heart valve replacement or restoration operations is one of the main factors determining the general condition, working capacity, social integration and quality of living of patients. Especially for patients who experience pastprophilic (disc) mitral prostheses and mitral valve-retaining plastic surgeries, regular and systematic monitoring is instrumental in detecting complications in time, properly dosing anticoagulant therapy, controlling heart rhythm, and preventing heart failure.In this section, we compared groups of patients based on the regularity of the dispensary observation, evaluating long-term results according to the following criteria:• good result (no clinical symptoms or minimal, NYHA I-II, high quality of life);• satisfactory result (NYHA II-III, symptoms under control, patient adapted to active life);• unsatisfactory result (NYHA III-IV, symptoms preserved or worsened);• incomplete clinical effect (major pathology eliminated but primary goal not achieved) Table 1.Table 1. Distribution of long-term results according to the level of dispensary observation
 |
| |
|
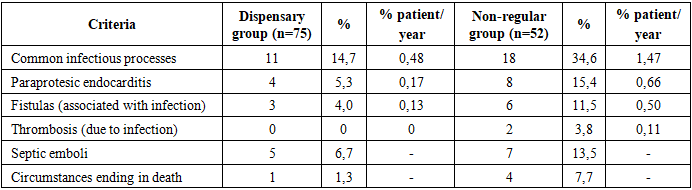
From the table above, it can be seen that in patients under regular dispensary supervision, the positive rate of long-term outcomes was statistically reliably high (p<0.0005), with a particularly good clinical outcome and quality of life index of 57.5%. Conversely, in 18.4% of patients with non-specific follow-up, the results were unsatisfactory (p<0.005). This clearly confirms the clinical significance of dispensarization. In patients with regular control, good outcome stability was maintained at levels of 80.9 ± 6.5% and 80.9 ± 6.5%, respectively, over the 5-and 10-year period, whereas in the non-specific group this rate was 20.0 ± 17.9% and 0.0% (p<0.005).The possibility of specific complications depending on the dispensary observation. Complications related to anticoagulant therapy.The regularity of dispensary control is important in the development of anticoagulant therapy-dependent complications in patients with heart valve prosthetics. In our observation groups, the total periodicity of thromboembolic syndrome was 0.95% in regularly observed patients and 1.72% in patients under non-observational observation (patient/year).A total of 22 embolic episodes were recorded in 11 patients (14.7%) in regular surveillance (dispensary group). Of these, 17 were septic embolisms and were found in 7 patients. In the remaining 5 patients, thromboembolism was associated with a violation of the anticoagulant therapy regimen. In the analysis on localization, embolisms were observed in 20 cases, central (trunk vessels of the brain) and peripheral in 2 cases (in one case, small branches of the pulmonary artery and in one case to the son artery). The clinical outcome of Central emboli was as follows: 5 patients had complete recovery, 1 patient had left-sided hemiparesis, and 3 patients had multiple, severe septic emboli, of which 2 were fatal and 1 clinically unsatisfactory.21 thromboembolic episodes were recorded in 11 patients (21.2%) in the non-randomized dispensary group. In 5 of them - septic emboli (up to 3 times each), and in 6-there was a violation of the anticoagulant therapy regimen. All emboli were centrally localized, with chronic dysculatory encephalopathy in 1 patient, stable hemiparesis in 1 patient, and complete clinical remission in 5 patients. Thromboembolism in 4 patients ended in death.Bleeding cases associated with anticoagulant therapy have been identified in a total of 6 patients: 3 in the dispensary group (0.13% bem./year), non-regular in follow - up-3 (0.25% patient/year).Of patients with regular follow-up, 2 had hypermenorrhea and nosebleeds, and the protronbin index was 33% and 40%, respectively. 1 patient had a renal hemorrhage accompanied by microgematuria with a protronbin index of 40%.In contrast, 3 patients who were under non-surveillance were found to have frequent nosebleeds in 2 cases, hypermenorrhea and microgematuria in 1 case.It should be noted that all hemorrhagic complications occurred in the first two years after surgery, during a period when anticoagulant doses were not fully adjusted. However, none of them required urgent hospitalization and phenylin was brought under control by dose correction.Prosthetic dysfunction.In long-term follow-up of patients with heart valve prosthetics, prosthetic dysfunction, especially cases of paraprothetic discharge (fistula) and thrombosis, is one of the complex complications associated with the infectious process in most cases.In the dispensary group (patients under regular dispensary surveillance), a paraprothetic fistula was detected in 10.7% of patients (n=8), which corresponds to a frequency of 0.35% patient/year. While 4 (50%) of these fistulas are associated with a long-term infectious process, 2 have evolved on the basis of pre-existing destructive valvulitis. Of these, only one was Hemodynamically significant (0.04% patient/year), while the rest had no significant effect on valve function. This patient abandoned secondary surgery, but with conservative therapy, the condition stabilized.In the non-randomized observational group (n=8), the paraprothetic fistula had a periodicity of 15.4%, equivalent to 0.66% patient/year. In 4 of these, the fistula was found to have hemodynamic significance (0.33% patient/year), with 6 cases associated with infection. It should be noted that in this group, fistulas had severe clinical consequences and required more secondary surgery.In addition, cases of thrombosis were observed only in the non - specific observation group-in 2 patients, after 7.5 and 10.5 years, respectively. Both are associated with prosthetic endocarditis. One patient had a thromboembolism death, while a second patient had successfully undergone re-surgery (Table 2).Table 2. Prosthetic dysfunction in long-term follow-up of heart valve prosthetic patients
 |
| |
|
Analytical explanation:Dysfunctions were relatively rare in patients under regular surveillance, indicating the positive efficacy of continuous dispensary surveillance and adequate anticoagulant control. In this case, early detection and treatment of infection, as well as regular control of blood clotting properties, are a decisive factor in the maintenance of prosthetic function.Whereas in patients with non-regular dispensary, prosthetic dysfunction was accompanied by more severe infectious and thrombotic processes, leading to a negative long-term clinical outcome.Paraprothetic endocarditis and infectious complications.One of the severe complications observed in the long term after heart valve replacement is prosthetic-dependent infectious processes, specifically paraprotesic endocarditis. This condition, in most cases, will be associated with secondary dysfunction, embolic syndrome and the patient's survival rate.In the dispensary group (patients with regular observation):Infectious processes were detected in 11 patients (14.7%), which was 0.48% patient/year periodicity. In 7 of these (63.6%), infection did not disrupt valve function, meaning endocarditis occurred in the form of periodic remission. The remaining 4 patients (36.4%) have developed paraprothetic endocarditis, which includes:• 3 patients developed paraprothetic fistula (in 2 cases-Hemodynamically insignificant;• 1 patient had fistula sepsis and multiple embolic syndrome with no preserved prosthetic refunction. In this case, the patient refused reoperation, the result – not satisfactory.Embolic complications, especially septic emboli, have been reported in 5 patients in this group. In 2 of them, for the last time, embolisms were numerous, accompanied by neurological decompensation.In a non-random observational group:The number of patients diagnosed with infectious processes is 18 (34.6%), compared to 1.47% per patient/year.In 10 of them, infection did not disrupt valve function, mostly occurring in the form of subclinical/remission, 8 patients (44.4%) developed paraprothetic endocarditis, among which 6 patients had a paraprothetic fistula (4 cases Hemodynamically significant), 2 patients reported prosthetic thrombosis. In 4 of the patients, these infectious complications resulted in death, and in the rest, reoperation or conservative treatment was carried out (Table 3).Table 3. Comparative indications for infectious complications
 |
| |
|
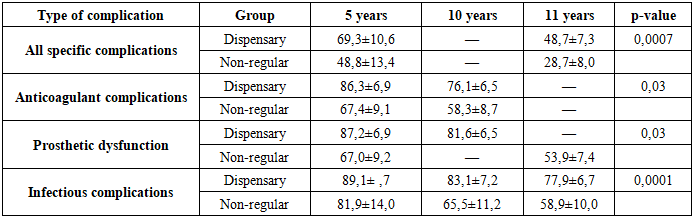
In patients with regular dispensary follow-up, infectious complications occurred in relatively few and mild forms, with the majority of cases maintaining valve function, with remission achieved. In this case, dispensary control and early antibacterial prophylaxis have become important.A notable aspect is infection in patients with nonregular follow-up:• more accompanied by impaired valve function;• paraprothetic endocarditis and sepsis-specific emboli were the majority;• high mortality rateThese differences are undoubtedly due to the lack of a dispensary control system and the complete failure of patients to follow treatment and monitoring recommendations.In long-term follow-up results, it is found that the level of actuarial release of specific complications (infectious processes, prosthetic dysfunction and thromboembolic or hemorrhagic conditions related to anticoagulant therapy) is clearly correlated with the patient's dependence on the dispensary monitoring system.According to the Kaplan–Meier survival analysis orcali calculated:• Freedom from all specific complicationso Dispensary group: 69.3±10.6% (5 years), 48.7±7.3% (11 years)o Non-regular group: 48.8±13.4 % (5 years), 28.7 ±8.0% (11 year)o sp=0.0007→statistically significant difference.• Freedom from complications related to anticoagulant therapy (thromboembolism and bleeding):o Dispensary group: 86.3±6.9% (5 years), 76.1±6.5% (10 years)o Non-regular group: 67.4 ± 9.1% (5 years), 58.3 ± 8.7% (10 years)o p=0,03.• Freedom from prosthetic dysfunction (fistula with thrombosis and paraprotesis):o Dispensary group: 87.2 ± 6.9% (5 years), 81.6 ± 6.5% (10 years)o Non-regular group: 67.0 ± 9.2% (5 years), 53.9 ± 7.4% (11 years)o p = 0,03.• Freedom from infectious complications (endocarditis, infectious dysfunction):o Dispensary group: 89.1±7.7% (5 years), 83.1±7.2% (10 years), 77.9±6.7% (11 years)o Non-regular group: 81,9±14,0% (5 years), 65,5±11,2% (10 years), 58,9±10,0 % (11 years)o p=0,0001 (Table 4).Table 4. Freedom from complications (%) according to Kaplan–Meier analysis
 |
| |
|
The results obtained show that patients with regular dispensary monitoring have a significant advantage in long-term stability and protection against complications. According to Kaplan-Meier analysis, there are statistically significant differences in all directions (p<0.05). An analysis of breast regression showed that non-specific observation is an independent risk factor that:• 2.1 times the risk of prosthetic dysfunction;• risk of infectious complications 2.4 times;• increases the risk of thromboembolic events by 1.9 times (p<0.05).Dynamics of labor recovery: a comparison of regular and non-regular dispensary observation groups.In assessing the quality of life and clinical outcomes of patients after long-term cardiac valve prosthetics or Valve-preserving (plastic) operations, it is not enough to limit yourself to studying the periodicity of survival and complications. One of the important criteria for clinical rehabilitation is the level of Return of the patient to work and the stability of work activity.In this analysis, we compared the dynamics of the restoration of the working capacity of patients, the speed and stability of their return to work in the conditions of regular dispensary observation dispensary group and non-continuous monitoring.Results: dispensary group• Group I disability — was recorded in two patients. The main cause in both is brain circulatory disorders (thromboembolism), which developed before surgery, accompanied by left-sided stable hemiparesis.• Group II disability — was in 28 patients, 12 of whom (42%) continued to engage in active labor.o 6 patients (22%) continued to work in their previous specialty (in most cases in intellectual or technical areas).o 5 patients (19%) changed their profession to lighter areas.o 1 patient started an independent business career.• Of the 16 patients who were not working, 2 were retired, but actively worked in agriculture, 1 patient (51 years of Operation time) performed large-scale physical work at home.• 8 patients did not receive re–entry into labor due to the cardiovascular system and other severe companion diseases (for example, large-focus cardiosclerosis, Stage II-III hypertension, strokes). 2 patients had an aortic valve defect added in the postoperative period.• 1 patient had incomplete correction, and another had 4 repeated thromboemboli with a lethal ending.Negative dynamics-observed in two cases. They worked for 5-10 years without disabilities, but later:1. In one patient - prosthetic endocarditis, thromboembolism and fistula of paraclapan.2. In the second - thromboembolism to the blood vessels of the brain, with stable hemiparesis.Results: non-regular observation group• Group I disability — in 1 patient (severe ischemic heart disease and double myocardial infarction).• Group II disability — in 15 patients:o 1 patient continued to work in his previous specialty;o 2 patients changed careers (i.e. 20% of Group II disabled people continued to work);o 1 patient who had the opportunity to work in the household in the village.o 11 patients did not work. Causes:§ In 4 patients-severe companion pathologies such as cardiovascular and kidney diseases;§ In 2 cases-more than three times a minute thromboembolism;§ In 3 cases - paraclapan fistula and other defects against the background of prosthetic endocarditis.§ In case 1 - disirculatory encephalopathy degree II• Negative dynamics-1 patient lost working capacity due to newly added severe companion diseases in 9 years.General comparison• The proportion of patients who did not work in the dispensary group during the long term and had a disability Group II — 17% (n=13). Of these, only in 4 cases (31%) the cause was directly related to a heart defect or the results of surgery.• In the Non-regular follow-up group, the rate was 42% (n=11), with 7 cases (64%) directly related to postoperative clinical walking and complications.These results show the strategic importance of regular dispensary surveillance in the return to labour and long-term maintenance of performance.
4. Conclusions
1. The stability of long-term outcomes (74.1% in 10 years) and survival rate (76.7% in 10 years) in patients operated on pastprophilic (disc) mitral prostheses are not significantly different from those cited in the literature on extracorporeal circulation operations. Pastprophilic prostheses provide the most favorable conditions for improving intracardial hemodynamics in all anatomical group patients at the mitral position, provide a good clinical outcome at high probability, allow functional class (I–II) storage in 81.7% of patients, and increase the functional reserve potential of the heart.2. The myocardium's ability to contract is the most important prognostic factor for long-term results following mitral valve prosthetics. Patients with normal initial contractility achieve the highest level of good outcomes in the long term - 97.5% of patients are ensured to be in the I–II functional reserve potential, their physical working capacity and overall wellness performance remain high.3. Significant influences on the periodicity of thromboembolic complications over the long term are preoperative left ventricular thrombosis or thromboembolism (3.73% patient/year), atriomegaly (3.71% patient/year), and supraventricular rhythm disturbances (3.54% patient/year). Inflammatory–destructive changes characteristic of severe Mitral valve (III–IV) calcinosis and infectious endocarditis (ulcerative–destructive valvulitis, fibrosis ring abscess) increase the likelihood of developing a paravalvular fistula (2.0% patient/year and 3.7% patient/year, group-wise overall 0.74% patient/year), as well as an increased risk of recurrence of the inflammatory process (2.12% patient/year, group-wise average 0.56% patient/year).4. Regular and active dispensary monitoring in the cardiosurgical center allows you to early identify the deterioration in the clinical condition of patients, establish its causes and correctly select the tactics of further treatment. The dispensary observation regime increases the survival rate, provides stable good clinical results in the long term, reduces the number of specific complications and, as a result, improves the dynamics of the restoration of working capacity. In such patients, the number of working and working people increases in 5 years and persists even in 10 years. In patients with nonegular follow-up, however, this rate drops consistently throughout the entire follow-up period.
References
| [1] | ACC/AHA Guidelines. Nishimura R.A., et al. 2021 AHA/ACC Guidelines for the Management of Valvular Heart Disease. J Am Coll Cardiol, 2021. |
| [2] | Baumgartner H., et al. ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J, 2021. |
| [3] | Carpentier A. The French correction of mitral valve insufficiency. J Thorac Cardiovasc Surg, 1983. |
| [4] | Carpentier A. Mitral valve repair and reconstruction. J Thorac Cardiovasc Surg, 2015. |
| [5] | Cohn L.H. Cardiac surgery in the adult. 5th edition. McGraw-Hill, 2017. |
| [6] | David T.E. Mitral valve repair experience. Ann Thorac Surg, 2010. |
| [7] | Dreyfus G.D., et al. Mitral valve repair versus replacement: Long-term follow-up. J Thorac Cardiovasc Surg, 2022. |
| [8] | Enriquez-Sarano M. Mitral valve disease: current management. Lancet, 2021. |
| [9] | Gillinov A.M., et al. Surgical management of mitral valve disease. Circulation, 2020. |
| [10] | Goldstone A.B., et al. Mechanical versus bioprosthetic mitral valve replacement: outcomes. J Am Coll Cardiol, 2020. |
| [11] | Habib G. Infective endocarditis: diagnosis and management. Lancet, 2019. |
| [12] | Ivanov Yu., et al. Long-term outcomes after mitral valve surgery. Kardiologiya, 2021. |
| [13] | Iung B., et al. Contemporary presentation and management of valvular heart disease. Eur Heart J, 2022. |
| [14] | Lancellotti P., et al. Recommendations for the echocardiographic assessment of native valvular regurgitation. Eur Heart J Cardiovasc Imaging, 2013. |
| [15] | Lorusso R., et al. Mechanical prostheses long-term quality of life. Eur J Cardiothorac Surg, 2021. |
| [16] | Masri A., et al. Anticoagulation strategies in patients with prosthetic valves. Heart, 2019. |
| [17] | Nakamura M., et al. Mitral valve prosthesis outcomes in Japan. Circ J, 2022. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML