-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4745-4747
doi:10.5923/j.ajmms.20251512.119
Received: Nov. 23, 2025; Accepted: Dec. 17, 2025; Published: Dec. 31, 2025

Evaluation of the Effectiveness of Various Methods for Correcting Sexual Dysfunction After Reconstructive Surgery for Pelvic Organ Prolapse
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDjalolova Iroda Abdujabborovna, Negmadzhanov Bakhodur Boltaevich
Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents a retrospective analysis of various methods used to correct genital prolapse in our patients over the period from 2012 to 2016. Increasingly, women of working age seek help for this condition, unwilling to accept a situation that significantly reduces their quality of life and level of social activity. The relevance of the study is reinforced by the “rejuvenation” of this pathology and the need to find the most acceptable method for its correction. Surgical, hormonal, physiotherapeutic, and psychotherapeutic methods were considered.
Keywords: Pelvic organ prolapse, Sexual dysfunction, Reconstructive surgery, Hormone therapy, Physiotherapy, Psychotherapy, Female Sexual Function Index (FSFI), Multidisciplinary approach, Quality of sexual life, Postoperative rehabilitation
Cite this paper: Djalolova Iroda Abdujabborovna, Negmadzhanov Bakhodur Boltaevich, Evaluation of the Effectiveness of Various Methods for Correcting Sexual Dysfunction After Reconstructive Surgery for Pelvic Organ Prolapse, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4745-4747. doi: 10.5923/j.ajmms.20251512.119.
1. Introduction
- Pelvic organ prolapse (POP) is a broad group of clinical conditions that affect the quality of life for millions of women worldwide. It is a polyetiological disease encompassing a range of disorders—from asymptomatic changes in vaginal anatomy to complete vaginal eversion, often accompanied by severe anal and sexual dysfunction [8], as well as stress urinary incontinence (SUI) triggered by sudden physical exertion. A significant role in the pathogenesis of POP and SUI is played by connective tissue metabolism disorders, loss of normal tone in connective tissue structures and ligaments, including those supporting the bladder neck and proximal urethra [7]. The combination of genital prolapse and urinary incontinence is one of the most common gynecological conditions, with no signs of decreasing prevalence [4]. According to global data, between 2.9% and 53% of women report some manifestation of POP [5]. Up to 47% of POP patients are women of working age [6]. The Women's Health Initiative Study, which examined 16,616 perimenopausal women, found uterine prolapse in 14.2%, cystocele in 34.3%, and rectocele in 18.6% of cases. Among women under 40, POP occurs in 26% of cases, indicating an increasing frequency in younger patients and highlighting the urgency of addressing this issue [9]. Clinically, prolapse can affect the anterior or posterior vaginal walls, the central or apical compartment, the uterus, or the vaginal vault in its absence. Anterior vaginal wall prolapse often results in cystocele and urethral hypermobility, leading to stress urinary incontinence. Posterior wall prolapse may cause rectocele—a herniation of the rectum. Many patients seek medical help when the prolapse has already reached stage III–IV according to the Pelvic Organ Prolapse Quantification (POP-Q) system [3]. Risk factors for POP development include: Predisposing factors: gender, racial differences, connective tissue weakness, vascularization, innervation. Provoking factors: pelvic floor trauma, pelvic surgery, radiation damage, traumatic childbirth. Contributing factors: pregnancy, obesity, constipation, physical exertion, respiratory diseases. Decompensating factors: age, tissue atrophy, emaciation, certain medications [10]. The risk of SUI significantly increases in women with a BMI over 30 kg/m², a history of delivering large babies vaginally, and/or hysterectomy without adnexa. Other major contributors include hereditary predisposition, heavy physical labor, hypertension treated with diuretics, osteoporosis, and obesity. A statistically significant increase in SUI risk has been observed among women with moderate undifferentiated connective tissue dysplasia (UCTD), commonly marked by joint hypermobility, dislocations, varicose veins, hemorrhoids, hernias, visceroptosis, and a family history of genital prolapse [1]. Surgical treatment—especially in severe POP—poses considerable challenges, requiring correction of the prolapse itself and restoration of pelvic anatomy and function of the genital organs, rectum, bladder, and urethra [4,9]. Perineal muscle reconstruction, especially of the m. levator ani, is essential in cases of rectocele. Surgery is recommended for moderate to severe SUI or when conservative treatment is ineffective or not possible. Modern approaches emphasize the need for innovative diagnostic methods to guide treatment decisions. The outcome of surgery depends significantly on the chosen method for correcting anatomical and functional abnormalities. Most invasive treatments for cystocele and SUI aim to restore bladder neck support by elevating the urethrovesical junction.Research Objective: To evaluate the effectiveness of various methods for correcting sexual dysfunction in women after reconstructive surgery for pelvic organ prolapse, taking into account clinical, psychological, and subjective parameters of sexual quality of life.
2. Materials and Methods
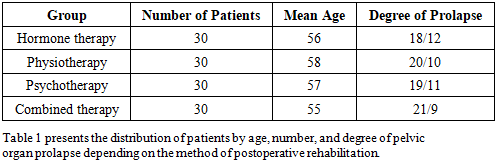
- Between 2024 and 2025, we treated 120 female patients with varying degrees of pelvic organ prolapse (POP), including anterior, posterior, and apical variants. The study included postmenopausal women aged 45 to 70 years who had not previously received specialized treatment for sexual dysfunction. The degree of POP was assessed using the standard POP-Q scale. All patients underwent reconstructive surgical procedures (colpoplasty, sacrospinous fixation, laparoscopic sacrovaginopexy, etc.) followed by structured postoperative follow-up. The postoperative period included planned correction of sexual dysfunction based on clinical presentation. Patients were randomized into four groups based on the rehabilitation method: Hormone therapy (local estrogens and systemic drugs). Physiotherapy (electrostimulation, Kegel exercises, myostimulation). Psychotherapy (individual and group counseling).Combined approach (a combination of all the above methods).Sexual function was assessed using the validated Russian version of the Female Sexual Function Index (FSFI) before the start of treatment and six months into the correction program. In addition, subjective satisfaction, psycho-emotional state (via the HADS scale), and overall quality of life improvement (via the SF-36 scale) were evaluated.
|
3. Results
- The most significant improvement in FSFI scores was observed in the combined therapy group (p<0.01), with the average FSFI score increasing from 15.0 to 25.6. Improvements were noted across all domains: desire, arousal, orgasm, satisfaction, pain reduction, and vaginal lubrication. Patients reported restored self-esteem, decreased anxiety and depression, and a significant increase in interest in intimate life. Subjective satisfaction with treatment reached 92%. General well-being improved as well, with reduced complaints of vaginal dryness, better sleep, and enhanced psycho-emotional balance. In the hormone therapy group, FSFI increased from 15.2 to 20.4, with the most notable improvements in "arousal" and "vaginal lubrication" domains due to the trophic effects of estrogens that enhance microcirculation and vaginal mucosa health. However, progress in the "orgasm" and "satisfaction" domains was less pronounced. Around 60% of patients noted improved general well-being, while 25% reported temporary side effects such as mastodynia, mood instability, and headaches. The effectiveness of therapy depended significantly on dosing regimen and individual estrogen sensitivity. Physiotherapy showed an FSFI increase from 14.8 to 21.1, with marked improvements in the "orgasm" and "satisfaction" domains. The program included regular Kegel exercises, myostimulation, and electromagnetic pelvic floor muscle stimulation. These measures enhanced muscle control, improved blood flow, and increased sensitivity in the intimate area. Patients reported new sensations during intercourse, greater confidence, and reduced pain during sex. However, benefits were sustained only with regular practice. Psychotherapeutic intervention led to an FSFI increase from 14.5 to 21.8. Effectiveness was particularly high among women with elevated anxiety, chronic stress, depressive symptoms, and body image disturbances. Psychocorrection methods included cognitive-behavioral therapy, elements of Gestalt therapy, emotional relief techniques, and work on family relationships. After 12 sessions of individual therapy, most patients experienced breakthroughs in overcoming internal barriers and fears related to intimacy. Women reported increased interest in their partner, reduced shame, and improved couple communication. The largest gains were observed in the "desire" and "arousal" domains. Continued psychotherapy after the study ended was found to enhance and sustain the results over time.
4. Discussion
- The results of this study confirm the high efficacy of a multidisciplinary approach in correcting sexual dysfunction in women following reconstructive surgery for pelvic organ prolapse (POP). The greatest therapeutic effect was achieved through the use of combined therapy, underscoring the need for simultaneous attention to somatic, hormonal, and psycho-emotional aspects of female sexuality. Hormone therapy showed significant improvements in physiological factors related to vaginal dryness and arousal. However, its influence on the psycho-emotional dimension of sexuality—such as orgasm and satisfaction—was limited. This suggests that hormone therapy is effective as a symptomatic treatment but does not address all facets of sexual dysfunction. Physiotherapeutic methods proved valuable in the rehabilitation of pelvic floor muscle function, directly impacting the quality of sexual sensations and control over sexual activity. Nevertheless, sustainable results required long-term, systematic engagement from the patients and strong motivation to adhere to the exercise regimen. Psychotherapy emerged as a crucial treatment component, particularly for women with pronounced anxiety, depressive symptoms, fear of intimacy, low self-esteem, and body image disturbances. Addressing these psycho-emotional issues led to significant improvements in desire and arousal—effects that could not be achieved through physiological means alone. Thus, the study highlights the need to integrate diverse therapeutic strategies to fully restore sexual health. The combined approach yielded the best outcomes across all FSFI parameters and achieved the highest level of subjective patient satisfaction. Given the heterogeneous nature of sexual dysfunction, personalized therapy tailored to each patient's medical, psychological, and social context is warranted. Promising directions for future research include investigating the partner’s role in the rehabilitation process, assessing the long-term sustainability of combined therapy outcomes, and developing algorithms for individualized treatment planning.
5. Conclusions
- This study demonstrated that correcting sexual dysfunction in women after reconstructive surgery for POP requires a comprehensive and individualized approach. All investigated treatment methods had a positive impact on sexual function parameters; however, the intensity and durability of these effects varied significantly depending on the strategy used. Hormone therapy proved effective in addressing local symptoms such as dryness and discomfort and improved the physiological aspects of sexual life. Physiotherapy aided in restoring pelvic floor muscle tone and sensitivity, enhancing orgasmic function and overall satisfaction. Psychotherapy was essential for overcoming psycho-emotional barriers and normalizing mental health, especially in women with anxiety and depressive disorders. The highest outcomes were achieved in the combined therapy group, emphasizing the importance of a multifactorial approach in sexual function rehabilitation. Only the integration of physiological, hormonal, and psychotherapeutic methods ensures the best clinical and subjective results. Therefore, the correction of sexual dysfunction following surgical treatment for POP should involve a comprehensive assessment of all components of a woman’s sexual health and be guided by the principles of interdisciplinary collaboration. Future research should focus on developing personalized therapy programs and evaluating the long-term results of such interventions.