-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4741-4744
doi:10.5923/j.ajmms.20251512.118
Received: Oct. 23, 2025; Accepted: Nov. 20, 2025; Published: Dec. 31, 2025

Surgical Stratefies for Sellar Tumors Emphasis on Transcranial Access
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUygun U. Altybayev1, Gayrat M. Kariyev2, Alisher M. Sultanov3, Jaxongir Z. Yo’ldoshev4, Gulrux T. Achilova5, Robiya R. Uzakova6
1Head of the Neuro-oncology Department of the Republican Specialized Scientific and Practical Medical Center of Neurosurgery
2Director, Professor of the Republican Scientific Center for Neurosurgery, Tashkent, Republic of Uzbekistan
3Doctor of Neurophysiologist of the Republican Specialized Scientific and Practical Medical Center of Neurosurgery
4Postgraduate Student of the Republican Specialized Scientific and Practical Medical Center of Neurosurgery
5Assistant Department of Neurosurgery Tashkent State Medical University
6Tashkent, Republic of Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Tumors of the sellar and suprasellar regions represent a significant neurosurgical challenge due to their complex anatomical relationships and potential for endocrine, visual, and neurological complications. Advances in microsurgical anatomy and skull base surgery have significantly expanded the understanding of this region and the available surgical corridors [1]. While endoscopic endonasal approaches have become widely adopted for the treatment of many pituitary and suprasellar tumors, transcranial approaches continue to play a crucial role in the management of large, invasive, or atypically located tumors that extend beyond the limits of endonasal exposure [2–4]. In such cases, transcranial surgery provides wider visualization and safer manipulation of critical neurovascular structures [5]. This study analyzes the clinical outcomes of 382 patients with sellar region tumors treated at the Republican Specialized Scientific and Practical Medical Center of Neurosurgery (Uzbekistan) between 2016 and 2023. Patients were divided into five groups according to the type of transcranial approach used: transcallosal, transcortical transventricular, subfrontal, pterional, and bifrontal (including a modified bifrontal technique). Similar classifications of transcranial routes have been described in previous surgical series addressing complex sellar and suprasellar tumors [6,7]. The analysis demonstrated that transcranial approaches provide broader surgical access and allow subtotal or total tumor resection in selected cases, particularly for giant pituitary adenomas and craniopharyngiomas with significant suprasellar, parasellar, or third ventricular extension [8,9]. These findings are consistent with reports emphasizing the continued relevance of transcranial surgery for tumors with firm consistency, vascular encasement, or irregular growth patterns [10]. Complication profiles varied by approach. Bifrontal and pterional craniotomies achieved higher resection rates in large and complex tumors but were associated with increased risks of diencephalic dysfunction and postoperative endocrine disorders. Similar complication patterns have been reported in comparative studies of transcranial versus transsphenoidal surgery [11,12].
Keywords: Sellar region tumors, Transcranial approach, Suprasellar tumors, Pituitary adenoma, Craniopharyngioma, Neurosurgery, Surgical outcomes, Bifrontal craniotomy, Pterional approach, Uzbekistan
Cite this paper: Uygun U. Altybayev, Gayrat M. Kariyev, Alisher M. Sultanov, Jaxongir Z. Yo’ldoshev, Gulrux T. Achilova, Robiya R. Uzakova, Surgical Stratefies for Sellar Tumors Emphasis on Transcranial Access, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4741-4744. doi: 10.5923/j.ajmms.20251512.118.
Article Outline
1. Introduction
- Tumors of the sella turcica and suprasellar region represent a complex interdisciplinary problem requiring collaboration between neurosurgeons, endocrinologists, and radiologists. The choice of surgical approach depends on tumor size, growth pattern, invasiveness, and relationship to surrounding neurovascular structures [3,5]. Over the past century, transsphenoidal surgery has become the preferred approach for most pituitary adenomas due to its lower morbidity and favorable endocrine outcomes [13,14]. The development of fully endoscopic endonasal techniques has further expanded surgical indications and reduced complication rates [15]. Despite these advances, transcranial approaches remain indispensable in selected cases. Large, invasive tumors with lateral, posterior, or superior extension, as well as lesions with dense fibrous consistency or encasement of major vessels, may not be safely or completely resected via an endonasal route [2,6,10]. In such situations, transcranial access provides superior control over the optic apparatus, hypothalamus, and major cerebral arteries. The goals of surgical treatment of sellar and suprasellar tumors include elimination of mass effect, normalization of pituitary hypersecretion, preservation or restoration of pituitary function, prevention of recurrence, and acquisition of tissue for histopathological analysis [4,9]. For these reasons, mastery of both transsphenoidal and transcranial techniques remains essential for neurosurgeons specializing in pituitary and skull base surgery [7,11].The Purpose. This topic is to examine in detail the indications, advantages, and limitations of transcranial approaches, as well as the need to compare their effectiveness in modern neurosurgical interventions.
2. Material and Methods of Research
- The study is based on the results of observations of 382 patients with tumors of the sella turcica region who were hospitalized at the Republican Specialized Scientific and Practical Medical Center for Neurosurgery of the Ministry of Health of the Republic of Uzbekistan between 2016 and 2023. The patients' ages ranged from 7 to 62 years. There were 59 males (45%) and 72 females (55%). The observation period ranged from 6 months to 5 years. The average age of patients at the time of the initial surgery was 33.5 years. All patients underwent a full range of diagnostic tests, including clinical neurological, clinical paraclinical, clinical instrumental, and clinical laboratory examinations. The clinical diagnosis was verified using overview and targeted craniography, as well as neuroimaging methods such as computed tomography (CT) or magnetic resonance imaging (MRI) of the brain. The individual characteristics of the tumors in the sellar region were studied in all patients, and additions were made to the existing indications for selecting the most optimal transcranial access. In addition, preoperative preparation was developed for each patient in accordance with the selected transcranial access. According to the primary surgical approach used, patients were divided into 5 groups:
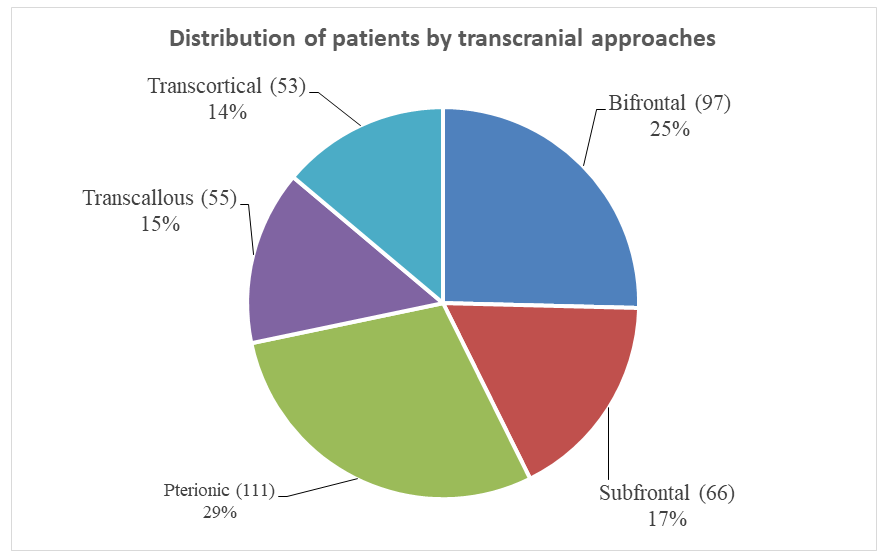 | Figure 1. Distribution of patients by transcranial access |
3. Results and Discussion
- We conducted a study of the radicality of removing tumors in the sella turcica region complicated by hydrocephalus, depending on the surgical approach used. Figure 1 shows that pterional and bifrontal approaches were mainly used to remove such tumors. In combination with the use of these approaches, total removal was achieved in 152 of the 382 patients who underwent surgery, which amounted to 40%. It should be noted that the more radical the tumor removal, the greater the risk of developing secondary disorders. This is because the tumor capsule is closely connected to the structures of the hypothalamus and is located in close proximity to the main artery, and in the postoperative period, diencephalic disorders are often observed in the form of an increase in body temperature, chills, general weakness, and drowsiness. There is also a clinical picture of ADH (antidiuretic hormone) deficiency due to damage to the pituitary stalk, which is accompanied by polyuria, polydipsia, and decreased urine density. Subtotal resection was performed in 179 (47%) patients. In some cases, due to the immediate proximity and close location to the main artery, removal of the lower part of the tumor capsule was impossible or excessively risky.In 51 (13%) patients, due to the density of the tumor, its adhesion to surrounding structures, profuse bleeding, and hemodynamic instability during surgery, tumor removal was limited to partial removal.
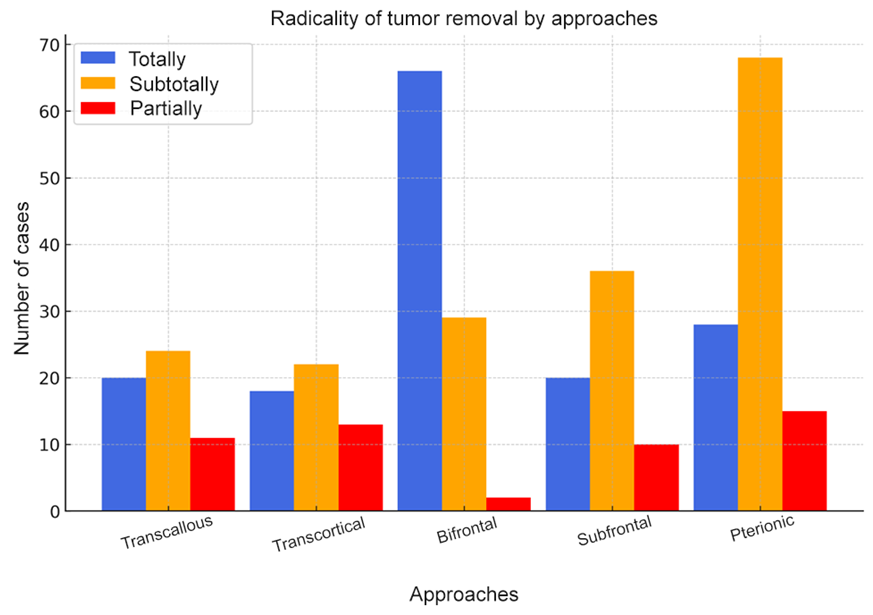 | Figure 2. Radicality of tumor removal by access |
4. Conclusions
- As a rule, most tumors of the sellar region are benign, slow-growing neoplasms. Early detection of these tumors is an important prognostic factor in surgical treatment, allowing for the most radical removal of the tumor, preservation of vital functions, and minimization of postoperative complications. This is due to the choice of the most optimal surgical approach for the operation. Figure 2 shows that when removing tumors of the suprasellar region of the brain, the use of a bifrontal approach allows for more complete and subtotal resection of the tumor compared to other approaches. This, in turn, led to the development of a modified bifrontal approach aimed at eliminating the shortcomings of the existing bifrontal approach and preventing possible complications associated with this method.