-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4725-4728
doi:10.5923/j.ajmms.20251512.116
Received: Sep. 27, 2025; Accepted: Oct. 22, 2025; Published: Dec. 31, 2025

Spatial Distribution of Ventricular Arrhythmia Sources: Retrospective Analysis of Localization in 177 Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSultanov Berdimurat Abdurashid oʻgʻli
Republican Specialized Cardiology Scientific and Practical Medical Center, 9th Department of Interventional Arrhythmology, Tashkent, Uzbekistan
Correspondence to: Sultanov Berdimurat Abdurashid oʻgʻli, Republican Specialized Cardiology Scientific and Practical Medical Center, 9th Department of Interventional Arrhythmology, Tashkent, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Idiopathic ventricular arrhythmias (VAs) often arise in the absence of structural heart disease, yet their sources vary widely across anatomical locations. Understanding the spatial distribution of VA foci is essential for optimizing catheter ablation strategies. Objective. To retrospectively analyze the anatomical localization of idiopathic ventricular arrhythmia sources in 177 patients and assess the impact of radiofrequency ablation (RFA) on quality of life. Methods. A total of 177 patients with documented focal VAs underwent electrophysiological mapping and RFA between 2020 and 2024. Arrhythmia origins were identified through activation mapping and pacing morphology analysis, and were categorized by anatomical region. Pre- and post-procedural quality of life was assessed using the SF-36 questionnaire. Results. The most common origin of VAs was the septal region of the right ventricular outflow tract (RVOT), accounting for 41.2% of cases. Additional frequent foci included the anterior RVOT wall (13.6%), left ventricular (LV) summit (7.9%), and fascicular regions (7.3%). More than 60% of arrhythmias originated from RVOT and LV summit areas. Rare sites included the His–Purkinje system, mitral annulus, and coronary cusps of Valsalva. Following RFA, significant improvements were observed in both the physical (from 42.1 ± 5.6 to 45.4 ± 6.9, p = 0.01) and psychological (from 42.3 ± 6.0 to 48.2 ± 7.0, p < 0.0001) SF-36 components, with total score rising from 84.4 ± 10.4 to 93.6 ± 12.8 (p = 0.0003). Conclusion. The RVOT—particularly its septal segment—is the predominant site of idiopathic VA origin. The heterogeneity of arrhythmic sources underscores the necessity for precise mapping and individualized ablation strategies. RFA significantly enhances quality of life in affected patients.
Keywords: Idiopathic ventricular arrhythmia, Ventricular arrhythmia localization, Right ventricular outflow tract (RVOT), Left ventricular summit, Fascicular ventricular tachycardia, Electrophysiological mapping, Radiofrequency ablation (RFA), His–Purkinje system
Cite this paper: Sultanov Berdimurat Abdurashid oʻgʻli, Spatial Distribution of Ventricular Arrhythmia Sources: Retrospective Analysis of Localization in 177 Patients, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4725-4728. doi: 10.5923/j.ajmms.20251512.116.
1. Introduction
- Ventricular arrhythmias (VAs) represent a significant clinical problem, particularly in patients without structural myocardial disease. Focal forms of VAs may originate from various anatomical structures, including the right ventricular outflow tract (RVOT), the left ventricle (LV), the coronary cusps of Valsalva, the conduction system, and the mitral annulus [1]. Detailed mapping and understanding of the anatomical localization of VA sources make it possible to optimize approaches to radiofrequency ablation and improve treatment efficacy [4].The aim of the present study was to quantitatively assess the incidence of VAs in different cardiac regions based on retrospective analysis data.
2. Materials and Methods
- The study included 177 patients with documented focal ventricular arrhythmias who underwent electrophysiological study and radiofrequency ablation between 2020 and 2024 at a specialized arrhythmology center. Patients with a history of myocardial infarction, significant valvular heart disease, or cardiomyopathies were excluded.The arrhythmia source was determined based on local pre-excitation, activation timing, and QRS morphology during pacing.The data were classified according to anatomical regions: RVOT, right ventricle (RV), left ventricle (LV), coronary cusps of Valsalva, fascicular VAs, the His–Purkinje system, and the mitral annulus (MA). For each region, absolute frequencies and percentage proportions were calculated.
3. Results
- Analysis of 177 documented VA episodes revealed a marked predominance of arrhythmogenic foci in the septal portion of the right ventricular outflow tract (RVOT), where 73 cases were identified, accounting for 41.2% of all observations. This finding confirms the pivotal role of this region in the origin of idiopathic arrhythmias [2]. Significantly less frequently, VAs were localized in the anterior RVOT wall (24 cases, 13.6%) and in the region of the LV summit (14 cases, 7.9%) (Fig. 1).
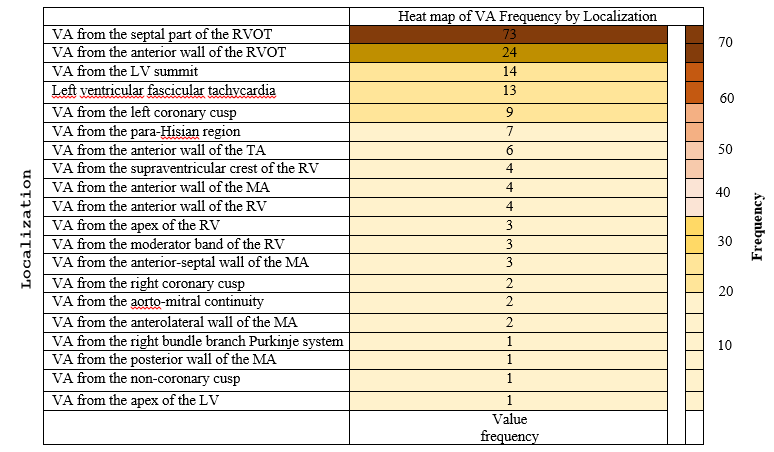 | Figure 1. Heat map of VA frequency by localization |
4. Discussion
- The findings of this study corroborate previous observations regarding the predominance of VAs originating from the RVOT [5]. A substantial proportion of arrhythmias originating from the LV summit and the fascicular system further underscores the importance of these localizations in ablation planning. Unlike the sinuses of Valsalva, ablation in the fascicular region requires particular attention to the anatomy of the conduction system due to the risk of atrioventricular block [6].The distribution of arrhythmogenic foci demonstrates high heterogeneity and highlights the necessity of a personalized approach to the selection of access routes and ablation energy parameters [1].
5. Conclusions
- 1. The most frequent source of VAs is the septal portion of the RVOT (41.2%).2. A substantial proportion of cases arise from the anterior RVOT wall, the LV summit, and fascicular VAs.3. The distribution of arrhythmic foci demonstrates considerable diversity, necessitating meticulous electrophysiological mapping and careful consideration of anatomical features.
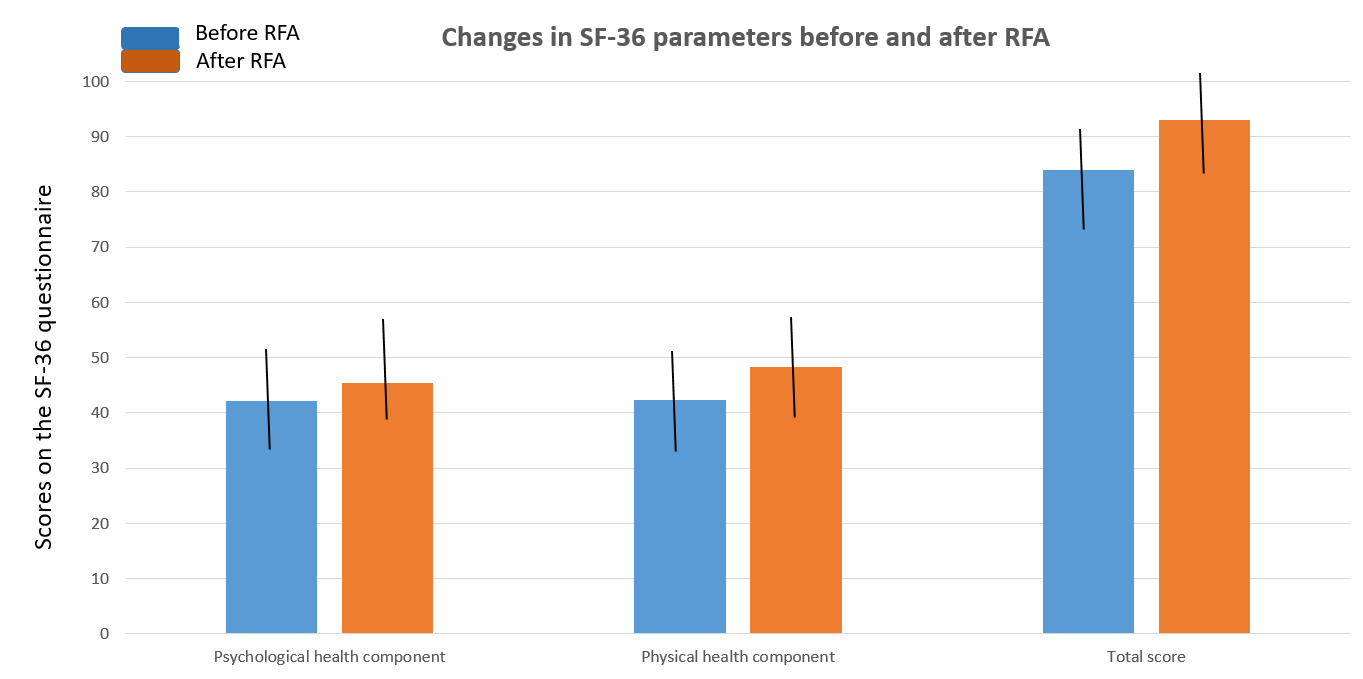 | Figure 2. Quality of life assessment using the SF-36 questionnaire |
|
