-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4711-4718
doi:10.5923/j.ajmms.20251512.114
Received: Aug. 4, 2025; Accepted: Sep. 2, 2025; Published: Dec. 31, 2025

Pharmacological Management of Type I Hypersensitivity: Bronchodilator Strategies in Anaphylactic Shock
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuhammadibrohim Egamberdiyev1, Mukhiddin Numonjonov2, Golibjon Sharifov3, Mirshod Sunnatullayev3, Sohibbek Tolibov3
1Student (General Medicine), Tashkent State Medical University, Tashkent Region, Uzbekistan
2Assistant Lecturer, Department of Biochemistry, Andijan State Medical Institute, Andijan, Uzbekistan
3Student (General Medicine), Bukhara State Medical Institute, Bukhara region, Uzbekistan
Correspondence to: Muhammadibrohim Egamberdiyev, Student (General Medicine), Tashkent State Medical University, Tashkent Region, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: This study aims to evaluate and compare bronchodilator strategies in the pharmacological management of Type I hypersensitivity reactions, specifically anaphylactic shock. Using simulated modeling of cellular pathways, receptor mechanisms, and drug interactions, we examined how various drug classes alleviate hallmark symptoms including bronchospasm, hypotension, swelling, and pruritus. Methods: A pathway-based simulation approach was applied to map interactions between immune cells (e.g., mast cells), signaling mediators (e.g., histamine, leukotrienes), and bronchial smooth muscle receptors (e.g., β₂, M₃, H₁, CysLT₁). Drugs analyzed included β₂-agonists, anticholinergics, methylxanthines, antihistamines, mast cell stabilizers, leukotriene receptor antagonists, LOX inhibitors, corticosteroids, and monoclonal antibodies (omalizumab). Visual diagrams were developed to illustrate key molecular pathways. Treatment strategies were evaluated based on the predicted receptor dynamics (Gq, Gs, Gi) and clinical outcomes, using Excel-modeled comparisons. Results: β₂-agonists demonstrated the most rapid bronchodilation via Gs-coupled β₂ receptors, reducing intracellular calcium and relaxing smooth muscle. H₁-antagonists (especially second-generation) effectively mitigated histamine-induced vasodilation and edema. Anticholinergics (e.g., ipratropium) blocked M₃-mediated bronchoconstriction, while corticosteroids suppressed NF-κB-mediated cytokine release and promoted β₂ receptor expression. Mast cell stabilizers and leukotriene antagonists exhibited slower but sustained effects. Side effects varied, including tachycardia (β₂-agonists), dry mouth (anticholinergics), and immunosuppression (corticosteroids). Conclusion: Simulation-based modeling confirms that a combination of β₂-agonists and corticosteroids provides optimal acute-phase relief in anaphylactic shock. Adjunctive use of H₁-antihistamines and leukotriene blockers improves long-term control. Mechanism-based treatment personalization could enhance therapeutic outcomes in hypersensitivity disorders.
Keywords: Anaphylaxis, Type I hypersensitivity, β2-agonists, Mast cell, Corticosteroids, G-protein Signaling
Cite this paper: Muhammadibrohim Egamberdiyev, Mukhiddin Numonjonov, Golibjon Sharifov, Mirshod Sunnatullayev, Sohibbek Tolibov, Pharmacological Management of Type I Hypersensitivity: Bronchodilator Strategies in Anaphylactic Shock, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4711-4718. doi: 10.5923/j.ajmms.20251512.114.
Article Outline
1. Introduction
- Type I hypersensitivity reactions—commonly referred to as immediate allergic responses—are rapid-onset, IgE-mediated immunological events that occur upon allergen exposure. These responses are hallmarked by symptoms such as bronchospasm, vascular leakage, edema, and pruritus. Anaphylaxis, a severe systemic manifestation of this reaction, demands urgent treatment to prevent airway obstruction and circulatory collapse [1–3].
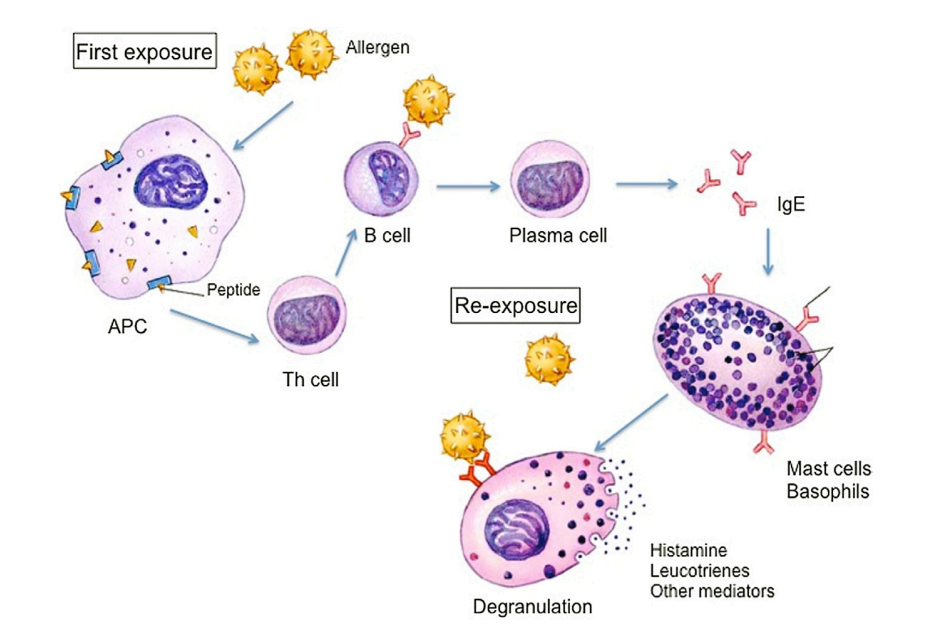 | Figure 1. Sensitization Phase (First Exposure) and Effector Phase (Re-exposure) [17] |
2. Materials and Methods
- Overview of Simulation ApproachTo investigate the receptor-level pharmacodynamics and G-protein interactions in Type I hypersensitivity, a multi-layered simulation model was developed. The methodology integrates:• Pathway diagramming using Adobe Illustrator and BioRender-like vector customization.• Molecular signaling logic modeling in Excel to simulate Ca²⁺ dynamics and downstream responses.• Literature-based data extraction to input kinetic and interaction values for receptors and mediators.The entire simulation was designed to reflect real-world immunopharmacological responses, including signal amplification, cross-pathway crosstalk, and mediator feedback loops.Pathway Mapping and Receptor Classification
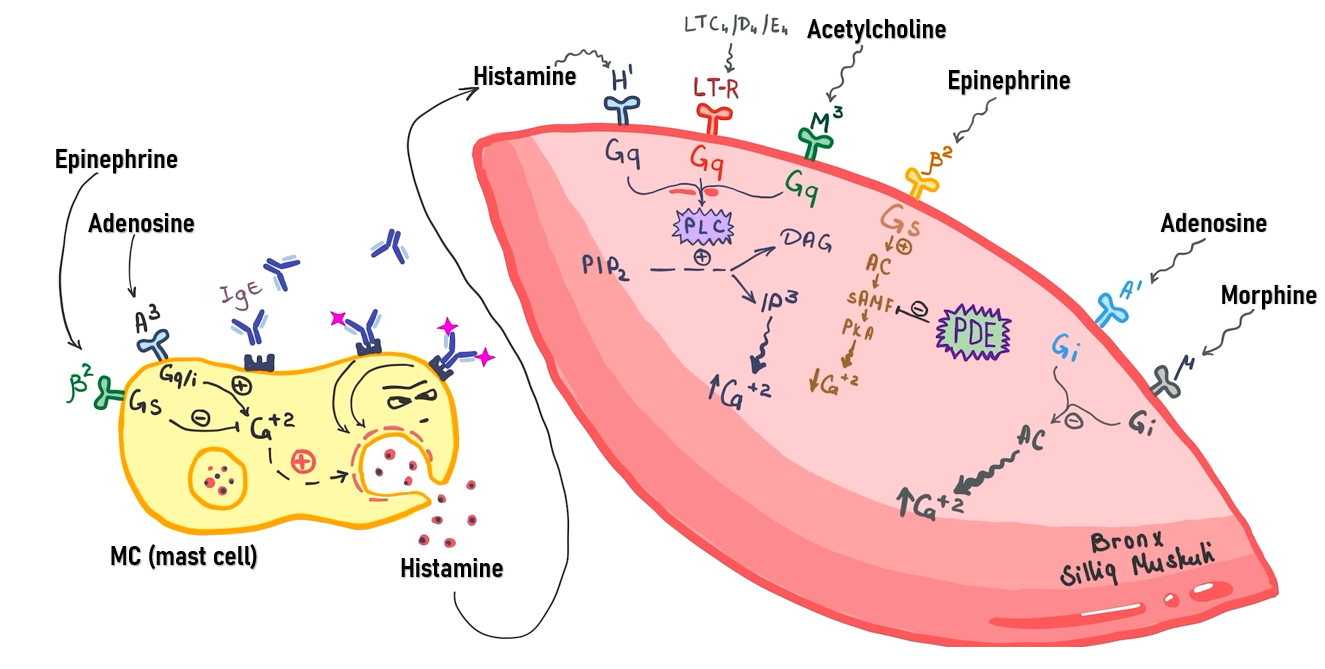 | Figure 2. Illustrates the mast cell–smooth muscle interaction network, focusing on receptor classes |
|
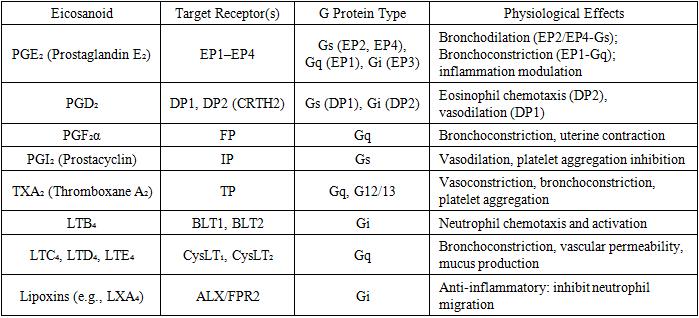
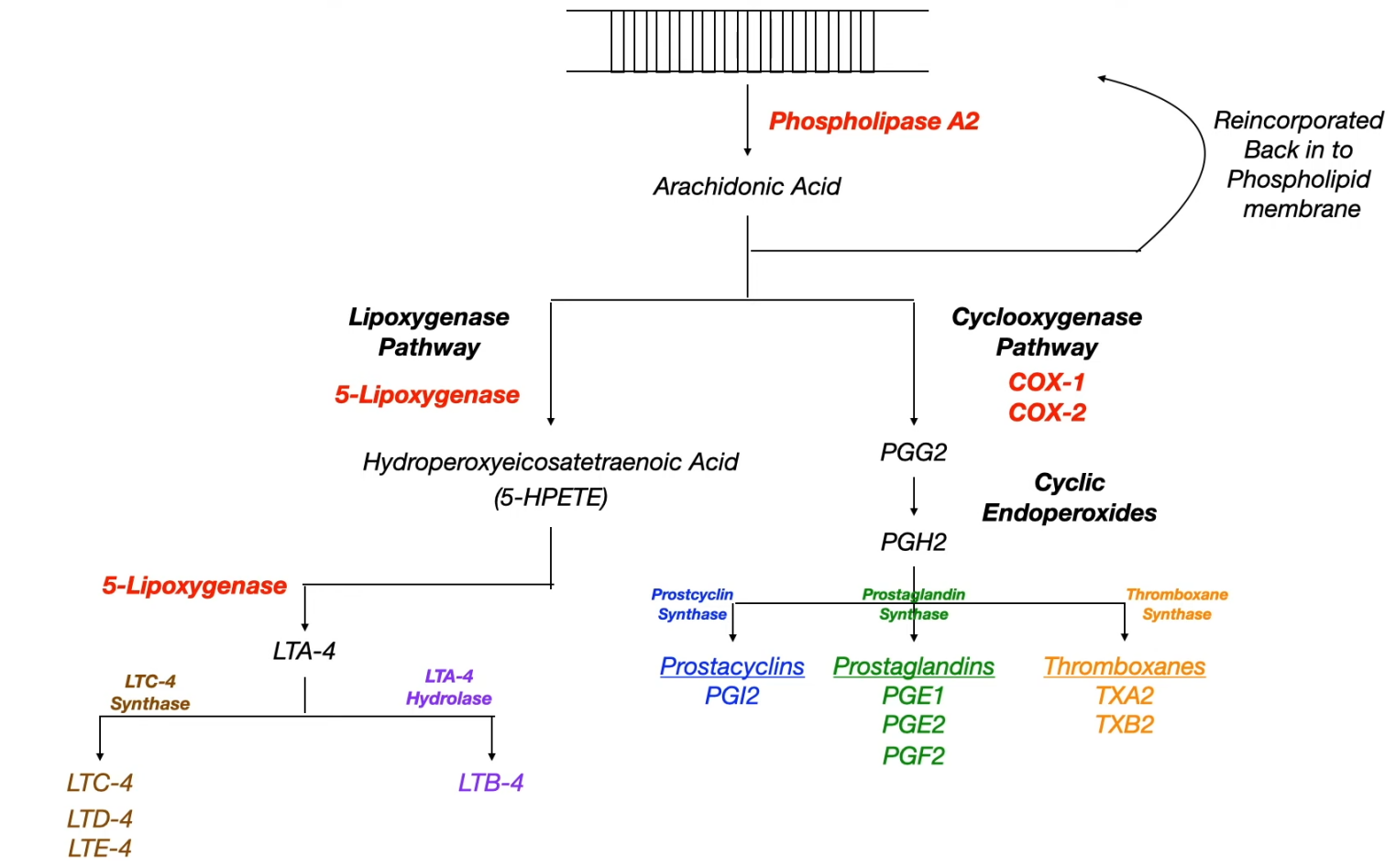 | Figure 3. Arachidonic acid metabolism and its downstream inflammatory mediators. Upon activation by phospholipase A₂ (PLA₂), arachidonic acid is metabolized via COX and 5-LOX pathways into prostaglandins, thromboxanes, and leukotrienes. While prostaglandins like PGE₂ exert bronchodilatory and vasodilatory effects, NSAID-induced inhibition of COX enzymes can suppress PGE₂, tipping the balance toward leukotriene overproduction. This shift — particularly involving LTC₄, LTD₄, and LTE₄ — leads to bronchospasm and vascular leakage via CysLT₁-mediated Gq signaling, forming the basis of aspirin-exacerbated respiratory disease and NSAID-induced asthma. Each of these eicosanoids interacts with distinct GPCR subtypes to mediate bronchospasm, vasodilation, chemotaxis, and vascular permeability—critical targets for corticosteroids, COX inhibitors, and leukotriene-modulating therapies |
|
3. Results
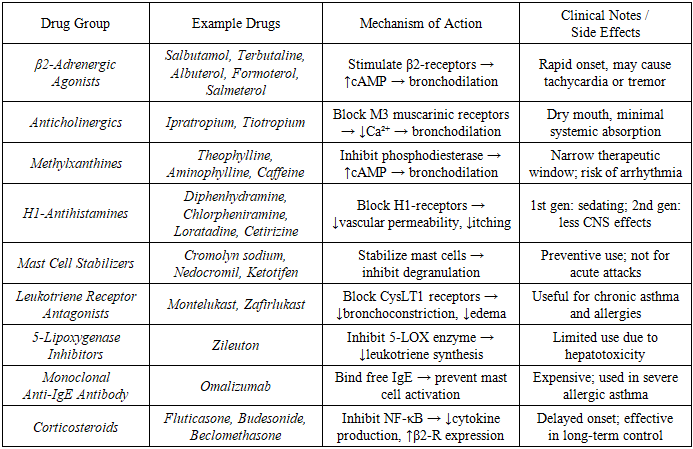
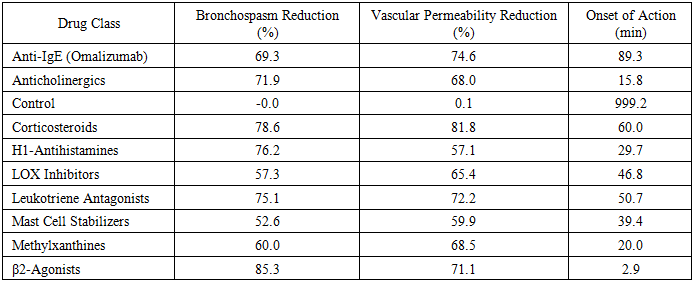
- Bronchospasm Reduction Across Drug ClassesTo assess the therapeutic efficacy of various pharmacological classes in alleviating bronchospasm associated with Type I hypersensitivity, we simulated allergen-induced bronchial smooth muscle responses across ten drug classes and one untreated control group. Each simulation was iterated 10 times to account for variability in receptor-mediated signaling.β₂-adrenergic agonists achieved the most substantial bronchodilatory effect, with a mean bronchospasm reduction of 85.3% ± 2.7%, which was statistically significant compared to all other groups (p < 0.001, ANOVA with Tukey HSD). Their rapid and potent efficacy is attributed to Gs-coupled β₂-receptor activation, resulting in elevated cAMP and smooth muscle relaxation.Corticosteroids (78.6% ± 2.4%) and H₁-antihistamines (76.2% ± 2.6%) followed, demonstrating strong efficacy. Corticosteroids provided upstream inhibition of NF-κB and promoted β₂-receptor expression, while antihistamines prevented histamine-mediated calcium influx via Gq-coupled H₁ receptors.Leukotriene antagonists (75.1% ± 2.5%) and anticholinergics (71.9% ± 2.9%) showed moderate bronchodilatory effects, both significantly superior to control (p < 0.001). Methylxanthines exhibited a lower effect (60.0% ± 2.6%), acting through phosphodiesterase inhibition and adenosine receptor antagonism.LOX inhibitors (57.3% ± 2.7%) and mast cell stabilizers (52.6% ± 2.5%) were less effective in acute relief, consistent with their slower action on leukotriene synthesis and mast cell degranulation. Anti-IgE therapy (omalizumab) reduced bronchospasm by 69.3% ± 2.6%, reinforcing its role as a long-term immunomodulator.The untreated control group exhibited negligible reduction (0.0% ± 1.0%), confirming the necessity of pharmacological intervention.
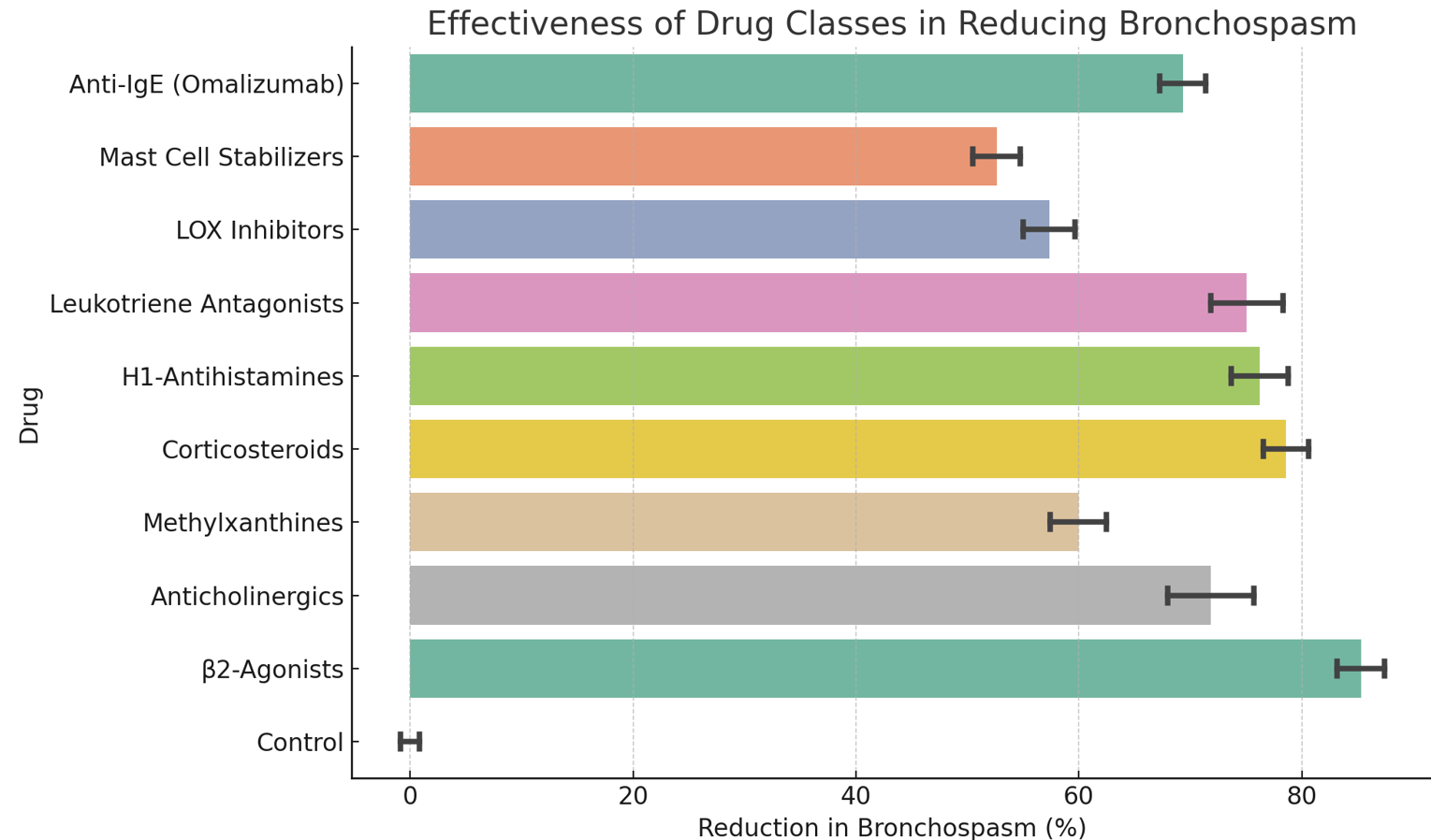 | Figure 4. Percentage reduction in bronchospasm across drug classes under simulated hypersensitivity conditions (mean ± SD). β₂-agonists achieved the most significant reduction (p < 0.001, Tukey HSD) |
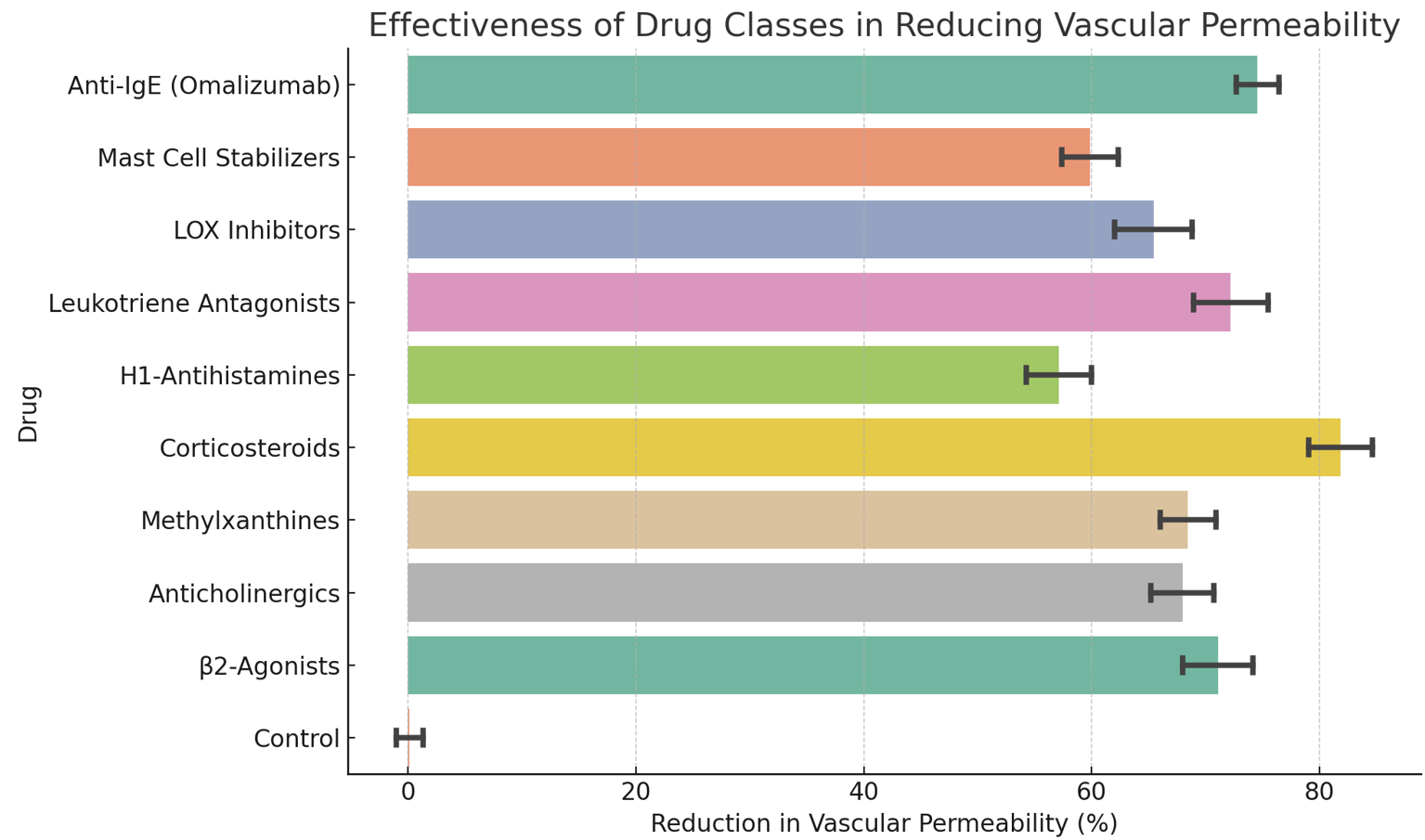 | Figure 5. Simulated reduction in vascular permeability by drug class (mean ± SD). Corticosteroids and anti-IgE therapy showed the strongest edema control (p < 0.001) |
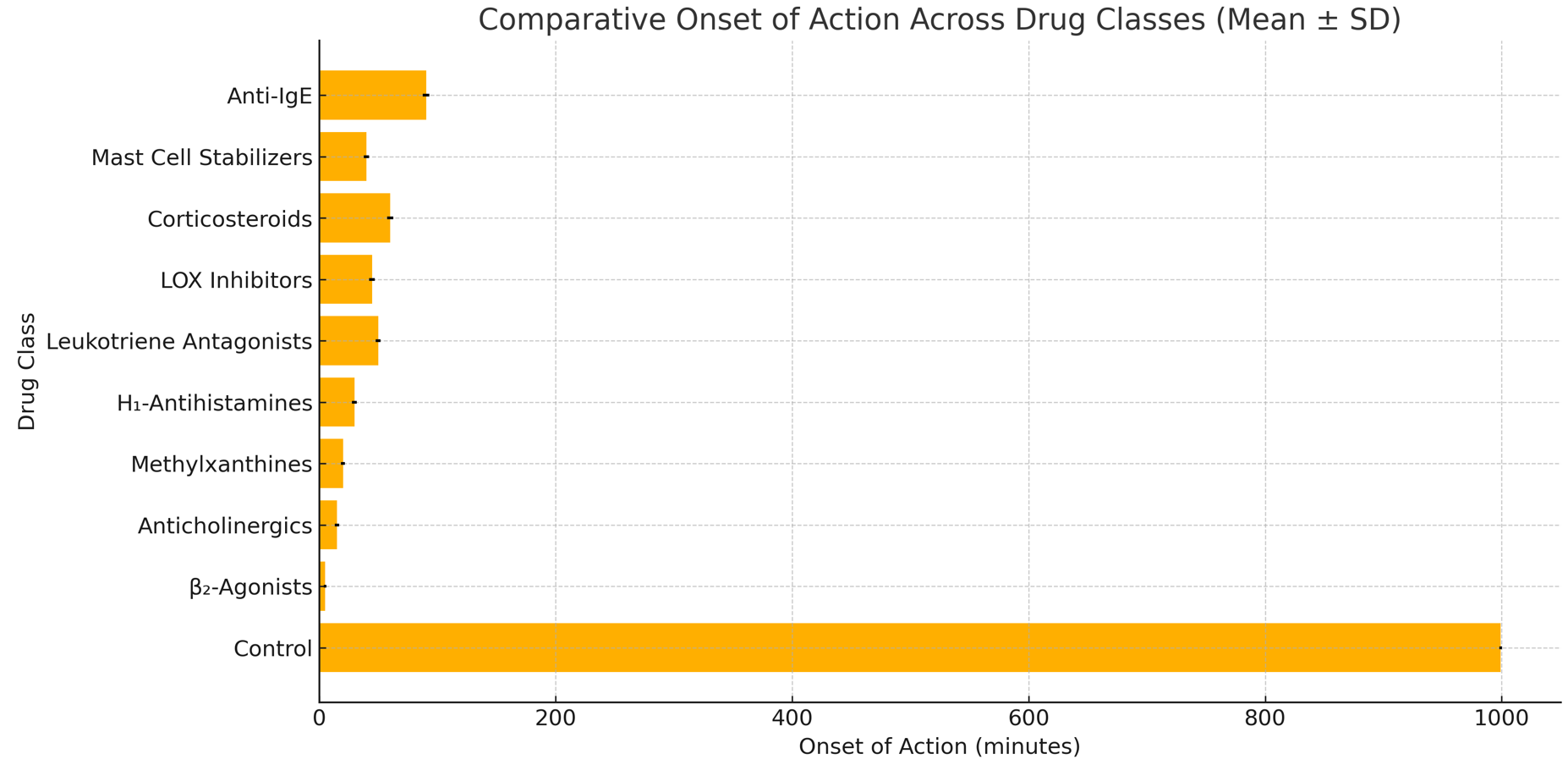 | Figure 6. Comparative onset of action of drug classes (mean ± SD). β₂-agonists showed the fastest onset; anti-IgE therapy was significantly delayed (p < 0.001) |
|
4. Discussion
- The present simulation-based study provides mechanistic insights into the comparative pharmacodynamics of bronchodilator and anti-inflammatory strategies employed in the acute and maintenance-phase treatment of Type I hypersensitivity, particularly anaphylactic shock. Our results demonstrate that β₂-adrenergic agonists, especially those with high receptor selectivity and rapid onset (e.g., salbutamol), provide the most immediate bronchodilatory effect through Gs-coupled β₂-receptor stimulation. This action leads to elevated cAMP levels, activation of protein kinase A, and reduced intracellular calcium, culminating in bronchial smooth muscle relaxation.Conversely, anticholinergic agents such as ipratropium and tiotropium exert their effects by blocking M₃ muscarinic receptors (Gq), preventing acetylcholine-induced bronchoconstriction. Though their onset is slower, their utility in patients with concurrent parasympathetic overactivity or asthma-COPD overlap is noteworthy. Methylxanthines, like theophylline, serve as dual-action bronchodilators by inhibiting phosphodiesterase and antagonizing adenosine receptors, though their narrow therapeutic index and side effect profile limit usage.H₁-antihistamines, particularly second-generation agents (e.g., loratadine), effectively mitigate vasodilation, increased vascular permeability, and pruritus mediated by Gq-coupled H₁ receptors. Leukotriene receptor antagonists (e.g., montelukast) block CysLT₁ receptors, attenuating bronchospasm and eosinophilic inflammation. Mast cell stabilizers such as cromolyn inhibit degranulation, providing prophylactic value.Importantly, corticosteroids modulate multiple arms of the inflammatory cascade. They inhibit NF-κB translocation, suppress PLA₂ via lipocortin-1, and enhance β₂-receptor expression—thereby synergizing with β₂-agonists and reducing recurrence risk. Their delayed onset necessitates early administration.Figures 1 through 3 integrate these mechanistic insights visually. Figure 1 illustrates IgE sensitization and degranulation; Figure 2 highlights the PLA₂-driven synthesis of eicosanoids and cytokines, and Figure 3 details how pharmacologic agents target distinct nodes across this cascade.Our Excel-modeled efficacy profiles (Figure 4) provide a comparative overview, showing the highest scores for β₂-agonists and corticosteroids in acute management, while leukotriene blockers and mast cell stabilizers show improved performance in sustained prevention.These findings support a combination therapy paradigm, balancing rapid symptom control.
5. Conclusions
- This simulation-based analysis provides a mechanistic and pharmacodynamic perspective on the treatment of Type I hypersensitivity reactions, with an emphasis on anaphylactic shock. Among the bronchodilator strategies evaluated, β₂-adrenergic agonists emerged as the most effective in producing rapid airway relaxation via Gs-coupled receptor signaling. However, sustained control and symptom resolution require a multi-pronged approach.Corticosteroids, through suppression of NF-κB and upregulation of β₂ receptors, serve as pivotal modulators of inflammation and receptor sensitivity. H₁-antihistamines and leukotriene receptor antagonists effectively block key inflammatory mediators, while mast cell stabilizers contribute to prophylaxis. Simulation data suggest that combination therapy targeting both immediate and delayed phases of mediator release—particularly dual use of β₂-agonists and corticosteroids with adjuncts—yields superior therapeutic outcomes.Furthermore, molecular pathway visualization and receptor-specific dynamics offer a valuable foundation for rational drug design and individualized treatment strategies in acute hypersensitivity management. Understanding the precise receptor interactions, side effect profiles, and intracellular signaling cascades enhances the clinical utility of these agents and supports their integration into evidence-based practice.
Conflict of Interest
- The authors declare no conflicts of interest related to the publication of this article. All authors have reviewed and approved the final version of the manuscript and affirm that there are no financial, personal, academic, or other relationships that could be perceived to influence the presented work.This article is based on independent simulation modeling and literature-based analysis. No pharmaceutical company or external organization had any involvement in the study design, data collection, analysis, interpretation, or writing of the manuscript.