-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4238-4241
doi:10.5923/j.ajmms.20251512.09
Received: Aug. 7, 2025; Accepted: Sep. 2, 2025; Published: Dec. 5, 2025

The Impact of Early Diagnosis of Multiple Organ Failure on Treatment Prognosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAshurova Gulchehra Zakirzhanovna1, 2, Mamatkulov Ikhtiyor Bosimovich1
1Tashkent State Medical University, Uzbekistan
2National Children's Medical Center, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

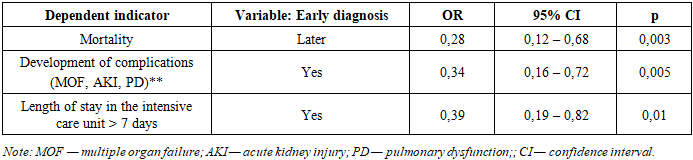
Multiple organ failure (MOF) is a leading cause of mortality in pediatric sepsis in the intensive care unit (ICU); early diagnosis remains a key factor in improving outcomes. Objective. To evaluate the impact of the timing of MOF diagnosis on treatment outcomes in pediatric sepsis. Materials and Methods. This retrospective study included 210 patients aged 6 months to 15 years (2022–2023): early diagnosis ≤3 hours (n=150) and late diagnosis >3 hours (n=60). Mortality, complications, and ICU length of stay were assessed. Multivariate logistic regression analysis adjusted for clinical and laboratory factors was used. Results. Early diagnosis of multiple organ failure was associated with reduced mortality (10% vs. 30%; p=0.002), length of stay in the intensive care unit (ICU) (7.3 ± 2.1 vs. 10.8 ± 3.5 days; p<0.01), and complication rates. Early diagnosis was associated with better outcomes across all age groups. Multivariate analysis confirmed its protective effect: OR for mortality was 0.28 (95% CI 0.12–0.68; p=0.003). The study power was 0.86. Conclusion. Early diagnosis of multiple organ failure in children with sepsis reduces mortality and severe complications, confirming the need for its implementation in clinical protocols and reducing the time to treatment.
Keywords: Multiple organ failure, Pediatric sepsis, pSOFA, Early diagnosis, Mortality, Lactate, Intensive care
Cite this paper: Ashurova Gulchehra Zakirzhanovna, Mamatkulov Ikhtiyor Bosimovich, The Impact of Early Diagnosis of Multiple Organ Failure on Treatment Prognosis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4238-4241. doi: 10.5923/j.ajmms.20251512.09.
1. Introduction
- Multiple organ failure (MOD) remains a leading cause of mortality in intensive care units worldwide. According to the World Health Organization (WHO), millions of cases of sepsis and associated MOD are reported annually, a significant proportion of which are fatal, especially in the absence of timely intervention [9]. MOD is a severe condition resulting from the body's systemic inflammatory response to infection, damaging vital organs and tissues [1,3]. As sepsis progresses to septic shock, the risk of developing MOD and an adverse outcome increases significantly [5,6,10]. Mortality from MOD in children can reach 25–35%, even with modern intensive care [17,18,23].One of the key factors contributing to an unfavorable prognosis is late diagnosis of organ dysfunction, leading to a delay in the initiation of therapeutic measures [10,19]. According to the international recommendations of the Surviving Sepsis Campaign, timely identification of organ dysfunction is the main condition for improving clinical outcomes [11,19,23].In recent years, increasing attention has been paid to the use of the pSOFA score, which demonstrates high prognostic value in children with sepsis [20,18]. Studies in 2022–2023 showed that an increase in pSOFA scores is associated with an increase in the severity of multiple organ dysfunction and mortality [20,23]. In addition to clinical scales, indicators of systemic hypoperfusion, in particular lactate levels, are recognized as important predictors of adverse outcome [21]. New multicenter studies in 2025 confirmed a significant relationship between hyperlactatemia and the risk of death in children with septic shock [21].In the post-pandemic period, methods for early prediction of severe sepsis are actively developing, including digital algorithms, machine learning technologies, and clinical decision support systems [23]. These innovative approaches aim to reduce the diagnostic window—the time between the onset of clinical deterioration and the verification of MOF.Despite the high relevance of the problem, data on the impact of the timing of MOF diagnosis on treatment outcomes in children in the CIS countries remain limited [3,4,7]. Recent studies confirm that early diagnosis and timely initiation of specialized therapy can significantly reduce mortality, complication rates, and length of stay in the intensive care unit [17,20,23].The aim of the study was to evaluate the impact of early diagnosis of multiple organ dysfunction on the prognosis and treatment outcomes of children with sepsis in the intensive care unit.
2. Materials and Methods
- A retrospective cohort study was conducted in the intensive care unit of the Tashkent Pediatric Medical Institute and the National Children's Medical Center (NCMC) from January 2022 to December 2023. The study analyzed the medical records of patients with a confirmed diagnosis of multiple organ failure and sepsis admitted to the intensive care unit (ICU). Current clinical protocols and scales for assessing multiple organ failure, such as the pSOFA score, were used to standardize the diagnosis.• Inclusion criteria: patients aged 6 months to 15 years with a confirmed diagnosis of multiple organ failure, complete medical records, including laboratory test results, clinical data at admission, and follow-up. • Exclusion criteria: patients with chronic diseases, such as terminal cancer, patients with incomplete documentation, and patients admitted in critical condition (septic shock), as these patients may require immediate treatment without the possibility of early diagnosis.Data were collected from medical records and included:• Time of diagnosis of multiple organ failure.• Clinical parameters at admission: body temperature. Heart rate (HR). Blood pressure (BP). Respiratory rate. Blood oxygen level (saturation). White blood cell count and other inflammatory markers (C-reactive protein, procalcitonin). Blood lactate level to assess tissue hypoperfusion.• Blood culture results, including pathogen type and antibiotic sensitivity, and other biochemical tests (bilirubin, creatinine, etc.).Applied treatment strategies (Time from diagnosis to initiation of treatment, administration of antibiotics, use of antibacterial therapy (choice of drugs, dosages, duration of therapy). Infusion therapy to maintain hemodynamics. Use of vasopressors to maintain blood pressure. Use of respiratory support (non-invasive or invasive ventilation).Time from diagnosis to treatment initiation.• Outcomes: length of stay in the intensive care unit (ICU), mortality, development of complications (multiple organ failure, acute kidney injury, pulmonary dysfunction).Missing data were assessed before analysis, and patients with missing key diagnostic parameters (pSOFA, lactate, CRP, PCT) were excluded. The study was approved by the local ethics committee. All patient data were anonymized to maintain confidentiality. Patient rights were protected in accordance with the Declaration of Helsinki.Multivariate logistic regression analysis was used to assess the impact of diagnostic timing on outcomes. Mortality, complications, and ICU stay of >7 days were considered as dependent variables. Models were adjusted for age, gender, baseline pSOFA, lactate level, infection source, and time to initiation of antibacterial therapy. Results are presented as odds ratios (OR) with 95% CI; p < 0.05 was considered statistically significant. Analysis was performed using SPSS 26.0.
3. Results
- The study included 210 patients aged 6 months to 15 years (150 with early diagnosis, 60 with late diagnosis) hospitalized with a confirmed diagnosis of multiple organ failure and sepsis in the intensive care unit (ICU) of the Tashkent Pediatric Medical Institute and the National Children's Medical Center (NCMC). The mean age of patients was 7.8 ± 3.2 years, of which 55% were boys and 45% were girls. The mean leukocyte level at admission to the ICU was 12.5 ± 2.3 x10⁹/L in the early diagnosis group and 14.1 ± 3.1 x10⁹/L in the late diagnosis group. The body temperature of patients in the early diagnosis group was 38.5 ± 0.7°C, while in the late diagnosis group it was 39.1 ± 0.6°C. Lactate levels were higher in patients with late diagnosis (3.8 ± 0.5 mmol/L) compared to patients with early diagnosis (2.9 ± 0.7 mmol/L). Moreover, higher lactate levels were associated with an increased risk of mortality, which is consistent with the results of recent multicenter studies [21].The study results are presented in terms of time to diagnosis, clinical parameters, and treatment outcomes.1. Time to diagnosis and initiation of treatment. In 150 patients (60%), multiple organ failure was diagnosed within the first 3 hours after admission to the ICU (early diagnosis group). In 60 patients (40%), diagnosis occurred 3 hours or more after admission (late diagnosis group).The mean time from admission to treatment was 2.4 ± 0.7 hours in the early diagnosis group and 4.6 ± 1.2 hours in the late diagnosis group (p < 0.001). A significant 50% reduction in lactate levels was observed in the early diagnosis group 48 hours after treatment initiation, compared with a 30% reduction in the late diagnosis group. The pSOFA scores after 72 hours decreased from 9.5 ± 1.2 to 6.4 ± 1.1 in the early diagnosis group and from 10.3 ± 1.3 to 8.1 ± 1.4 in the late diagnosis group (p < 0.01).2. Treatment outcomesMortality: In the early diagnosis group, mortality was 10% (n = 9). In the late diagnosis group, mortality was 30% (n = 18) (p = 0.002).A power analysis was performed using the actual mortality differences between the groups. With a sample size of 210 patients (150 early diagnosis, 60 late diagnosis), a significance level of α = 0.05, and a mortality difference of 10.0% versus 30.0%, the achieved statistical power was 0.86, indicating sufficient power to detect clinically significant differences between the groups. Length of stay in the intensive care unit: the mean length of stay in the intensive care unit was 7.3 ± 2.1 days in the early diagnosis group and 10.8 ± 3.5 days in the late diagnosis group (p < 0.01). In the late diagnosis group, 30% of patients had concomitant infections requiring antibiotic therapy adjustments, compared with 15% in the early diagnosis group. The time to initiation of infusion therapy averaged 1.8 ± 0.5 hours in the early diagnosis group and 3.2 ± 1.0 hours in the late diagnosis group. Patients who started infusion therapy earlier had a 20% lower risk of developing multiple organ failure. A subgroup analysis was conducted taking into account patient age (Table 1). In both age categories, early diagnosis was associated with a significantly lower mortality rate compared to late diagnosis. In children aged 6 months to 5 years, mortality was 7.5% with early diagnosis and 26.7% with late diagnosis. A similar trend was observed in the 6-15 year age group: 11.4% versus 33.3%, respectively. The data confirm that timely diagnosis of multiple organ failure improves survival regardless of age category.
|

|
4. Conclusions
- 1. The study results showed that early diagnosis of multiple organ failure (MOF) in children with sepsis is a key factor determining treatment outcome. Patients diagnosed with MOF within the first three hours of ICU admission had significantly better outcomes compared to those diagnosed later.2. Key findings include: Reduced mortality: 10% with early diagnosis versus 30% with late diagnosis (p = 0.002).3. Age-related stability of the effect: in both subgroups (6 months–5 years and 6–15 years), early diagnosis significantly reduced mortality; the effect was more pronounced in younger children.4. Reduced ICU stay: an average of 3.5 days shorter with early diagnosis (7.3 ± 2.1 versus 10.8 ± 3.5 days; p < 0.01).5. Fewer complications: the incidence of multiple organ failure, acute kidney injury, and pulmonary dysfunction was significantly lower with early diagnosis.6. Early antibacterial therapy: initiation of treatment within the first 3 hours after diagnosis reduced mortality to 9% versus 28% with a delay (p < 0.005).Thus, early diagnosis of multiple myeloma and prompt initiation of antibacterial therapy significantly improve treatment outcomes, reduce the length of stay in the intensive care unit (ICU), and reduce the incidence of complications. Implementation of early detection protocols and technologies that accelerate diagnosis is a priority for improving the effectiveness of pediatric intensive care.
5. Study Limitations
- This study has several limitations due to its retrospective design and use of medical record data, which may introduce a risk of incomplete information and selection bias. To minimize bias, patients with missing key diagnostic parameters were excluded from the analysis. Despite the use of uniform inclusion criteria, the potential for uncontrolled confounding remains. The results obtained have limited applicability to other clinical settings. Because the study was retrospective, sample size calculations were not performed a priori; power was assessed post hoc.