Minovarova Ch. A., Atakhodzhaeva G. A.
Tashkent State Medical University, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
105 patients with arterial hypertension of I - III degree of young age from 18 to 44 years were examined. The results of bioimpedance analysis in patients with arterial hypertension and abdominal obesity revealed significant differences in parameters according to the data of metabolographic and bioimpedancemetric analysis indicating an unfavorable metabolic and cardiovascular profile of patients with hypertension with abdominal obesity, as well as low metabolic activity of adipose tissue, predominance of carbohydrate metabolism and insufficient ability to oxidize fats.
Keywords:
Arterial hypertension, Young age, Abdominal obesity, Metabolography, Bioimpedancemetry
Cite this paper: Minovarova Ch. A., Atakhodzhaeva G. A., Assessment of the State of Metabolic Activity in Young Patients with Arterial Hypertension Against the Background of Abdominal Obesity, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4219-4224. doi: 10.5923/j.ajmms.20251512.06.
1. Introduction
According to WHO experts, the spread of overweight and obesity among young people and adolescents has reached epidemic proportions in recent years. Epidemiological studies show that up to 32% of young people in economically developed countries are obese or overweight. At the same time, the prevalence of obesity in the global population continues to grow. The criticality of the situation is due to the fact that along with the prevalence of obesity, the incidence of concomitant diseases increases, in particular, cardiovascular diseases, which are currently the leading cause of death worldwide [4,12,14].A sharp increase in the incidence of overweight and obesity in young people was first noted in the 1980s, followed by a rise in the incidence of hypertension and prehypertension. Trends in blood pressure values lag behind the dynamics of BMI values by approximately 10 years, which apparently explains a certain variability in the relationship between blood pressure and BMI. Long-term trends in changes in these indicators in young people indicate a relationship between overweight and hypertension [4,13,14].A total of 105 patients with arterial hypertension (AH) of stage I - III (According to the classification of the recommendations of the European Society of Hypertension and the European Society of Cardiology) of young age (according to the WHO classification of 2023 [2,11] from 18 to 44 years old) were examined. The examination of patients with AH was carried out in the departments of interventional cardiology and cardiac rehabilitation of the Republican Scientific and Practical Medical Center for Therapy and Medical Rehabilitation of the Republic of Uzbekistan (Scientific and Practical Medical Center for Therapy and Medical Rehabilitation of the Republic of Uzbekistan) from 2023 to 2024. All examined patients with AH, depending on the presence of abdominal obesity (AO) (based on measuring waist circumference (WC): more than 102 cm in men, more than 88 cm in women, determining the body mass index (BMI) ≥30 kg / m 2 and the waist-to-hip ratio (WHR): in men > 0.95 and in women >0.85 U.S.) were divided into 2 study groups: Group 1 consisted of patients with grade I – III hypertension without AO (n = 55) and Group 2 consisted of patients with grade I – III hypertension with AO (n = 50) (Fig. 1).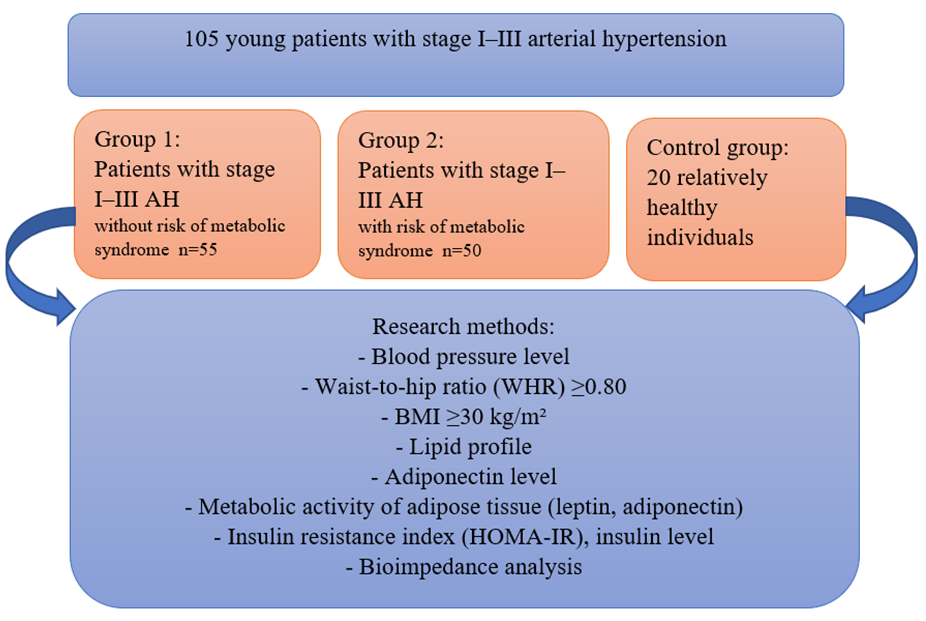 | Figure 1. Study design |
The average age of patients in the 1st group was 26.7±4.5 years, and in the 2nd group 32.8±3.4 years (p<0.01). The duration of hypertension in patients in the 1st group was 2.45±2.22, in the 2nd group 3.48±2.31 years, without statistically significant difference (p>0.05).The gender distribution by groups was as follows: in the 1st group, the number of men was 23 (39.7%) and women 35 (60.3%), in the 2nd group of patients with hypertension and AO, there were slightly more men than women and amounted to a ratio of 37 (55.2%) to 30 (44.8%).According to the oral survey of the clinical history of young patients, a burdened heredity for hypertension in the 1st study group was detected in 29 patients (50%), in the 2nd group in 36 (54%) patients. Also, from the risk factors for hypertension, smoking was detected in 23 (40%) in the 1st study group and in 35 (52%) in the 2nd group of examined patients with hypertension of I-III degree.All patients in the 2nd group had various degrees of obesity, such as 1 degree of obesity (BMI) ≥30-34.9 kg/m2 was observed in 23 (34.3%) patients, 2 degree obesity (BMI) ≥35-39.9 kg/m2 in 31 patients (46.3%) and 3rd degree obesity (BMI) ≥40 kg/m2 was observed in 13 (19.4%) examined patients with hypertension of young age. BMI in the 1st and 2nd groups was 25.4±2.62 and 37.8±4.31 kg/m2, which was 29.13% higher than the data of the 1st study group (p<0.01). The values of waist circumference (WC, cm) in patients of the 1st and 2nd groups were 91.26±3.21 cm and 106.8±9.54 cm, respectively, exceeding the data of the 1st group with hypertension without obesity by 17% (p<0.01). The waist-to-hip ratio (WHR, c.u.) in the 2nd group was 16.5% higher than the data in the 1st study group and amounted to 0.85±0.05 and 0.99±0.07 (p<0.01), respectively.Exclusion criteria: secondary forms of obesity and hypertension, stage III hypertension, diabetes mellitus, autoimmune diseases, bronchial asthma, oncological diseases, neurological pathology, mental disorders, cardiovascular pathology (coronary heart disease, chronic heart failure (CHF), previous myocardial infarction, high-grade heart rhythm disturbances), occlusive peripheral arterial disease, severe liver dysfunction (increase in transaminases more than two reference values), pregnancy, lactation, statins, allergic reactions to antihypertensive drugs, refusal to participate in the study, presence of inflammatory diseases of the myocardium.Body mass index assessment: BMI = Weight (kg) /body area (height 2) (m 2)(https://www.gensio.ru/tools/health/whr-calculator).Waist circumference (WC) assessment to identify abdominal obesity - measurement is taken horizontally, at the navel level. Standard waist circumference values (https://www.gensio.ru/tools/health/whr-calculator):for men: > 102 cm or > 94 cm (depending on source). for women: > 88 cm or > 80 cm (depending on source).Calculation of the WHR ratio (Waist - Hip Ratio) or OT/OB (waist-to-hip ratio) is an indicator that is calculated by dividing the waist size by the hip size. Normal WHR values: for men: WHR < 0.9, for women: WHR < 0.85 (https:// www. gensio. ru / tools / health / whr - calculator).The blood biochemistry study included measurement of total cholesterol, high-density lipoprotein cholesterol (HDL), triglycerides (TG) and fasting blood glucose. All analyses were performed using the state-of-the-art SYNCHRON CX SYSTEMS “BECKMAN” automatic biochemical analyzer.Bioimpedance analysis (BIA) is a non-invasive method of assessing body composition, allowing to determine the amount of fat, muscle, active cell mass and water in the body. The bioimpedancemetry method was performed on Meta equipment Lyzer 3 B - R 2 in the functional diagnostics department at the Republican Scientific and Practical Center for Sports Medicine. The following bioimpedancemetry indicators were calculated: BMI, fat mass (%), visceral fat (points), volume of water component (%), volume of muscle mass (SMM) (%), basal metabolism (BMR) [1,5,6].The metabolography method was carried out on the Meta Lyzer 3B-R2 device in the functional diagnostics department at the Republican Scientific and Practical Center for Sports Medicine. The most important metabolography indicators were calculated: VO ₂ (oxygen consumption), VCO ₂ (carbon dioxide release, RQ (Respiratory Quotient (respiratory quotient) is the ratio of the volume of carbon dioxide to the volume of oxygen, RMR (Resting Metabolic Rate (resting metabolic rate) is the amount of energy that the body spends in a state of complete rest to maintain basic functions (breathing, circulation, thermoregulation) [7].The data obtained during the study were subjected to statistical processing on a Pentium - IV personal computer using the Microsoft software package. Office Excel -2012, including the use of built-in statistical processing functions. Comparison of three or more independent groups was carried out by one-factor analysis of variations ANOVA. The level of reliability P<0.05 was taken as statistically significant changes.
2. Research Results
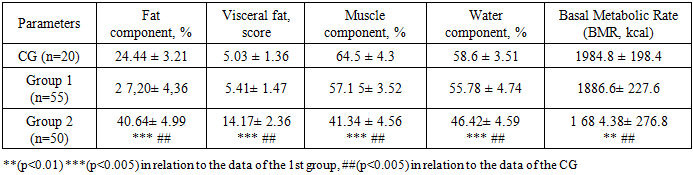
To determine the amount of fat, muscle, active cell mass and water in the body, we used a non-invasive method for assessing body composition - bioimpedancemetry, which reveals characteristic disorders: high levels of visceral fat, decreased muscle and active cell mass, and water balance disorders. The results of bioimpedance analysis in patients with hypertension and abdominal obesity revealed significant differences between the parameters of groups 1 and 2, as well as between the CG and group 2 data. Young patients in group 1 with hypertension without obesity had statistically insignificant differences in bioimpedance analysis data compared to the control group data (p> 0.05). At the same time, patients in group 2 with hypertension and obesity differed significantly in the parameters of the fat component by 66.3%, the muscle component by 56.02% and the water component by 26.3%, in contrast to the CG data (p<0.005). The volume of visceral fat in patients with hypertension and AO was significantly higher by 2.8 times (p<0.005) compared to the CG data. The level of basal metabolism (BMR, kcal) in young patients of the 2nd group with hypertension and AO was 1684.38±276.8 versus 1984.8±198.4 (p<0.01).The results of the analysis of intergroup differences in bioimpedance analysis parameters in young patients with hypertension depending on the presence of AO had the following values: Fat component is 49.4% higher; muscle component is less than 38.2%; water component is 20.2% less (p<0.005). The volume of visceral fat in patients with hypertension and AO was significantly 2.6 times higher (p<0.005) compared to the data of the 1st study group with hypertension without AO. The level of basal metabolism (BMR, kcal) in young patients of the 2nd group with hypertension and AO was 1684.38±276.8 versus 1886.6±227.6 (p<0.01), which was 12.0% lower compared to the data of the 1st group (Table 1). The changes revealed by bioimpedance analysis indicate an unfavorable metabolic and cardiovascular profile in patients with hypertension and abdominal obesity.Table 1. Results of bioimpedance analysis in patients with arterial hypertension and abdominal obesity
 |
| |
|
A study evaluating the effect of aerobic and strength PE [1,5] on BIA indices demonstrated a significant decrease in FMT and impedance values when measuring immediately after training on a segmented 8-point analyzer. This confirms that physical exercise, regardless of the energy supply mode (aerobic or anaerobic), has a significant effect on body composition indices and assessment of the body's hydration status, thereby supporting traditional recommendations for compliance with standard measurement conditions in terms of excluding PE before conducting the examination. The same authors, similar to the previous study, showed that after a 30-minute cyclic load on a stationary bike, the proportion of FMT statistically significantly decreases, and this decrease directly depends on the intensity of the training [1].Changes in bioimpedance analysis indices in clinical conditions. M. R. Scheltinga et al. (1991) observed changes in BIA indices after intravenous infusion of 1 l of physiological solution, as well as after donation of 48 ml of blood. Infusion of 1000 ml of physiological solution for 15 min affected the BIA results by significantly decreasing resistance and significantly increasing the total body water index; at the same time, donation of 480 ml of blood caused the opposite changes – the resistance of the body increased significantly and the total body water index decreased significantly [1].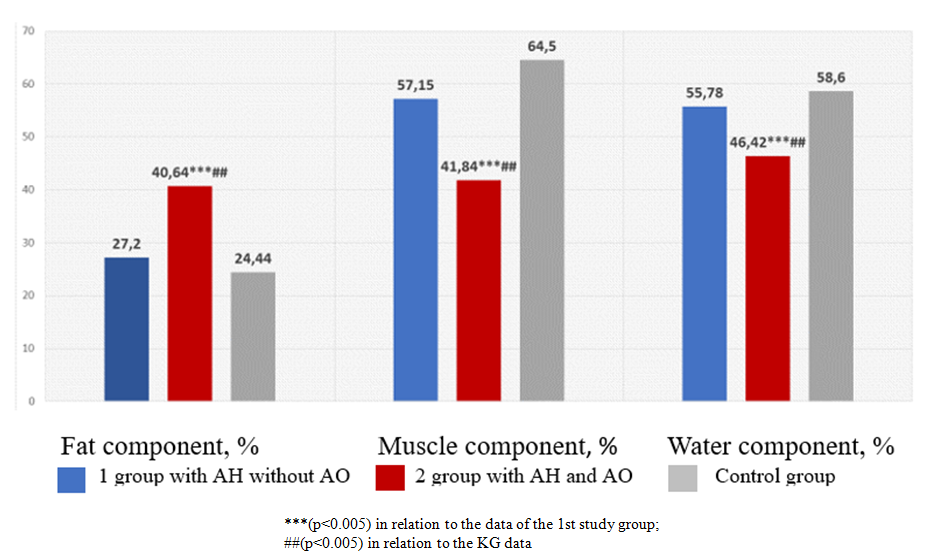 | Figure 2. Results of bioimpedance analysis in patients with arterial hypertension and abdominal obesity |
Next, to assess the key parameters of metabolic activity and the basic level of energy needs of patients with hypertension of young age, we conducted a metabolographic study method - RMR (Resting Metabolic Rate (resting metabolic rate), that is, an assessment of the amount of energy that the body spends in a state of complete rest to maintain basic functions (breathing, circulation, thermoregulation).The results of the study showed that in patients with abdominal obesity, despite the high total RMR, it was 27.7% lower than in the control group (p<0.005) and 13.3% lower than in the 1st group (p<0.01) (Fig. 3). At the same time, a decrease in specific energy expenditure per kg of body weight was also noted compared to the control group by 45.1% (p<0.005) and by 20.7% (p<0.005) compared to the data obtained in the 1st study group. This is due to the low metabolic activity of adipose tissue in young patients with hypertension and AO.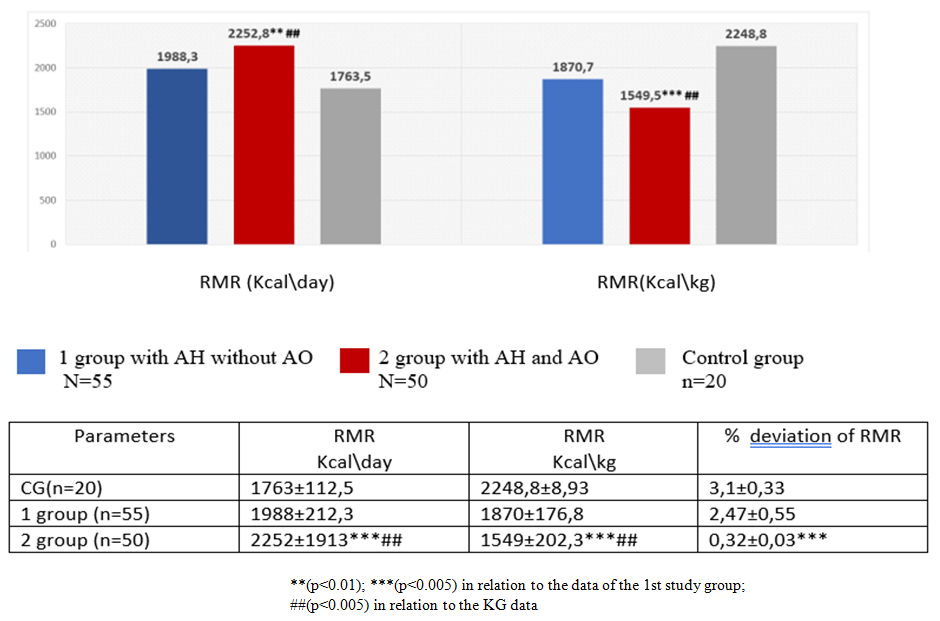 | Figure 3. Results of the metabolographic study of RMR (Resting Metabolic Rate) in patients with hypertension and AO of young age |
In patients with hypertension and abdominal obesity of young age, a decrease in VO ₂ - the volume of oxygen consumption due to low physical activity and reduced muscle mass was observed. The value of VO ₂ (ml / min) in the 2nd study group statistically significantly differed from the control group data by 33.6% (p<0.005) and by 21.2% from the data of the 1st study group (p<0.005). The VO ₂ (ml / kg / min) indicator of the 2nd study group had statistically significant differences in relation to the control group data by 37.25% and by 21.6% in relation to the data of the 1st study group (p<0.005).CO ₂ released (VCO ₂ - ml/min) in the 2nd group with hypertension and obesity also had statistically significant differences in relation to the CG data by 17.8% and by 12.6% in relation to the 1st study group data (p<0.01) (Fig. 4). The revealed moderate increase in VCO ₂ (carbon dioxide release) in patients of the 2nd group with hypertension and obesity at rest is a sign of increased glucose metabolism.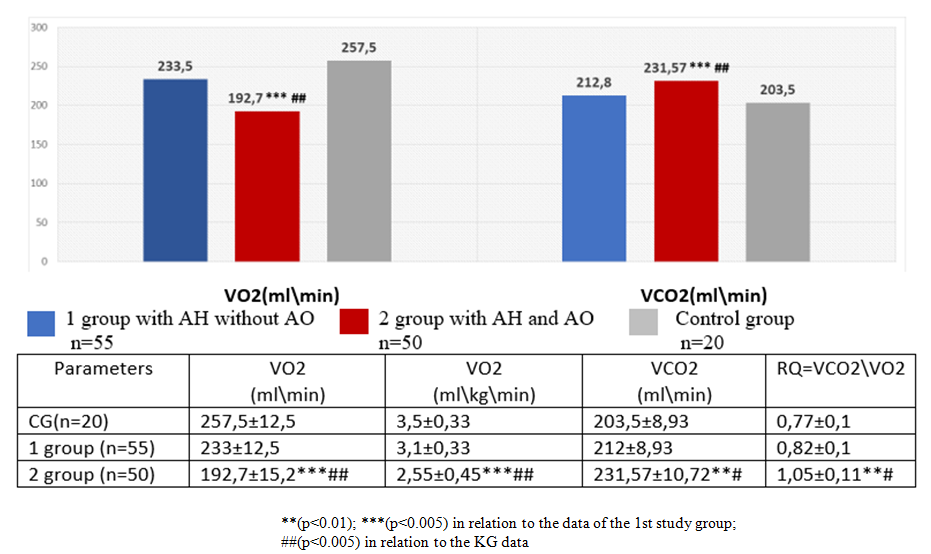 | Figure 4. Results of the metabolographic study of RMR (Resting Metabolic Rate) in patients with hypertension and AO of young age |
A meta-analysis by Naci et al. [15], which included 391 randomized controlled trials (RCTs), found that aerobic exercise reduced BP in a similar manner to antihypertensive drugs [8]. Overall, 33 systematic reviews (including 25 meta-analyses) covering healthy individuals and individuals with health complications found that high-intensity aerobic exercise (high - intensity interval High intensity intra-intensive training (HIIT) improved cardiorespiratory fitness, anthropometric parameters, vascular function, cardiac function, and muscle mass compared to inactive controls [3].Thus, an increased RQ value (>0.9) (Respiratory Quotient is a respiratory coefficient, which indicates the prevalence of carbohydrate metabolism and insufficient ability to oxidize fats. The results of the analysis of metabolographic data of young patients with hypertension and obesity noted a significant decrease in this coefficient by 36.4% and 28.0%, respectively, compared with the data of the CG and the 1st study group. The obtained metabolographic data between patients of the 1st study group with hypertension without obesity and with the data of healthy individuals of the CG did not have statistically significant differences.
3. Conclusions
• The results of bioimpedance analysis in patients with arterial hypertension and abdominal obesity revealed significant differences in the parameters of the fat component: 49.4% higher; muscle component less than 38.2%; water component less than 20.2% (p<0.005), a decrease in the level of basal metabolism (BMR, kcal) by 12.0% (p<0.005), compared with the data of the 1st group, which indicates an unfavorable metabolic and cardiovascular profile of patients with hypertension and abdominal obesity.• Significant reduction in specific energy expenditure of the body according to the RMR study (Resting Metabolic Rate) in patients with abdominal obesity indicates low metabolic activity of adipose tissue. In patients with hypertension and abdominal obesity of young age, there was a decrease in VO ₂, - the volume of oxygen consumption (21.6%; p<0.01) due to low physical activity and reduced muscle mass, an increased RQ value (20.8; p<0.01), which indicates the predominance of carbohydrate metabolism and insufficient ability to oxidize fats.
References
| [1] | Vybornaya K.V., Nikityuk D.B. Bioimpedance analysis in sports and clinical practice: the influence of alternative measurement conditions on body composition indicators // Nutrition Issues. 2025. Vol. 94, No. 1. Pp. 6–20. DOI: https://doi.org/10.33029/0042-8833-2025-94-1-6-20. |
| [2] | ESH / ESC 2018 clinical guidelines for the diagnosis and management of patients with arterial hypertension: a first look. Arterial hypertension. 2018; 24(3): 351–358. |
| [3] | Miroshnikov A. B., Formenov A. D., Smolensky A. V. Effect of uniform and high-intensity interval training in cardiac rehabilitation of bodybuilders with arterial hypertension: a randomized controlled trial // Bulletin of Restorative Medicine. 2020. No. 6 (100). |
| [4] | Mustafayeva A.G. Mechanisms of development of arterial hypertension in young individuals with overweight // Problems of Endocrinology. - 2019. - Vol. 65. - No. 3. - P. 191-196. |
| [5] | Lipid Metabolism Disorders. Clinical Guidelines 2023. Russian Journal of Cardiology. 2023; 28(5): 5471. https://doi.org/10.15829/1560-4071-2023-5471 https://russjcardiol.elpub.ru/jour/article/view/5471/3988?locale =ru_RU). |
| [6] | Nikolaev D.V., Shchelykalina S.P. Bioimpedance analysis of human body composition: medical application, terminology Vol 2 (2) 2021 Clinical nutrition and Metabolism DOI: https://doi.org/10.17816/clinutr72132. |
| [7] | Orazmukh a Medov a A., Azatgeldieva A. METABOLOGRAPH AND ITS INDICATORS FOR DETERMINING THE STATE OF AN ATHLETE DURING REST // Science and Worldview. 2024. No. 30. |
| [8] | Ragino Yu. I., Shcherbakova L. V., Oblaukhova V. I., Blood adipokines in young people with early ischemic heart disease background of abdominal obesity ISSN 0022-9040. Cardiology. 2021; 61(4). DOI: 10.18087/cardio.2021.4. n 1369 pp 32-38. |
| [9] | Rogoza A. N., Oshchepkova E. V., Tsagareishvili E. V., Gorieva Sh. B. Modern non-invasive methods of measuring blood pressure for the diagnosis of arterial hypertension and evaluation of the effectiveness of antihypertensive therapy. Moscow, 2007. 72 p. ISBN: 978-5-98495-010-7. |
| [10] | Khursa R.V., Voitikova M.V. Daily monitoring of arterial pressure using intelligent data analysis: new diagnostic possibilities, HYPERTENSION, ISSN 2224-1485 N ¹2(40)-2015, pp. 40-49, DOI: 10.22141/2224-1485.2.40.2015.80406. |
| [11] | 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH) Received 16 May 2023 Accepted 22 May 2023 J Hypertens / DOI:10.1097/HJH.0000000000003480 https://congress-med.ru/rekomendaczii. |
| [12] | Carbone S, Canada JM, Billingsley HE, Siddiqui MS, Elagizi A, Lavie CJ. Obesity paradox in cardiovascular disease: where do we stand? Vascular Health and Risk Management. 2019; 15: 89–100. DOI: 10.2147/VHRM.S168946. |
| [13] | With hait A, den Hartigh LJ. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Frontiers in Cardiovascular Medicine. 2020; 7: 22. DOI: 10.3389/fcvm.2020.00022. |
| [14] | Krzysztoszek J, Laudańska-Krzemińska I, Bronikowski M. Assessment of epidemiological obesity among adults in EU countries. Annals of Agricultural and Environmental Medicine. 2019; 26(2): 341–9. DOI: 10.26444/aaem/97226. |
| [15] | Naci H, et al. Br J Sports How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomized controlled trials assessing exercise and medication effects on systolic blood pressure Med 2018; 0: 1–12. doi:10.1136/bjsports-2018-099921 http://bjsm.bmj.com/. |
| [16] | Neeland IJ, Ross R, Després JP, Matsuzawa Y, Yamashita S, Shai I et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. The Lancet Diabetes & Endocrinology. 2019; 7(9): 715–25. DOI: 10.1016/S2213-8587(19)30084-1. |
| [17] | O'Brien E, Dolan E. Ambulatory blood pressure monitoring for the effective management of antihypertensive drug treatment. Clin Therapeutics. 2016; 38: 2142-51. doi:10.1016/j.clinthera.2016.08.006. |
| [18] | Staessen J, Amery A. APTH — A trial on ambulatory blood pressure monitoring and treatment of hypertension: objectives and protocol. Acta Cardiol. 1993; 158: 25-42. |
| [19] | Staessen J, Buttebier G, Buntinx F, et al. for the Ambulatory Blood Pressure Monitoring and Treatment of Hypertension Investigators. Antihypertensive treatment based on conventional or ambulatory blood pressure measurement. A randomized controlled trial. JAMA. 1997; 278: 1065-72. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML