-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4216-4218
doi:10.5923/j.ajmms.20251512.05
Received: Sep. 4, 2025; Accepted: Oct. 2, 2025; Published: Dec. 2, 2025

Clinical Evaluation of the Effect of Epidural Analgesia on Renal Function in Patients with Intra-abdominal Hypertension
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBatirov U. B.1, Mirakhmedov G. M.2, Khaydarova S. E.1, Ochiljonov S. M.1
1Center for the Development of Professional Qualifications of Medical Workers
2Multidisciplinary Clinic "Akfa Medline"
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study analyzed clinical data from 45 patients who underwent abdominal surgery. The effectiveness of epidural analgesia as a component of intensive care in patients with intra-abdominal hypertension was evaluated, with particular attention to its impact on renal function. The findings demonstrated that epidural analgesia not only provides effective pain relief but also reduces intra-abdominal pressure and improves glomerular filtration rate and diuresis. Thus, epidural analgesia is considered a significant pathogenetically substantiated method in the comprehensive treatment of intra-abdominal hypertension, exerting a positive influence on renal functional status.
Keywords: Intra-abdominal hypertension, Renal dysfunction, Epidural analgesia, Glomerular filtration rate, Diuresis, Abdominal surgery, Intensive care
Cite this paper: Batirov U. B., Mirakhmedov G. M., Khaydarova S. E., Ochiljonov S. M., Clinical Evaluation of the Effect of Epidural Analgesia on Renal Function in Patients with Intra-abdominal Hypertension, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4216-4218. doi: 10.5923/j.ajmms.20251512.05.
1. Introduction
- The increase in intra-abdominal pressure (IAP) plays a critical role in the development of multiple organ dysfunction syndrome in patients following abdominal surgical interventions [1,2,7,10,13,15]. In addition to impairments of hepatic, pulmonary, and intestinal function, pronounced alterations are observed in renal function. Elevated pressure within the enclosed space of the abdominal cavity leads to compromised regional perfusion, hypoxia, and organ ischemia, resulting in a progressive decline in functional activity, potentially culminating in complete organ failure [3,6,9,11,12,14].The kidneys, due to their high sensitivity to hemodynamic disturbances, are among the first organs to respond to changes in intra-abdominal pressure. According to R. Bellomo (2004) [5], the incidence of renal dysfunction in intensive care units ranges from 5% to 15% [4,8]. However, contemporary studies, including the international WSACS guidelines (2025) [4], indicate that under conditions of intra-abdominal hypertension, the risk of developing acute kidney injury (AKI) is considerably higher—reaching 30–40%—and is frequently accompanied by dysfunction of other organs and systems.Objective:The objective of the present study is to evaluate the effect of epidural analgesia on renal functional status in patients with intra-abdominal hypertension following abdominal surgical interventions.
2. Materials and Methods
- The analysis included 45 patients (22 men and 23 women) diagnosed with generalized peritonitis. The diagnoses serving as inclusion criteria were: generalized peritonitis (n = 18), pancreatic necrosis (n = 10), intestinal obstruction (n = 9), and incarcerated giant ventral hernias (n = 8). The patients’ ages ranged from 18 to 61 years, with a mean age of 42.6 ± 2.16 years. The patients were divided into two groups. The control group (n = 21) received standard postoperative therapy, which included antibacterial agents, systemic analgesics, infusion-transfusion therapy, and gastrointestinal motility stimulants. The main group (n = 24), in addition to the standard treatment, received epidural analgesia with 1% lidocaine solution administered at a dose of 0.8 mg/kg every 4 hours. In both groups, the following parameters were recorded: Renal function indicators: hourly diuresis, serum urea and creatinine levels, and glomerular filtration rate (GFR), calculated using the CKD-EPI formula. Pain intensity: assessed using the verbal rating scale (VRS), ranging from 0 to 10 points. Intra-abdominal pressure (IAP): measured using the I. Kron method via Foley catheter following instillation of 30 mL of sterile saline, with a Waldman hydromanometer. Pressure readings were taken relative to the upper edge of the pubic symphysis.All parameters were assessed dynamically at 24, 48, and 72 hours postoperatively.Statistical analysis was performed using SPSS v.26.0 software. For comparison of quantitative variables between the two independent groups, Student’s t-test was used for normally distributed data, and the Mann–Whitney U-test was applied when normality assumptions were not met. Categorical variables were analyzed using the χ² test. Statistical significance was established at p < 0.05.
3. Results and Discussion
- The conducted analysis revealed positive dynamics in intra-abdominal pressure (IAP) and renal function parameters in both groups during intensive care. However, more pronounced and sustained improvements were observed in patients of the main group who received epidural analgesia.In the main group, the mean IAP, which initially measured 21.3 ± 1.24 mm Hg, decreased to 15.7 ± 1.21 mm Hg within 24 hours after initiation of therapy (p < 0.05) (see Table 1). In the control group, no significant reduction in IAP was noted during the first 24 hours; statistically significant changes were observed only by the second postoperative day (p < 0.05).Patients in the main group demonstrated significant improvement in renal perfusion and functional indicators. The glomerular filtration rate (GFR) increased from 52.4 ± 2.63 mL/min to 103.1 ± 1.29 mL/min, while hourly urine output rose from 42.1 ± 2.54 mL/h to 68.5 ± 2.83 mL/h. Serum urea levels showed a statistically significant decrease only by the second day of observation compared to baseline (14.2 ± 1.31 mmol/L; p < 0.05). A similar positive trend was recorded for serum creatinine levels (see Table 1).
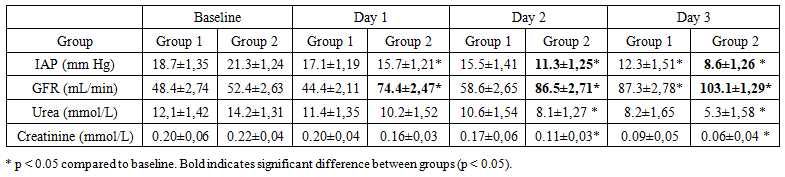 | Table 1. Dynamics of Intra-Abdominal Pressure, Glomerular Filtration Rate, Urea, and Creatinine |
4. Conclusions
- The results of the present study demonstrate the high efficacy of epidural analgesia as part of comprehensive intensive care in patients with intra-abdominal hypertension following abdominal surgery. The application of this method significantly reduces intra-abdominal pressure and improves renal function, as evidenced by increased diuresis and glomerular filtration rate. At the same time, normalization of nitrogenous blood metabolites (urea and creatinine) occurs after 48 hours or more, which should be taken into account when clinically evaluating treatment effectiveness.The obtained data support the rationale for incorporating epidural analgesia into standard management protocols for patients at risk of multiple organ failure associated with intra-abdominal hypertension.