-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4206-4211
doi:10.5923/j.ajmms.20251512.03
Received: Oct. 14, 2025; Accepted: Nov. 8, 2025; Published: Dec. 1, 2025

Comparative Morphological Study of Flat and Verrucous Forms of Oral Leukoplakia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRizaev J. A.1, Absalamova N. F.2, Akhmedova S. M.3
1Professor, Rector of Samarkand State Medical University, Doctor of Medical Sciences, Uzbekistan
2Independent Researcher, Samarkand State Medical University, Associate Professor of the Department of Clinical Disciplines Alfraganus University, PhD, Uzbekistan
3Professor, Department of Human Anatomy of Tashkent State Medical University, Doctor of Medical Sciences, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study included 92 individuals. OCT images of different anatomical regions of the oral mucosa were obtained in all subjects and compared with morphological analysis results. Morphometric parameters assessed included epithelial thickness, epithelial papilla height, number and diameter of blood vessels, basement membrane thickness, and collagen fiber density. Compared with the control group, leukoplakia cases showed a significant increase in epithelial thickness and papilla height. The number of blood vessels also increased. OCT images demonstrated epithelial thickening and increased brightness in the flat form, while the verrucous form showed irregular margins and verrucous projections. In cases of malignant transformation, the layered structure disappeared, the image became homogeneous, and the informative depth was less than 1 mm.
Keywords: Oral mucosa, Leukoplakia, Precancerous lesion, Optical coherence tomography (OCT), Hyperkeratosis, Acanthosis, Malignant transformation
Cite this paper: Rizaev J. A., Absalamova N. F., Akhmedova S. M., Comparative Morphological Study of Flat and Verrucous Forms of Oral Leukoplakia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4206-4211. doi: 10.5923/j.ajmms.20251512.03.
1. Introduction
- Leukoplakia is one of the most common and clinically significant precancerous disorders of the oral mucosa. According to the World Health Organization, a considerable proportion of precancerous lesions in the oral cavity are attributed to leukoplakia, with malignant transformation observed in approximately 3–20% of cases [1]. Hence, its early detection and continuous monitoring remain critical challenges in modern dentistry and oncology. Clinically, leukoplakia presents in several forms—flat, verrucous, and erosive—each demonstrating distinct morphological and morphometric features of the epithelium [3]. Conventional diagnostic approaches, including cytology and biopsy, remain the gold standard; however, they are invasive and often limited to late-stage detection [2].Recently, optical coherence tomography (OCT) has emerged as a valuable non-invasive diagnostic tool in dental practice. It enables the assessment of the epithelial and stromal layers and the identification of early pathological changes such as hyperkeratosis and acanthosis without requiring tissue sampling [4]. Correlating OCT findings with histological and morphometric data enhances diagnostic accuracy, contributing to early identification of at-risk patients [7]. Thus, the integration of OCT data with morphological and morphometric analysis represents a scientifically and clinically significant advancement, improving the early diagnosis, monitoring, and prevention of precancerous lesions of the oral mucosa. [5]The purpose of this study is to compare images obtained by optical coherence tomography with morphological and morphometric indicators in cases of oral mucosal leukoplakia.Materials and methods. The study was conducted at the dental clinic of Samarkand State Medical University. A total of 92 patients were involved in the examination, aged 19 to 70 years, including 55 women and 37 men. The main group included 76 patients with clinically and histologically confirmed leukoplakia of the oral mucosa. The control group consisted of 16 clinically healthy individuals with no pathological changes in the oral mucosa and free from dental and somatic diseases. [6]Optical coherence tomography was used in all examinations. For OCT diagnostics, a Swept-Source OCT (SS-OCT) system from Novacam Technologies (Canada) was used, with a signal wavelength of 1300 nm and a tissue depth resolution of 7–10 μm. OCT images were obtained from various anatomical regions of the oral cavity: the labial mucosa, cheeks, dorsal surface of the tongue, hard palate, and gingiva. At least 5 different zones were imaged in each patient, and they were comparatively analyzed for normal and pathological changes.For morphological analysis, biopsy materials were taken from patients in the main group based on clinical indications. In the control group, biopsy was not performed for ethical reasons; for morphological comparison, normal histological preparations from the pathoanatomical archive and excess tissue fragments removed during surgical procedures were used. [8]The obtained biopsies were fixed in 10% formalin, and paraffin blocks were prepared. Histological slides were stained with hematoxylin-eosin, and in additional cases, with the Van Gieson method. Morphometric analysis was performed using a microscope (Olympus BX51), images were digitized, and analyzed using the ImageJ software.The following were studied as morphometric indicators:• Epithelial thickness (μm);• Basement membrane thickness (μm);• Epithelial papilla height (μm);• Number and diameter of blood vessels (per 1 mm² area);• Collagen fiber density (arbitrary units);• Average diameter of glandular acinar structures (μm).All data were processed using the Statistica 10.0 software. Mean value (M), standard deviation (SD), and confidence intervals (CI) were calculated. Differences between groups were assessed using Student's t-test and the Mann–Whitney criterion. The significance level was accepted as p<0.05.
2. Materials and Methods
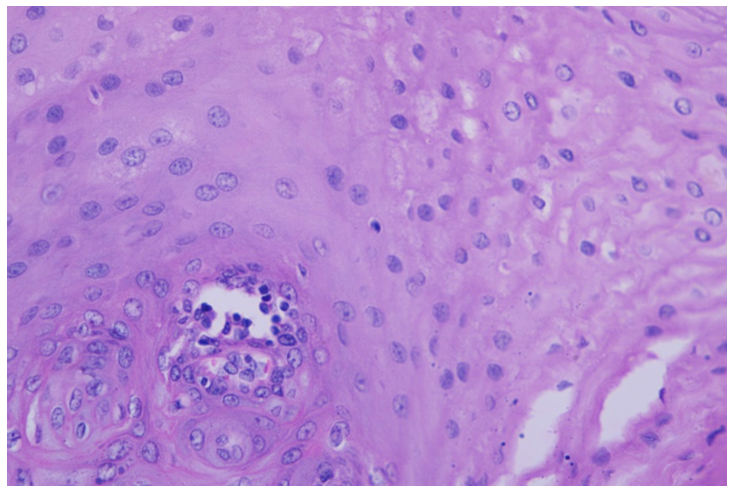
- In the control group, OCT tomograms of the oral mucosa demonstrated a distinct two-layered structure. The upper layer corresponded to the stratified squamous epithelium, showing moderate brightness and uniform optical density, while the lower layer represented the connective tissue with higher brightness and heterogeneous signal intensity. The boundary between the epithelial and stromal layers was clear, smooth, and continuous, serving as a normal morphological standard. Within the lower layer, small hypoechoic regions of variable brightness were detected, corresponding to blood vessels and mucosal glands. The informative imaging depth was typically 1.0–1.2 mm and approximately 0.5–0.6 mm in the alveolar mucosa. Histological analysis fully corroborated the OCT findings. Microscopic examination revealed stratified squamous hyperkeratotic epithelium with an average thickness of 250–320 μm, while in the hard palate and gingiva, this thickness reached 400–450 μm. The basement membrane remained intact, and the epithelial-stromal boundary was distinctly visible. In the stroma, collagen fibers were densely packed and predominantly oriented horizontally, with deep connections to the epithelial ridges. The mean vessel diameter ranged from 18–26 μm, with an average of 22 ± 3 vessels per 1 mm². Glandular acinar structures appeared intact, averaging 28 ± 4 μm in diameter. Morphometric evaluation indicated that the mean epithelial thickness was 280 ± 25 μm, 410 ± 30 μm in the gingiva, and 260 ± 20 μm in the labial mucosa. The basement membrane thickness ranged between 0.8–1.2 μm, and epithelial ridge height averaged 65 ± 10 μm. The collagen fiber density was calculated at 0,68 ± 0,05 arbitrary units. These findings established the morphological and morphometric reference parameters for the oral mucosa in the control group. The consistency between OCT imaging and histological analysis confirmed the two-layered architecture of the normal mucosa, the integrity of the basement membrane, and the structural harmony between the epithelium and stroma. This dataset serves as a reliable baseline for comparison with leukoplakia cases in the main group. Comparative evaluation of OCT and histological data revealed that leukoplakia, a common precancerous lesion of the oral mucosa, presents with distinct clinical and morphological variants. Flat leukoplakia predominantly occurs in regions of hyperkeratotic epithelium, maintaining a relatively preserved layered structure. OCT scans showed two horizontal layers: the upper layer—representing hyperplastic, stratified squamous epithelium—appeared brighter and thicker than normal, while the lower layer corresponded to connective tissue with increased reflectivity. Histological findings included acanthosis, parakeratosis, irregular epithelial ridges, local proliferative activity in the basal layer, and focal epithelial atypia. The subepithelial stroma exhibited diffuse or focal lymphomacrophagal infiltration.Verrucous leukoplakia demonstrated more pronounced pathological alterations in both OCT and histological assessments. Tomograms revealed an uneven, elevated upper boundary due to verrucous epithelial projections, with partial disturbance of the normal layered pattern. The upper layer displayed marked hyperkeratosis and acanthosis, while the lower layer contained hypoechoic regions corresponding to vascular and inflammatory elements. Histological sections showed a markedly thickened keratin layer, epithelial hyperplasia, and dyskeratosis in individual cells. The stratified squamous epithelium exhibited irregular thickening and focal distortions. Epithelial cells displayed nuclear enlargement, hyperchromasia, and an increased nuclear-to-cytoplasmic ratio, indicative of dysplastic transformation. The basement membrane was preserved but locally thickened. The underlying stroma revealed dense fibrosis with thick collagen bundles and sclerosis. Chronic inflammatory infiltrates—mainly lymphocytes with occasional neutrophils—were concentrated around dilated blood vessels, forming perivascular cuffs (Figure 1).
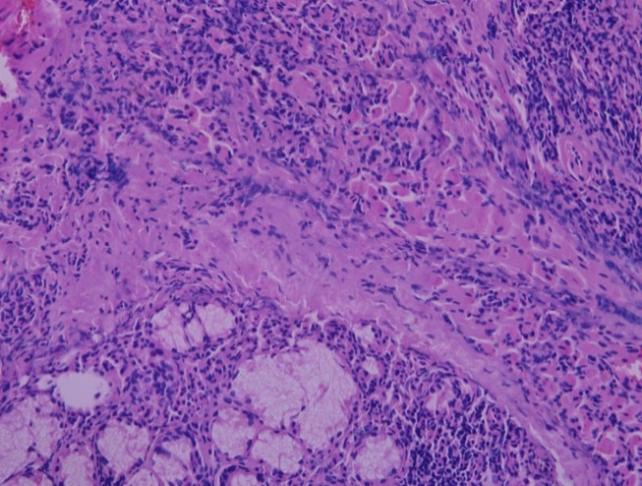 | Figure 1. The epithelial cells show nuclear enlargement, hyperchromasia, and an increased nuclear-to-cytoplasmic ratio, suggestive of dysplastic alterations. The basement membrane is preserved but focally thickened. Stain H.E. Magnification 40x10 |
3. Results and Discussions
- These morphological features are consistent with chronic inflammation of the oral mucosa associated with verrucous or erosive forms of leukoplakia, where prolonged irritation and epithelial remodeling are accompanied by stromal fibrosis and cellular infiltration (Figure 2).
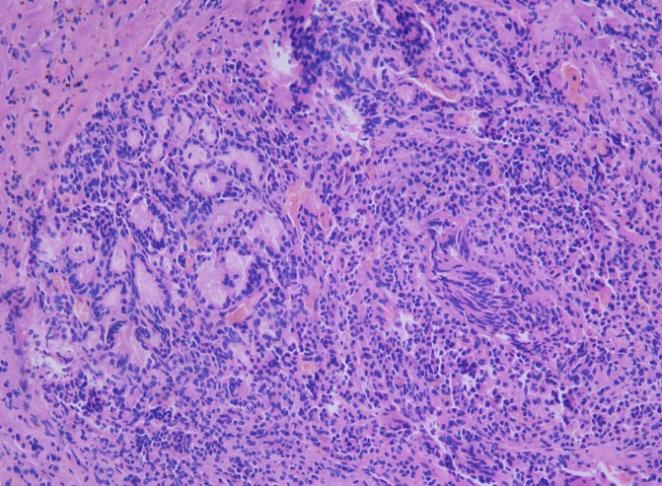 | Figure 2. Histological section of the oral mucosa with leukoplakia/ Pronounced lymphomacrophagal infiltration, focal epithelial hyperplasia, and perivascular inflammatory cuffs indicate chronic inflammatory changes typical for verrucous leykoplakia. Stain H.E. Magnification 40x10 |
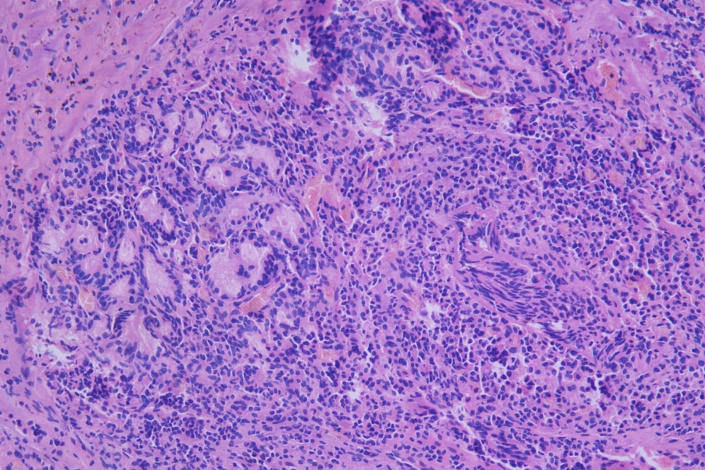 | Figure 3. Leukoplakia in the oral mucosa. Lymphomacrophagal infiltration under the epithelium, presence of dyskeratosis in some cells, and signs of atypia are noticeable. Accumulation of inflammatory cells in the stroma and infiltration around blood vessels are noted. Stain H.E. Magnification 40x10 |
|
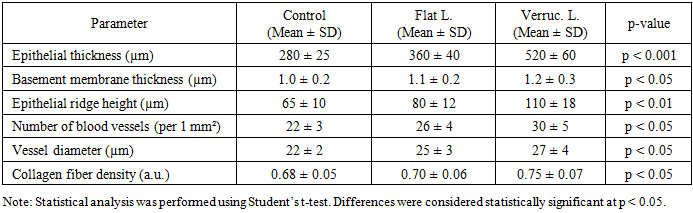
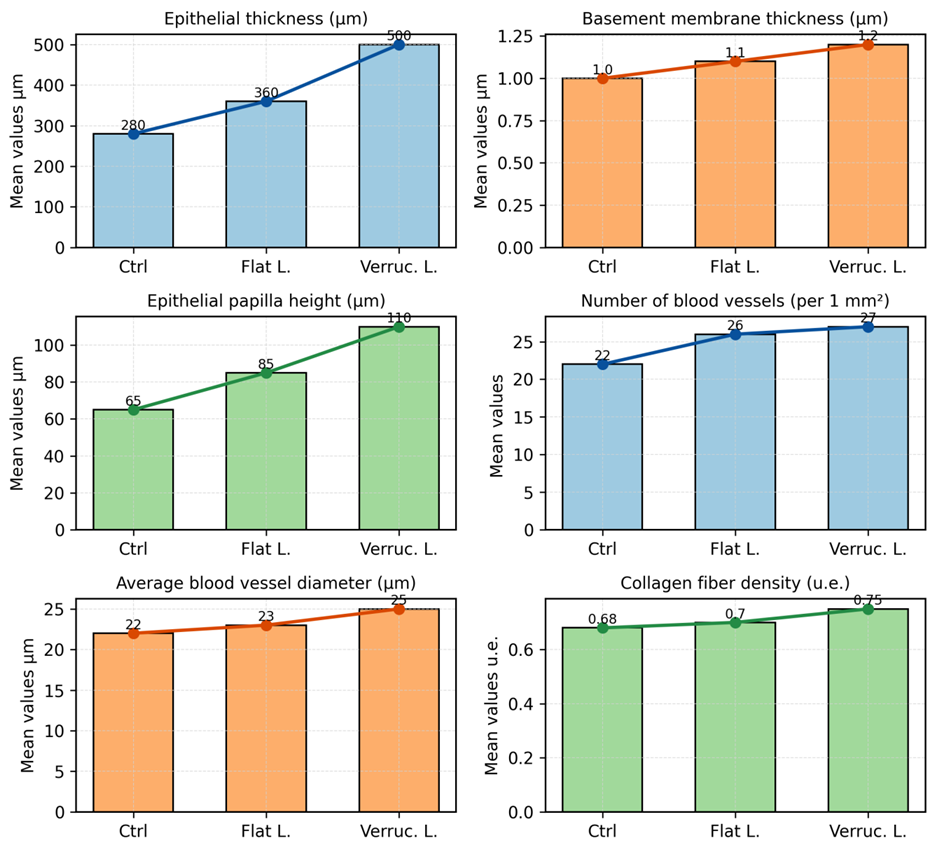 | Figure 4. Morphometric indicators of the oral mucosa (mean ± SD) |
 | Figure 5. Flat leukoplakia in the oral mucosa. The layers of multilayered squamous epithelium are thickened, signs of hyperkeratosis between cells and dyskeratosis in some cells are observed. Stain H.E. Magnification 40x10 |
4. Conclusions
- According to the obtained results, significant changes in morphometric indicators in the epithelium and stroma were identified in cases of oral mucosal leukoplakia. In flat and verrucous forms, epithelial thickness, papilla height, and the number of blood vessels were higher compared to the control group. OCT diagnostics were consistent with morphological analysis, reflecting the integrity of the layered structure in the control group, and hyperkeratosis, acanthosis, and boundary disruption in leukoplakia cases. In malignization processes, the loss of layered structure and uniformity of the optical signal were noted as reliable signs of cancer transformation.Thus, the OCT method is an effective non-invasive diagnostic tool for early detection of precancerous processes in the oral mucosa, stratification of patients into risk groups, and dynamic monitoring.