-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(12): 4197-4202
doi:10.5923/j.ajmms.20251512.01
Received: Aug. 4, 2025; Accepted: Sep. 2, 2025; Published: Dec. 1, 2025

Comparison of Morphological and Morphometric Changes in the Thymus Following Neuroprotective Correction of Traumatic Brain Injury
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAхmedova Shakhlo Malikovna
Department of Endocrinology, Bukhara State Medical Institute, 23 Gijduvan street, Bukhara, Uzbekistan
Correspondence to: Aхmedova Shakhlo Malikovna, Department of Endocrinology, Bukhara State Medical Institute, 23 Gijduvan street, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Traumatic brain injury is a leading cause of death and disability worldwide. Although many experiments have been successfully conducted in rodent models of experimental TBI, all pharmacological agents used to date have failed to improve outcomes in clinical trials. Clinical TBI is characterized by a diverse nature, biomechanics of injury, site of injury, severity, and clinical features, with individual differences. Marie Hanscom and co-authors (2021) observed strong activation of the sympathetic nervous system (SNS) after traumatic brain injury (TBI) in their study. The resulting hyperadrenergic state was systematically associated with immunomodulation in the brain. Post-TBI dysregulation enhanced inflammation, that is, secondary brain injury, which aggravated the patients’ condition and, in some cases, resulted in death. The aim of this study was to assess circulating inflammatory cytokines (the early dynamic state of chemokines) in patients with moderate and severe TBI, as well as to evaluate the severity of injury and clinical indicators of neurological symptoms. The obtained experimental and clinical results indicated that inflammation is an integral component of the pathogenesis of secondary injury following traumatic brain injury.
Keywords: Brain injury, Neuroprotectors, Correction, Hassal corpuscles, Thymocytes
Cite this paper: Aхmedova Shakhlo Malikovna, Comparison of Morphological and Morphometric Changes in the Thymus Following Neuroprotective Correction of Traumatic Brain Injury, American Journal of Medicine and Medical Sciences, Vol. 15 No. 12, 2025, pp. 4197-4202. doi: 10.5923/j.ajmms.20251512.01.
1. Introduction
- Traumatic brain injuries (TBI) are one of the leading causes of death and disability worldwide. Although numerous experiments using experimental TBI models in rodents have been successfully completed, to date, all pharmacological agents applied have failed to improve outcomes in clinical trials. The heterogeneous nature of clinical TBI — including differences in injury biomechanics, location, severity, and clinical features — is characterized by significant individual variability. Therefore, therapies capable of influencing not only a single pathophysiological mechanism but multiple mechanisms simultaneously may be the most effective in improving clinical outcomes of TBI [1,2].According to the scientific literature, over the past decade, the understanding of the pathophysiological processes of traumatic brain injury (hypoxia, hypotension, increased intracranial pressure, and other factors that cause secondary damage to brain tissue) has significantly improved, which in turn has allowed us to base new directions on treatment. The results of modern research on the physiology and pharmacology of the nervous system have proven the need for neuroprotectors as the main treatment [4]. Magnesium-containing drugs are widely used to improve organic and functional changes in brain cells caused by various internal and external factors. One of the most common of these is magnesium sulfate. This drug is one of the most effective pharmacological agents for protecting the brain. Magnesium plays an important role in the vital activity of brain cells. Its neuroprotective effect has been demonstrated in experimental models of stroke and traumatic brain injury. Another advantage of magnesium sulfate is its pleiotropic effect. Most other neuroprotective agents affect only one pathophysiological process. The neuroprotective effect of magnesium is achieved through a number of mechanisms, including: non-selective blockade of N-methyl D-aspartate (NmDa) receptors, reduction of presynaptic excitatory neurotransmitter release, and blockade of calcium channels associated with inhibition and amplification of depolarizing waves in the cerebral hemispheres. Magnesium sulfate helps reduce intracranial pressure. It is also widely used in traumatic brain injury, subarachnoid hemorrhage, ischemic stroke, eclampsia and preeclampsia, hypoxia of the central nervous system, and central paralysis [5,6].It is noted that in cases of traumatic brain injury, along with neuroprotectors, nootropic drugs should be used. Piracetam is used as the most effective means for this. In addition to the nootropic effect, piracetam also has antihypoxic, neuroprotective, antixiolytic, antidepressant and analgesic effects. Data on the nootropic activity of piracetam have been studied in detail. It has been studied in rodents using various methods (passive conditioned reflex (PCR), active conditioned reflex (ACR) and maze methods). They have been confirmed by many years of clinical practice. It is noted that the drug has an effective effect with long-term use in high doses. However, the positive effect of the drug occurs when taking courses of treatment in small doses [3].Disability in BMS is associated with primary brain damage and the formation of dysregulation mechanisms and a decrease in adaptive reserves over a long period of time and during the consequences of new clinical syndromes. Therefore, effective neuroprotection requires the use of a complex combination of drugs that act on different links in the chain of pathophysiological processes that develop after traumatic brain injury. Among the evidence-based medical research materials, one of the drugs with proven high medical efficacy is Ceraxon. Its active ingredient, citicoline, is a precursor of phosphatidylcholine (lecithin), which is the main component of neuronal membranes [7,22].The bioavailability of citicoline for the body is close to 100%. This allows the drug to be administered orally and parenterally. The instructions for use of the drug indicate the following indications for use: acute cerebral edema after acute brain injury and intracranial hypertension in patients with acute stroke. This indicates the absence of side effects in the clinical use of the drug. According to the results of the authors' research, citicoline has shown a number of positive results in hemorrhagic stroke, traumatic brain injury of varying degrees, and in elderly patients with cognitive disorders of vascular and neurodegenerative genesis [8,9].In experimental studies of local ischemia in rats, the following were found when using long-term citicoline as a therapeutic therapy. It was found that this drug promotes functional recovery of neurons and increases the plasticity of neurons at the border of uninjured brain matter. The analysis of the results of using citicoline in patients with brain injury made it possible to develop an optimal dose selection taking into account the severity of the disease [8]: in mild cases - in the first stage, 500-1000 mg intravenously per day for 5-6 weeks, in the second stage, 600-900 mg orally per day for 3-5 days; in moderate cases - in the first stage, 1500-2000 mg intravenously per day drip for 5-7 days, in the second stage, 900-1200 mg orally per day for 1.5-2 months; in severe head injury - in the first stage, from the day of injury, it is administered intravenously at a dose of 2000 mg/day for 10-14 days, then in the second stage, it is recommended to administer orally (through a gastric tube) at a dose of 1200-2000 mg/day for 2-3 months. Taking into account the proven safety and efficacy of the drug, it is confirmed that citicoline is a reliable drug that should be included in the list of neuroprotective drugs at the first signs of brain injury. The availability of oral and parenteral forms of citicoline makes it convenient for use in all categories of outpatients and inpatients [10,11,12,21].Severe traumatic brain injuries can lead to disability and, in some cases, death. 10-15% of deaths occur as a primary complication, while the remaining percentage is due to complications associated with secondary brain damage. In developed countries, injuries are the second leading cause of death after cardiovascular and oncological diseases, and in terms of total economic and socio-economic damage (temporary disability, disability and death), traumatic brain injury is the leading cause of death in a number of countries, as it is more common in young and middle-aged people. Although 0.2% of the total number of injured patients die, this figure increases with the severity of the injury. 90% of victims are admitted with mild TBI, and mortality is almost non-existent. The mortality rate in patients with moderate BMJ is from 5% to 20%, and the mortality rate in severe BMJ (this diagnosis is made by less than 10% of victims), according to different authors, reaches 38-80% [10,13,14].In conclusion, the thymus plays an important role in the development and functioning of the immune system, especially in the early stages of human life. Its condition and response to brain injury can significantly affect the recovery processes and the general condition of the body [8,13,16]. The results of the analysis of the scientific literature show that the morphometric, morphofunctional and immunohistochemical changes in the thymus in different degrees of brain injury, i.e. mild, moderate and severe, have not been sufficiently identified. There is also practically no scientifically substantiated data on modeling brain injury in laboratory animals. This situation requires a detailed study of the morphometric parameters of thymic tissue and the changes that may occur in the thymus in brain injury [14]. Following neuroprotective correction of brain injuries, the thymus exhibited near-normal shape, coloration, and capsule luster. That is, for pharmacological correction, L-lysine aescinate (1 mg/mL) was administered intramuscularly at a dose of 5 mL, and citicoline (125 mg/mL) was administered intramuscularly at a dose of 4 mL for 10 consecutive days. A comparative analysis of morphometric parameters was conducted between animal groups with brain injury and control groups using the "road accident" model. The obtained results were statistically analyzed and described. The findings of the study were documented in a formal report. The following results were obtained when studying the organometric indices of the thymus in 3-month-old white rats after correction of brain injuries with neuroprotectors [18,19,20].
2. Materials and Methods
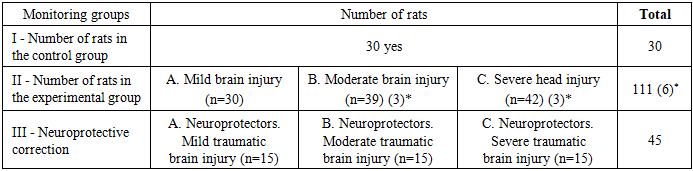
- The dissertation work was carried out in the research laboratory of the Abu Ali Ibn Sino Bukhara State Medical Institute from 2022 to 2024. Based on the results of the morphometric study of thymus parameters under the influence of traumatic brain injury, an algorithm for providing emergency care to patients with traumatic brain injury is developed, taking into account the periods of emergency situations. A method for calculating the prognosis of the condition of patients with traumatic brain injury, taking into account the periods of traumatic brain injury, is determined. When working with laboratory animals, all biological safety rules and ethical principles for working with laboratory animals given in the methodological manual by Nuraliev N.A., Bektimirova A.M., Alimova M.T., Suvanov K.J. were followed. “Rules and methods of working with laboratory animals in microbiological and immunological research”, approved by the resolution of the Ministry of Health of the Republic of Uzbekistan dated May 25, 2016 (8n-p89), and the information letter of Nuraliev N.A., Suvonov K.J., Khamrakulova M.A. “Ethical principles of working with laboratory animals”, registered by the ONMI of the Ministry of Health of the Republic of Uzbekistan on June 6, 2016 (№0438).For the purpose of experimental studies, 186 three-month-old white non-breed rats of both sexes, kept in ordinary vivarium conditions, were used. All laboratory animals were kept in plastic cages with wood shavings in the vivarium, at standard room temperature, with a 12-hour light-dark cycle, in accordance with the standards for keeping laboratory animals. All rats were kept in quarantine for one week, after which all animals were visually inspected to ensure that there were no somatic or infectious diseases. After ruling out any disease-specific pathology in the rats, they were transferred to their usual vivarium conditions.The following groups were formed to determine the morphological and morphometric indicators of the thymus structure at different levels of severity of brain injury.
|
3. Results
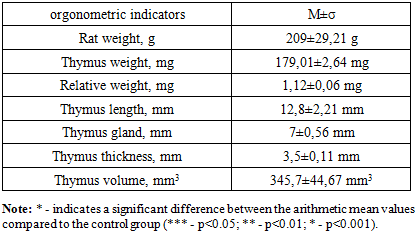
- According to the morphometric analysis after neuroprotective correction of traumatic brain injury in 3-month-old white outbred rats, the body weight ranged from 179.79 g to 238.21 g, with a mean of 209 ± 29.21 g. The mean thymus weight was 179.01 ± 2.64 mg, relative weight — 1.12 ± 0.06 mg, length — 12.8 ± 2.21 mm, width — 7 ± 0.56 mm, thickness — 3.5 ± 0.11 mm, and thymus volume — 345.7 ± 44.67 mm³. These values were obtained based on the morphometric analysis results.
|
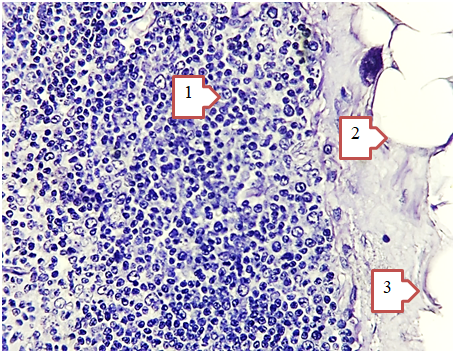 | Figure 1. Morphological changes in the thymus after treatment of traumatic brain injury with neuroprotectors. Hematoxylin-eosin staining; magnification ×400. The thymus tissue shows: (1) adipocytes, (2) a cortical layer of lymphoid cells (thymocytes), and (3) a collagenous connective tissue barrier |
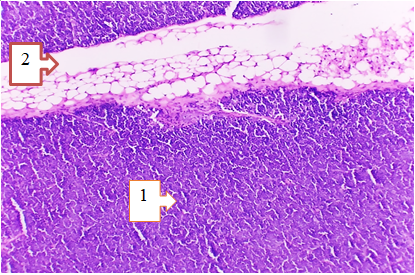 | Figure 2. Morphological changes in the thymus after treatment of traumatic brain injury with neuroprotectors. Hematoxylin-eosin staining; magnification ×400. Thymic epithelial cells (1) and areas of fatty metamorphosis (2) are visible |
|
4. Discussion
- The results of our study indicate that neuroprotective correction after traumatic brain injury (TBI) contributes to the restoration of thymic structure and function. Morphological observations showed that after the administration of neuroprotective agents, the general shape, color, and capsule brightness of the thymus approached normal. This finding suggests improvement in the organ’s trophic state and blood circulation.The use of L-lysine aescinate and citicoline had a significant effect on the recovery processes in experimental animals. These drugs possess anti-exudative, antioxidant, and neuroregenerative properties that reduce cellular hypoxia and improve metabolic activity in nervous tissue. As a result, the stress response associated with brain injury was alleviated, and gradual normalization of thymic morphology was observed.Morphometric data revealed an increase in thymus mass and volume compared to the untreated TBI group, indicating activation of thymic function and partial restoration of immune activity. The increase in relative thymus weight and its structural parameters (length, width, and thickness) reflects enhanced proliferative activity and a reduction in atrophic changes. These findings are consistent with previous data showing a close relationship between the integrity of the central nervous system and the condition of immune organs.Furthermore, the positive changes observed in the general state and behavior of animals after neuroprotective therapy confirm the overall systemic effect of the applied treatment method. Stabilization of body weight and normalization of behavioral responses demonstrate that neuroprotective correction not only alleviates the severity of brain injury but also reduces secondary immunological disturbances.In general, the combined use of L-lysine aescinate and citicoline exhibits a clearly defined neuroprotective and immunomodulatory effect, contributing to the recovery of both neural and thymic structures after traumatic brain injury.
5. Conclusions
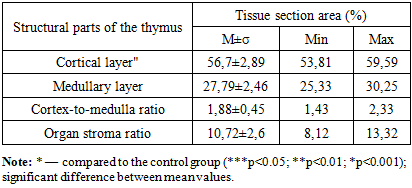
- Following neuroprotective therapy, a significant recovery of the morphological and morphometric parameters of the thymus was observed. In particular, in treated animals compared to the severe BMD group, thymus weight increased by 38.2% and volume by 41.3% (p < 0.05). The proportion of the cortex increased to 56.7 ± 2.89%, the medulla to 27.79 ± 2.46%, and the cortex-to-medulla ratio was restored to 1.88 ± 0.45. The proportion of stromal tissue decreased to 10.72 ± 2.6%, indicating a reduction in fibrillar components and collagen.Histological analysis revealed normalization in the shape and localization of Hassall's corpuscles, increased lymphoid cell density, reduced capillary permeability, maintenance of mucopolysaccharide levels within the normal range, and elimination of hypersecretion. These findings suggest that neuroprotective therapy effectively reduces stress-induced thymic involution and promotes the restoration of immune architecture.Proliferation of thymocytes and a reduction in the rate of fatty metamorphosis were observed. Focal proliferation of T-lymphocytes was noted in the subcapsular region of the cortex, along with the formation of immature prethymocytes actively dividing by mitosis. Enlargement of the nuclei in thymic epithelial (reticuloepithelial) cells—also undergoing mitotic division—further indicated active cellular regeneration.Additionally, a reduction in stromal edema was observed. These findings suggest a partial reversal of degeneration in the reticuloepithelial cells and restoration of both T-lymphocyte and epithelial cell function. Such regenerative processes support the production of biologically active substances and reflect the thymus's role in the endocrine regulation of the body.