-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4184-4188
doi:10.5923/j.ajmms.20251511.95
Received: Sep. 6, 2025; Accepted: Oct. 3, 2025; Published: Nov. 28, 2025

Cognitive Dysfunction and Emotional-Behavioral Disorders in Patients with Ischemic Stroke: Correlation with Neurological Status and Quality of Life
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuradimova Alfiya Rashidovna1, Gulomqodirov Muzaffar Maxmit ugli2
1PhD, Associate Professor, Head of the Department of Neurology and Psychiatry, Fergana Medical Institute of Public Health, Uzbekistan
2Assistant, Department of Neurology and Psychiatry, Fergana Medical Institute of Public Health, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study presents the results of analyzing cognitive, emotional, and behavioral disorders in 75 patients during the early recovery period of ischemic stroke. Depending on the localization of the lesion, patients were divided into two groups: cortical and subcortical strokes. Cognitive functions were assessed using a modified MoCA scale with additional subtests designed to detect specific deficits associated with right hemisphere lesions (right–left orientation, simultanagnosia, prosopagnosia, ideational apraxia, and metaphor comprehension). The emotional sphere was evaluated using the Hospital Anxiety and Depression Scale (HADS) and the Starkstein Apathy Scale (SAS). Quality of life was assessed with the Stroke-Specific Quality of Life Scale (SS-QOL). The findings revealed that cortical strokes were more often associated with pronounced cognitive deficits and anxiety-depressive disorders, while subcortical strokes were characterized by apathetic-abulic manifestations and reduced motivation. These results highlight the pathogenetic role of stroke localization in the development of cognitive-emotional impairments and emphasize the importance of developing differentiated neurorehabilitation programs.
Keywords: Ischemic stroke, Early recovery period, Cortical stroke, Subcortical stroke, Cognitive impairment, Modified MoCA scale, Depression, Anxiety, Apathy, Quality of life
Cite this paper: Muradimova Alfiya Rashidovna, Gulomqodirov Muzaffar Maxmit ugli, Cognitive Dysfunction and Emotional-Behavioral Disorders in Patients with Ischemic Stroke: Correlation with Neurological Status and Quality of Life, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4184-4188. doi: 10.5923/j.ajmms.20251511.95.
1. Introduction
- Stroke is one of the key medical and social challenges for healthcare worldwide. According to the World Health Organization, stroke ranks second among the leading causes of mortality, accounting for about 10% of all deaths [1,2].In Uzbekistan, stroke remains one of the primary causes of death and disability. According to the Ministry of Health of the Republic of Uzbekistan and WHO, more than 40–45 thousand new cases of stroke are registered annually, with approximately 70% being ischemic forms. Stroke mortality rates in the country range from 18–20%, and more than half of survivors are left with persistent disability. Stroke accounts for over 40% of all disability cases, which highlights the high social significance of the problem [1].The issue of early rehabilitation of patients after acute cerebrovascular accident (ACVA) is particularly important, as a significant proportion of them lose their working capacity [4]. Motor impairments caused by disruptions in motor activity regulation remain the leading factor of long-term disability [5]. Equally important are cognitive and emotional disorders, which may represent the dominant clinical manifestation of stroke and significantly influence prognosis, quality of life, and recovery potential [6,7].The study of etiological factors, pathogenetic mechanisms, and molecular biomarkers of stroke, along with the development of modern methods for early diagnosis and correction of neuropsychological impairments, is of particular importance, since these processes directly determine rehabilitation outcomes, life expectancy, and quality of life in patients who have suffered acute cerebrovascular accidents [5–8,16,17]. Neuropsychological disorders often serve as the only clinical manifestation of stroke or occupy a central role in its symptomatology. An important milestone in neuropsychology was the introduction of the concept of the “neuropsychological factor”, which enabled the identification and explanation of the interrelation between cognitive, emotional, and behavioral changes in patients with lesions of different areas of the right and left hemispheres [3–10].Currently, functional asymmetry and interhemispheric interaction of the brain are considered among the most promising directions in clinical neurology of stroke [9,10]. The recognition of ontogenetic patterns of higher mental functions, their systemic organization, and topographic specificity has become the foundation for further research on interhemispheric differences [11].Over the past decades, extensive data on functional lateralization have been accumulated in global and domestic science; however, in clinical practice, individual asymmetry features are often insufficiently taken into account, which may affect stroke progression, disease outcomes, and processes of social adaptation [12,13]. Of particular clinical importance are neuropsychological syndromes that occur in focal lesions of the right or left hemisphere during the acute phase of stroke, as they may represent the leading or even the sole manifestation of pathology [14,15].Comparative studies demonstrate pronounced differences in emotional-volitional, motivational, and cognitive-behavioral domains in patients with right- versus left-hemispheric lesions. In particular, individuals with right hemisphere damage more frequently experience impairments of attention, perception, learning, as well as difficulties in recognizing and expressing emotions [16]. They are characterized by a low level of awareness of their condition, reduced emotional responses, manifestations of anosognosia and neglect syndrome, as well as difficulties in performing complex language tasks involving semantic and lexical processing.A particularly urgent issue remains the delayed seeking of medical care and insufficient access to modern methods of neurorehabilitation, including cognitive-behavioral correction and the use of innovative neuromodulation technologies.Objective of the StudyThe aim of the study was to assess the severity of cognitive and psycho-emotional disorders in patients during the early recovery period of ischemic stroke.
2. Materials and Methods
- The study was conducted at the Neurology Department of the Multidisciplinary Clinic of the Fergana Medical Institute of Public Health between January 2024 and January 2025. A total of 75 patients diagnosed with ischemic stroke in the early recovery period were included.Depending on the lesion site, patients were divided into two groups:Group 1 — 37 patients with cortical stroke (15 men — 40.5% and 22 women — 59.5%); mean age: 61.3 ± 12.7 years.Group 2 — 38 patients with subcortical stroke (21 men — 55.3% and 17 women — 44.7%); mean age: 63.1 ± 11.5 years (figure 1).
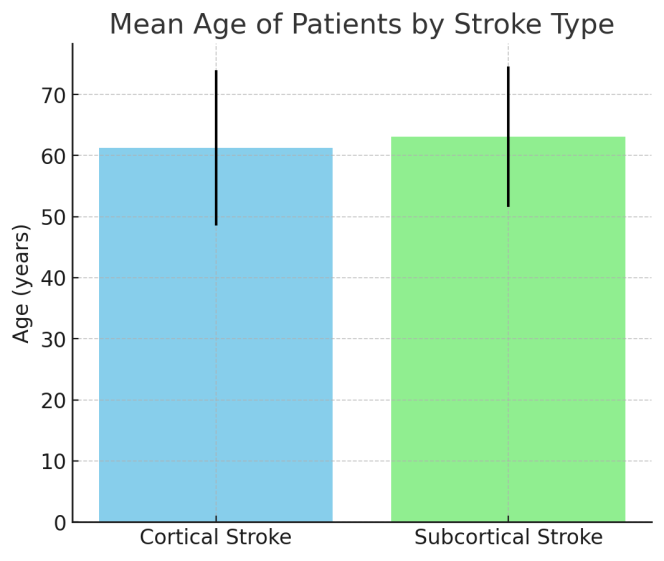 | Figure 1. Age characteristics of the studied patients |
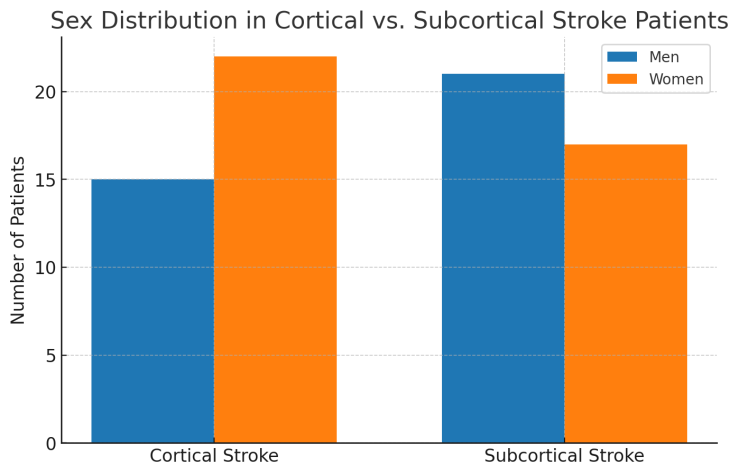 | Figure 2. Gender characteristics of the studied patients |
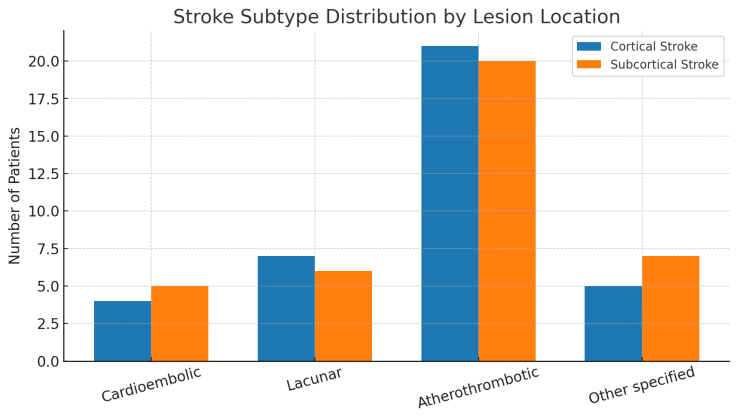 | Figure 3. Types of ischemic stroke causes according to TOAST |
3. Results and Discussion
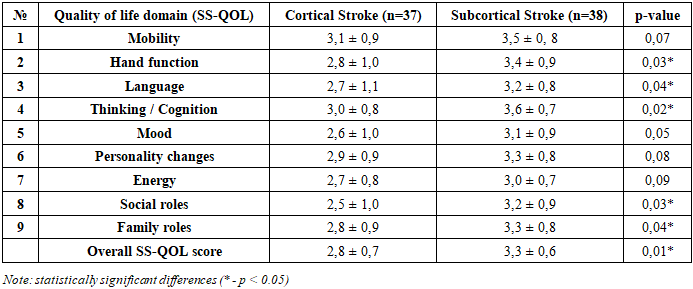
- Before conducting the study, an assessment of the somatic and neurological status of the patients was performed. All patients demonstrated stable hemodynamics. Neurological disorders were evaluated using the National Institutes of Health Stroke Scale (NIHSS). Upon hospital admission, patients in Group 1 had a median NIHSS score of 6.0 [3.7; 9.2], while patients in Group 2 had a median score of 5.0 [5.7; 9.0]. By day 7 of the disease, the neurological deficit in both groups was reduced to 3.0 [1.7; 5.0].Cognitive status was assessed using the modified Montreal Cognitive Assessment (MoCA), which enabled a detailed analysis of both global cognitive decline and specific deficits associated with right hemisphere damage. The standard MoCA protocol was expanded with additional subscales to verify the following impairments: right–left disorientation, simultanagnosia, prosopagnosia, ideational apraxia, and difficulties in understanding metaphors.In patients with cortical brain lesions (Group 1, n=37), cognitive impairments were more diverse and pronounced. The mean MoCA score was 22.1 ± 3.4, indicating moderate cognitive impairment. The main deficit domains included: attention and concentration – impaired in 64.9% of patients, manifesting as difficulties in retaining information and shifting attention; short-term memory – reduced in 70.3%, with difficulties in word recall after a brief delay; language – deficits in naming and verbal fluency were present in 59.5%; visuospatial functions – impaired in 56.7%, with difficulties in the clock-drawing test and figure copying.Additional findings from the modified MoCA: right–left disorientation – 29.7%; simultanagnosia (difficulty perceiving whole images) – 24.3%; prosopagnosia (impaired face recognition) – 18.9%; ideational apraxia (difficulty performing sequential actions) – 27.0%; impaired metaphor comprehension – 32.4%.In patients with subcortical strokes (Group 2, n=38), cognitive impairments were less pronounced but more specific. The mean MoCA score was 23.8 ± 3.1, closer to normal but still indicating mild cognitive impairment. The main deficit domains included: processing speed and attention – impaired in 52.6%, with reduced concentration and slowed mental shifting; executive functions (sequencing, planning) – impaired in 47.3%; working memory – impaired in 44.7%, with difficulties retaining and manipulating information; visuospatial functions – reduced in 34.2%, though less severe than in the cortical group.Additional findings from the modified MoCA: simultanagnosia – 10.5%; prosopagnosia – 7.9%; ideational apraxia – 13.2%; difficulties in metaphor comprehension – 15.8%; right–left disorientation – rare (5.3%).Comparative analysis demonstrated that cortical strokes are associated with more severe cognitive deficits (MoCA < 26 in 81.1% of patients), particularly affecting language, associative, and visuospatial domains, while subcortical strokes were associated with milder impairments (MoCA < 26 in 65.8%), primarily affecting attention, executive functions, and processing speed. In the modified MoCA, cortical deficits (agnosias, apraxias, metaphor comprehension difficulties) occurred significantly more often in cortical stroke patients (p < 0.05).Emotional status was assessed during the early recovery phase of ischemic stroke using the HADS and the Starkstein Apathy Scale. Analysis with the HADS revealed that patients with cortical stroke more frequently experienced pronounced anxiety-depressive disorders, whereas patients with subcortical stroke demonstrated less severe anxiety but persistent emotional lability (Table 1).
|

|

|
4. Conclusions
- The study demonstrated that cognitive, psycho-emotional, and behavioral disorders in the early recovery period of ischemic stroke have distinct neuropathogenetic features determined by the localization of the lesion.In patients with cortical stroke, more pronounced cognitive deficits were observed, which can be explained by damage to the associative brain regions involved in the organization of speech, memory, visuospatial, and executive functions. The modified MoCA scale revealed a high frequency of agnosias, apraxias, and difficulties in understanding metaphors, indicating disintegration of cortical networks responsible for complex cognitive operations. Emotional disturbances in this group were mainly represented by anxiety-depressive disorders, reflecting the pathogenetic link between frontal-limbic damage and dysfunction of emotion regulation systems.In patients with subcortical stroke, cognitive deficits were less severe, but disturbances in attention, processing speed, and executive functions predominated. These changes can be explained by the involvement of subcortical-frontal connections and disruption of the fronto-striato-thalamic circuits. In the emotional sphere, apathy and reduced motivation were more frequently observed, reflecting dysfunction of dopaminergic and medial frontal structures.A decline in quality of life was found in both groups, but with different pathogenetic profiles: in cortical strokes, impairments of language functions, mood, and social roles predominated, whereas in subcortical strokes, the main factors reducing quality of life were apathy and low energy, with relatively preserved language and cognitive functions.Thus, the pathogenesis of cognitive and psycho-emotional disorders in the early recovery period of ischemic stroke is determined by lesion localization: cortical strokes are associated with more severe cognitive deficits, anxiety-depressive disorders, and pronounced socio-communicative impairments; subcortical strokes are characterized by apatho-abulic manifestations and executive dysfunction, with less prominent speech and spatial deficits.These findings confirm the necessity of a comprehensive approach to the diagnosis and rehabilitation of stroke patients, which should include not only the assessment of cognitive and neurological deficits but also analysis of the emotional-motivational sphere and quality of life. This allows the development of individualized rehabilitation programs.