-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4173-4176
doi:10.5923/j.ajmms.20251511.93
Received: Sep. 21, 2025; Accepted: Oct. 16, 2025; Published: Nov. 27, 2025

Results of 6-Month Use of Neprilysin Inhibitors in Chronic Heart Failure
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKodirova Sh. K.1, Kenzhaev M. L.2
1First-year PhD Student (Basic Doctoral Program), Republican Specialized Scientific and Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan
2Chief Physician of the Tashkent Regional Specialized Somatic Hospital, Doctor of Medical Sciences, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic heart failure (CHF) with reduced ejection fraction remains a major cause of morbidity and mortality. This study evaluated the effects of 6-month therapy with the neprilysin inhibitor sacubitril/valsartan in 58 patients with NYHA class II–IV CHF and LVEF <40%. Treatment led to a significant improvement in systolic function (LVEF increased from 40% to 49%) and reduction of ventricular volumes, indicating reverse remodeling. Diastolic function markers improved, and NT-proBNP levels decreased by more than 2.5-fold, reflecting reduced neurohormonal activation. Clinically, 69% of patients improved by at least one NYHA class, and CHF-related hospitalizations decreased by 52%. These findings confirm the medium-term effectiveness of sacubitril/valsartan in improving cardiac function and clinical outcomes in patients with HFrEF.
Keywords: Chronic heart failure (CHF), Neprilysin inhibitors, Sacubitril/valsartan, NT-proBNP, Echocardiography, Reverse remodeling
Cite this paper: Kodirova Sh. K., Kenzhaev M. L., Results of 6-Month Use of Neprilysin Inhibitors in Chronic Heart Failure, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4173-4176. doi: 10.5923/j.ajmms.20251511.93.
1. Introduction
- CHF remains one of the leading causes of disability and mortality among the adult population. Impaired neurohormonal regulation, particularly the activation of the renin–angiotensin–aldosterone system (RAAS) and the sympathoadrenal system, plays a key role in the pathogenesis of CHF [6]. The emergence of neprilysin inhibitors, represented by the combined drug sacubitril/valsartan, has opened new opportunities in the treatment of CHF with reduced ejection fraction [1]. The mechanism of action of sacubitril/valsartan involves simultaneous inhibition of neprilysin and blockade of angiotensin II receptors, which leads to improved hemodynamics, reduction of natriuretic peptide levels, and a favorable impact on myocardial remodeling [3]. Objective: To assess the impact of neprilysin inhibitors (sacubitril/valsartan) on the clinical and functional status of patients with chronic heart failure (CHF) with reduced ejection fraction.
2. Materials and Methods
- The study included 58 patients (mean age: 63 ± 8 years; 67% men) with CHF class II–IV according to NYHA and LVEF <40%. All participants provided informed consent to take part in the study.Exclusion criteria: acute coronary syndrome or revascularization within the past 3 months; severe chronic kidney disease (eGFR <30 mL/min/1.73 m²); significant hepatic dysfunction; uncontrolled arterial hypertension (BP >180/110 mmHg); acute inflammatory diseases and active malignant neoplasms; allergy or intolerance to drug components; and poor treatment adherence.All participants received UPERIO (sacubitril/valsartan, Novartis Pharma Services AG, Russia) in titrated doses (initial dose 50–100 mg twice daily, further increased to 200 mg twice daily) as part of standard CHF therapy. Treatment effectiveness was evaluated based on changes in echocardiographic parameters (LVEF, EDV, ESV), hospitalization rates, and NYHA functional class, as well as quality of life assessment (MLHFQ) and measurement of NT-proBNP levels using FINECARE test systems on the Wondfo FINECARE analyzer. Assessments were performed at baseline and after 3 and 6 months of pharmacotherapy.Statistical analysis:Statistical analysis was performed using Jamovi software (version 2.2.5.0). To assess the dynamics of quantitative variables, the paired t-test was used for normally distributed data, or the Wilcoxon signed-rank test for non-normally distributed data. For multiple comparisons, repeated-measures analysis of variance (ANOVA) was applied. Categorical variables were analyzed using the χ² test. Statistical significance was defined as p<0.05.
3. Results
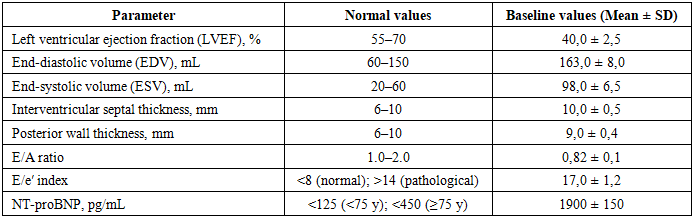
- Chronic heart failure (CHF) is one of the most common and socially significant cardiovascular diseases, characterized by a progressive decline in myocardial contractile function and impairment of systemic hemodynamics. Clinical and functional parameters play a leading role in the assessment of patients with CHF, as they reflect the degree of cardiac pump dysfunction, exercise tolerance, and disease prognosis [5]. A comprehensive evaluation of these parameters makes it possible to timely detect the progression of the pathological process, optimize therapy, and assess the effectiveness of the treatment provided [2].For an objective assessment of the obtained echocardiographic parameters and NT-proBNP levels, the study results were compared with reference values presented in current international guidelines [7,4].Results (continued)The normal left ventricular ejection fraction (LVEF) ranges from 55% to 70% and serves as the main criterion for preserved myocardial contractile function. End-diastolic volume (EDV) and end-systolic volume (ESV) reflect the geometric characteristics of the left ventricular cavity and allow assessment of the presence or absence of dilation. Interventricular septal thickness and posterior wall thickness of the left ventricle within 6–10 mm correspond to a normal myocardial profile without signs of hypertrophy.Indicators of diastolic function include the E/A ratio (normal range 1.0–2.0) and the E/e′ index, with values <8 indicating normal filling pressure, and values >14 suggesting pathological elevation of filling pressure. NT-proBNP concentrations below 125 pg/mL in individuals under 75 years of age and below 450 pg/mL in older patients are considered normal and reflect the absence of significant neurohormonal activation.In accordance with the aim of our study, we evaluated the clinical and functional cardiac parameters in patients with CHF prior to pharmacotherapy with neprilysin inhibitors (Table 1), which demonstrated that …
|
|
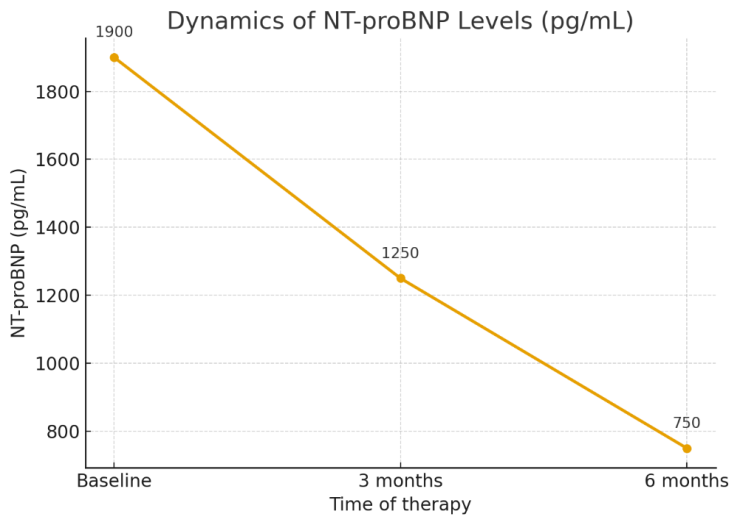 | Figure 1. NT-proBNP levels in patients after pharmacotherapy |
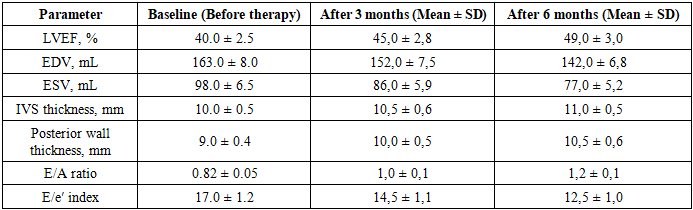
4. Conclusions
- The use of neprilysin inhibitors as part of combination therapy for CHF contributes to a significant improvement in clinical status, left ventricular remodeling, and reduced frequency of decompensations, confirming the high effectiveness of this approach in the medium term.After 6 months of therapy, positive dynamics were recorded in 87% of patients:• Mean reduction of NT-proBNP by 38%• Improvement of CHF functional class by ≥1 stage in 69%• Reduction of hospitalizations due to CHF decompensation by 52%• Improvement of subjective quality of life (average reduction of MLHFQ score by 15 points)In 13% of patients, the therapeutic effect was minimal; this group was predominantly represented by individuals with type 2 diabetes mellitus, anemia, and poor treatment adherence.