-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4147-4149
doi:10.5923/j.ajmms.20251511.87
Received: Oct. 10, 2025; Accepted: Nov. 3, 2025; Published: Nov. 25, 2025

Clinical and Microbiological Features of Generalized Periodontitis in Patients After Kidney Transplantation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRizaev E. O.1, Mirzaev Kh. Sh.2
1Faculty Therapeutic Dentistry Department, Tashkent State Medical University, Tashkent, Uzbekistan
2Therapeutic Dentistry Propaedeutics Department, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Periodontitis is a chronic inflammatory disease of the oral cavity that progressively destroys the tooth-supporting structures. In patients with chronic kidney disease (CKD), particularly those after kidney transplantation, periodontal disease often presents in more severe forms due to systemic comorbidities, impaired microcirculation, and compromised immune response. The present study aimed to improve the effectiveness of diagnosis and treatment of generalized periodontitis in kidney transplant recipients. A total of 105 patients aged 20–60 years were examined, including 54 kidney transplant recipients with generalized periodontitis (main group), 30 patients with generalized periodontitis without renal pathology (comparison group), and 20 healthy controls. Clinical and microbiological methods were applied. Results demonstrated more severe periodontal manifestations in kidney transplant recipients compared with controls, including higher bleeding indices, probing pocket depth, and tooth mobility. Oral microbiota analysis revealed marked dysbiosis with increased facultative microorganisms (Staphylococcus spp., Streptococcus spp., Candida spp.) in both groups, but less pronounced in transplant patients compared to those with generalized periodontitis without renal pathology. It was established that comorbidity and polymorbidity distort the clinical course of periodontitis, contribute to more severe progression, and increase the risk of complications. Tailored diagnostic and therapeutic protocols are therefore essential for kidney transplant patients.
Keywords: Periodontitis, Kidney transplantation, Chronic kidney disease, Oral microbiota, Comorbidity
Cite this paper: Rizaev E. O., Mirzaev Kh. Sh., Clinical and Microbiological Features of Generalized Periodontitis in Patients After Kidney Transplantation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4147-4149. doi: 10.5923/j.ajmms.20251511.87.
Article Outline
1. Introduction
- Periodontitis is a chronic inflammatory disease of the oral cavity that progressively destroys the periodontal tissues and leads to tooth mobility and loss. It usually develops as a complication of gingivitis and represents a major dental and systemic health problem. According to various studies, periodontal diseases affect up to 98% of the adult population and show an increasing prevalence [1,2,7,8].Patients with chronic kidney disease (CKD), especially those who have undergone kidney transplantation, exhibit a higher frequency of severe generalized periodontitis (Community Periodontal Index 3.43–3.52). These patients often demonstrate poor oral hygiene (Silness-Löe index 2.44–3.56) and high rates of oral mucosal diseases (16.3–39.0%) [2,3,4,5]. Thus, the development of targeted diagnostic and treatment strategies for this population is of great clinical significance.
2. Object of Research
- The study included 105 patients aged 20-60 years, 54 of whom had chronic generalized periodontitis and had undergone kidney transplants. The main group included 28 women and 22 men; 30 patients with chronic generalized periodontitis who had undergone kidney transplants, including 18 women and 12 men, formed the comparison group; 20 healthy individuals served as a control.
3. Material and Methods of Research
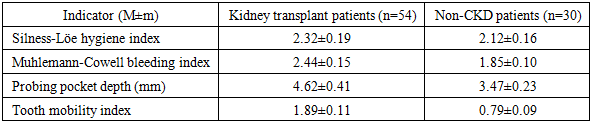
- Clinical examination included assessment of gingival bleeding (Muhlemann-Cowell index), oral hygiene (Silness-Löe index), probing pocket depth (PPD), and tooth mobility (Miller-Fleszar index). Radiographic studies were performed. Microbiological analysis of oral fluid was conducted to evaluate aerobic and anaerobic flora. Statistical analysis was performed using standard methods with p<0.05 considered significant.The comparison groups were randomized by sex, age and frequency of underlying somatic pathology, which ensured the representativeness of the data obtained during treatment.
4. The Results of the Study
- Clinical manifestations of periodontitis varied according to disease severity.- Healthy controls: No complaints, normal gingiva, no bleeding, no periodontal pockets.- Mild periodontitis: Gingival hyperemia, bleeding on brushing, pockets ≤3 mm, tooth mobility grade I, radiographic bone loss up to one-third of root length.- Moderate periodontitis: Gingival edema, cyanosis, suppuration, pockets ≤5 mm, tooth mobility grades I–II, radiographic bone loss up to half the root length.- Severe periodontitis: Persistent gingival pain, suppuration, halitosis, tooth mobility II–III, deep pockets (>5 mm), marked granulation and fibrosis.
|
5. Conclusions
- It has been established that somatic and periodontal pathologies are typically combined with other diseases, which corresponds to the status of polymorbidity. Furthermore, polymorbidity has been shown to distort the classic clinical picture of diseases, leading to a more severe course, increasing the risk of complications, reducing the effectiveness of treatment, and worsening life prognosis.Dysbiotic changes also occur in patients with chronic generalized periodontitis after kidney transplantation, but their severity is significantly lower than in patients without kidney disease. Although the number of all types of cocci is significantly increased in this group of patients, streptococci are predominant, while Candida species also show a similar trend.