-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4135-4141
doi:10.5923/j.ajmms.20251511.85
Received: Aug. 7, 2025; Accepted: Sep. 3, 2025; Published: Nov. 25, 2025

Comparative Analysis of Enamel Resistance and Caries Experience in Children Using Different Toothpastes
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShalola Iskandarovna Azizova1, Farangiz Abduvaitovna Abdurahimova2, Bakhtinur Oybutaevich Khudanov3
1PhD Candidate, Department of Preventive Dentistry, Tashkent State Dental Institute, Makhtumquli Street, Tashkent, Uzbekistan
2PhD, Senior Lecturer, Department of Preventive Dentistry, Tashkent State Dental Institute, Makhtumquli Street, Tashkent, Uzbekistan
3DSc, Professor, Department of Preventive Dentistry, Tashkent State Dental Institute, Makhtumquli Street, Tashkent, Uzbekistan
Correspondence to: Bakhtinur Oybutaevich Khudanov, DSc, Professor, Department of Preventive Dentistry, Tashkent State Dental Institute, Makhtumquli Street, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. Dental caries remains a significant public health concern, particularly among children, due to its impact on oral health and overall well-being. Purposes and tasks. This study aimed to evaluate the effectiveness of different toothpaste formulations in preventing caries progression and enhancing enamel resistance among 15-year-old children over a 12-month period. Materials and methods. A comparative analysis was conducted on five groups using fluoride-based, hydroxyapatite-based, and fluoride-free toothpastes. Caries experience was assessed using the Decayed, Missing, and Filled Teeth (DMFT) index, while enamel resistance was measured using the Test for Enamel Resistance (TER). Results. At baseline, DMFT scores showed no significant differences among groups (p > 0.05). After 12 months, fluoride toothpastes had the lowest DMFT increase, with Colgate Total 12 (5.15 ± 0.2) and Colgate Calcium-Remin (5.28 ± 0.14) significantly reducing caries progression (p < 0.05) compared to the fluoride-free control (5.91 ± 0.2). Hydroxyapatite-based toothpaste (Splat) provided moderate protection but was not significantly different from the control (p > 0.05). TER values declined in fluoride groups (Colgate Total 12: 3.51 ± 0.17, Colgate Calcium-Remin: 4.57 ± 0.18, p < 0.05), indicating increased acid susceptibility despite caries protection. Hydroxyapatite-based toothpaste maintained stable TER (5.4 ± 0.13, p > 0.05), preserving enamel resistance. The fluoride-free control (ROCS) showed an unexpected TER increase (5.62 ± 0.22), possibly due to methodological variability. Conclusion. Fluoride toothpastes reduce caries progression, while hydroxyapatite offers better enamel protection. Fluoride-free toothpaste showed minimal protection, emphasizing fluoride's role in pediatric oral care. Future research should explore fluoride-hydroxyapatite hybrids for optimal benefits.
Keywords: Dental caries, Fluoride toothpaste, Enamel resistance, DMFT index, Caries prevention, Remineralization
Cite this paper: Shalola Iskandarovna Azizova, Farangiz Abduvaitovna Abdurahimova, Bakhtinur Oybutaevich Khudanov, Comparative Analysis of Enamel Resistance and Caries Experience in Children Using Different Toothpastes, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4135-4141. doi: 10.5923/j.ajmms.20251511.85.
Article Outline
1. Introduction
- Dental caries is one of the most widespread chronic diseases affecting children and adolescents worldwide, posing significant challenges to public health. According to the World Health Organization (WHO), dental caries affects nearly 60–90% of school-aged children globally, with varying prevalence depending on socioeconomic status, dietary habits, and access to preventive dental care [1]. Caries is a multifactorial disease caused by the demineralization of enamel due to acidogenic bacterial activity in dental plaque, often exacerbated by poor oral hygiene and frequent consumption of fermentable carbohydrates [2].Fluoride has long been recognized as an essential agent in caries prevention due to its ability to enhance enamel remineralization, inhibit bacterial metabolism, and reduce enamel solubility in acidic environments [3]. Fluoride-containing toothpastes have been extensively studied and are considered the gold standard in caries prevention, with numerous studies demonstrating their efficacy in reducing caries incidence and progression [4]. However, concerns regarding fluoride overexposure, especially in children, have led to the development of alternative remineralizing agents such as hydroxyapatite (HA), a bioactive material that mimics the natural mineral composition of enamel and has shown potential in strengthening and repairing enamel lesions [5].Hydroxyapatite-based toothpastes have gained attention as a non-toxic, biomimetic alternative to fluoride, with studies suggesting their ability to form a protective layer over the enamel, fill surface defects, and enhance resistance to acidic challenges [6]. However, the comparative effectiveness of fluoride-based, hydroxyapatite-based, and fluoride-free toothpastes in preventing caries and maintaining enamel resistance remains a subject of ongoing research.This study aims to evaluate and compare the effects of different toothpaste formulations on enamel resistance and caries experience in 15-year-old children over a 12-month period. The study specifically focuses on two key parameters:Caries Experience (DMFT Index): The Decayed, Missing, and Filled Teeth (DMFT) index, originally proposed by Klein and Palmer (1939), serves as an epidemiological measure of dental caries experience and progression.Enamel Resistance (TER Test): The acid resistance of enamel was assessed using the Enamel Resistance Test (TER), developed by Okusko et al. (2011) [7], which measures the ability of enamel to withstand acid exposure over time.By analyzing these parameters, this study seeks to determine whether fluoride-based toothpastes remain the most effective option for caries prevention, or if hydroxyapatite-based formulations offer comparable protective benefits. Additionally, the study assesses whether fluoride-free toothpastes provide adequate enamel protection or if their use may be associated with increased caries risk. The findings of this research will contribute to the growing body of literature on caries prevention strategies and provide practical insights for pediatric dentistry.
2. Materials and Methods
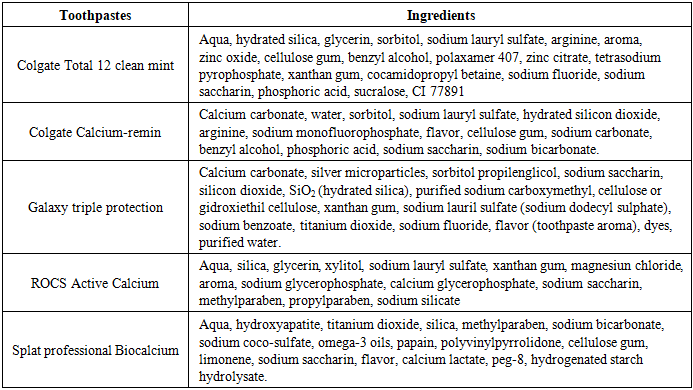
- Five experimental groups, each consisting of 50 children, were evaluated. The groups differed based on the type of toothpaste used:• Group 1: Colgate Total 12 clean mint (fluoride-based)• Group 2: Colgate Calcium-Remin (fluoride-based with calcium)• Group 3: Galaxy triple protection (fluoride-based, locally manufactured)• Group 4: Splat professional Biocalcium (hydroxyapatite-based)• Group 5: ROCS Active Calcium (Control Group) (fluoride-free)The specific contents of each toothpaste, such as active ingredients, flavoring agents, and other compounds relevant to their therapeutic claims, are detailed in Table 1 to provide a comparative overview of their composition.
|
|

3. Results
- Caries Experience Assessment (DMFT Index)At the beginning of the study, the mean DMFT values across the groups ranged between 4.31 and 4.88, with no significant differences among them (p > 0.05). Over time Fluoride-based groups (Colgate Total 12, Colgate Calcium-Remin, and Galaxy) exhibited lower increases in DMFT compared to the control group (p < 0.05).Hydroxyapatite-based toothpaste (Splat) showed moderate protective effects but was not significantly different from the control group (p > 0.05).Fluoride-free toothpaste (ROCS, control group) demonstrated the highest increase in DMFT, confirming its lower efficacy in preventing caries.The final results showed that the highest preventive effect was observed in Group 1 (Colgate Total 12) and Group 2 (Colgate Calcium-Remin), where the DMFT index remained significantly lower than in the control group. Group 3 (Galaxy) also showed statistically significant caries prevention, though slightly less effective than Groups 1 and 2. Meanwhile, Group 4 (Splat) exhibited moderate effectiveness, and Group 5 (ROCS, fluoride-free) had the highest increase in caries experience, indicating inadequate protection against caries progression (Figure 1).
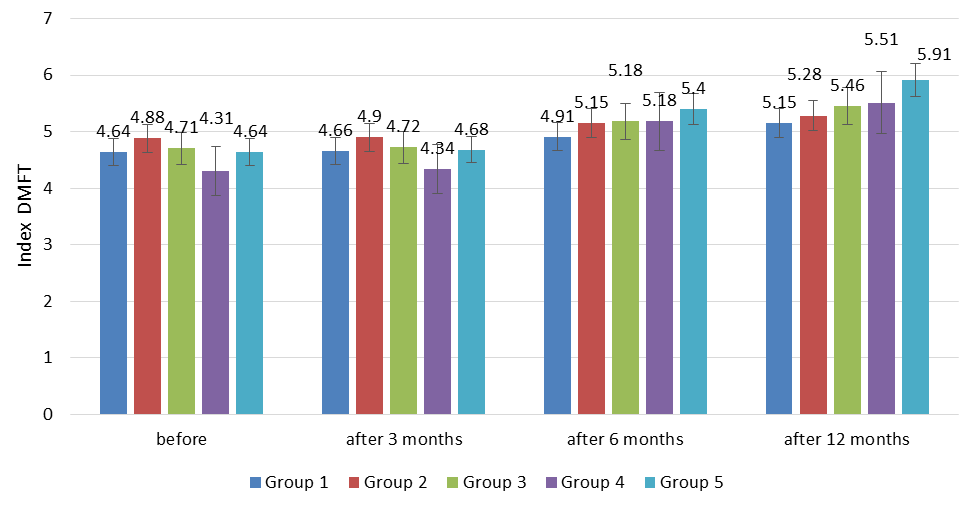 | Figure 1. Results of DMFT index evaluation |
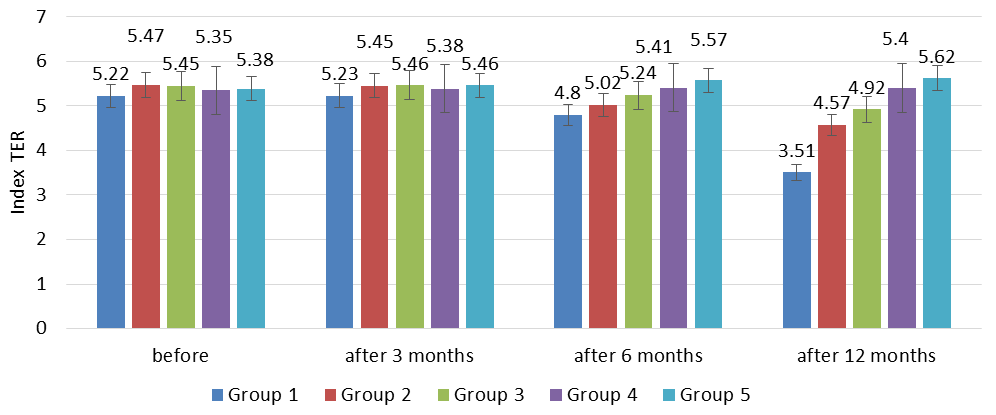 | Figure 2. Results of TER index evaluation |
4. Discussion
- The present study evaluated the efficacy of different toothpaste formulations in preventing dental caries and maintaining enamel resistance among children over a 12-month period [8]. The results demonstrated significant variations in the effectiveness of fluoride-based, hydroxyapatite-based, and fluoride-free toothpastes in terms of caries experience (DMFT index) and enamel resistance (TER test). The findings provide valuable insights into the role of different remineralization agents in caries prevention and enamel protection [9].The results of the DMFT index assessment clearly indicate that fluoride-containing toothpastes (Groups 1, 2, and 3) exhibited superior efficacy in reducing caries progression compared to non-fluoride formulations. The statistically significant lower increase in DMFT scores in these groups (p < 0.05) supports the well-established role of fluoride in caries prevention through the processes of remineralization and inhibition of bacterial metabolism [10-12].• Group 1 and Group 2 showed the lowest caries progression rates, confirming the importance of fluoride in conjunction with additional remineralizing agents like calcium and phosphates.• Group 3, a locally manufactured fluoride-based toothpaste, demonstrated moderate efficacy, though slightly lower than the leading international fluoride brands, suggesting that formulation differences might affect performance.• Group 4, a hydroxyapatite-based toothpaste, showed some protective effect, but was not significantly different from the control group (p > 0.05). This suggests that while hydroxyapatite has some potential for enamel remineralization, it may not be as effective in caries prevention as fluoride-based alternatives.• Group 5, the fluoride-free control group, exhibited the highest DMFT increase, confirming previous research that fluoride-free formulations provide insufficient protection against caries [13-15].The superiority of fluoride-based toothpastes in this study aligns with existing literature that supports fluoride's role in enhancing enamel resistance, reducing demineralization, and promoting the remineralization of early carious lesions [16]. However, differences among the fluoride formulations suggest that the addition of calcium and remineralizing agents may further enhance their protective effects.The TER test results provided additional insights into the long-term impact of different toothpaste formulations on enamel acid resistance.• Fluoride-based toothpastes (Groups 1, 2, and 3) exhibited a progressive decline in enamel resistance over time. This suggests that while fluoride enhances remineralization, it does not entirely prevent acid-induced demineralization.• The Group 1 showed the greatest decline in TER scores (3.51 ± 0.17 after 12 months, p < 0.05), followed by Colgate Calcium-Remin (4.57 ± 0.18, p < 0.05), and Galaxy (4.92 ± 0.19, p < 0.05). These results indicate that fluoride strengthens enamel primarily by promoting remineralization rather than by providing direct resistance to acid exposure.• Group 4, hydroxyapatite-based toothpaste showed the most stable enamel resistance levels (5.4 ± 0.13, p > 0.05), suggesting that hydroxyapatite may help preserve enamel integrity more effectively. Hydroxyapatite has been reported to fill microdefects in enamel, mimicking the natural mineral composition of teeth [17]. These findings align with previous studies demonstrating the potential of hydroxyapatite-based products in restoring enamel microstructure and improving resistance to acid attacks [18].• Unexpectedly, the fluoride-free control group, Group 5 demonstrated an increase in TER values over time (5.62 ± 0.22), which is inconsistent with previous research. This anomaly may be due to experimental variations or differences in sample behavior rather than a true improvement in enamel resistance.These findings suggest that while fluoride is essential for caries prevention, hydroxyapatite may provide additional benefits in maintaining enamel resistance. The combination of fluoride and hydroxyapatite might be a promising approach for future toothpaste formulations.The comparison of fluoride and hydroxyapatite in caries prevention and enamel protection provides valuable insights into their respective mechanisms and clinical effectiveness. Fluoride remains the gold standard in caries prevention, primarily due to its dual-action mechanism—enhancing remineralization and inhibiting bacterial metabolism. Fluoride promotes the deposition of calcium and phosphate ions, forming fluorapatite, a structure more resistant to acid dissolution than natural hydroxyapatite. In this study, fluoride-based toothpastes (Colgate Total 12, Colgate Calcium-Remin, and Galaxy) showed the lowest increase in DMFT scores over 12 months, confirming their superior ability to reduce caries incidence (p < 0.05). The statistically significant differences between the fluoride groups and the control group reinforce the well-documented benefits of fluoride in preventing demineralization and arresting early-stage carious lesions.However, despite fluoride’s effectiveness in reducing caries progression, enamel resistance (TER values) decreased over time in fluoride groups, suggesting that fluoride alone might not provide optimal long-term protection against acid erosion. The decline in enamel resistance (Colgate Total 12: 3.51 ± 0.17, p < 0.05; Colgate Calcium-Remin: 4.57 ± 0.18, p < 0.05) suggests that although fluoride aids in remineralization, it does not prevent ongoing enamel loss when exposed to acidic challenges. This highlights a potential limitation of fluoride, as it predominantly works in areas where active demineralization is already occurring, rather than acting as a structural reinforcer of enamel.On the other hand, hydroxyapatite-based toothpaste (Splat) showed a different pattern of protection, maintaining higher enamel resistance (TER: 5.4 ± 0.13, p > 0.05), even though its effectiveness in reducing DMFT scores was limited (p > 0.05, no significant difference from the control group). This suggests that hydroxyapatite does not actively prevent new carious lesions as effectively as fluoride but provides structural reinforcement to the enamel, reducing susceptibility to acid erosion. Unlike fluoride, which relies on ion exchange and chemical bonding, hydroxyapatite integrates directly into the enamel matrix, filling in microdefects and restoring mineral density without requiring biological activation. This supports previous findings that hydroxyapatite may be more effective in cases of enamel erosion and hypersensitivity rather than active caries prevention [19-21].A notable observation was the fluoride-free control group (ROCS) showing the highest increase in DMFT scores over 12 months (5.91 ± 0.2, p < 0.05 vs. fluoride groups), confirming its inadequacy in caries prevention. Interestingly, the TER values in the control group unexpectedly increased (5.62 ± 0.22, p > 0.05), which could be due to variations in salivary composition, diet, or measurement inconsistencies rather than true enamel strengthening. This highlights the complexity of enamel resistance as a multifactorial process, influenced not only by toothpaste composition but also by biological and environmental factors.These findings indicate that fluoride and hydroxyapatite function through complementary pathways. While fluoride remains the most effective agent in caries prevention, hydroxyapatite provides superior protection against enamel erosion. This raises an important question—should future toothpaste formulations incorporate both agents to achieve optimal oral health benefits? Several recent studies suggest that a fluoride-hydroxyapatite combination may provide synergistic effects, maximizing caries prevention while simultaneously reinforcing enamel integrity [22-26]. By combining fluoride’s antibacterial and remineralization properties with hydroxyapatite’s structural integration and protective film formation, a dual-action approach could potentially address both caries development and acid erosion more effectively.Clinical and Public Health ImplicationsThe study highlights several important clinical and public health implications:1. Fluoride remains the most effective agent for caries prevention and should be included in all pediatric oral care products.2. Hydroxyapatite-based toothpastes may be beneficial for individuals with enamel erosion, sensitivity, or high susceptibility to acid damage, but they should not replace fluoride in caries prevention strategies.3. Combination therapies using fluoride and hydroxyapatite could provide enhanced benefits by simultaneously reducing caries risk and strengthening enamel.4. Non-fluoride toothpastes (such as ROCS) offer insufficient protection against caries development and should not be recommended for children at high caries risk.Limitations of the StudyWhile the findings of this study provide valuable insights into the comparative efficacy of different toothpaste formulations, several limitations must be acknowledged:• The study was conducted over a 12-month period, which may not fully capture long-term effects on caries progression and enamel resistance.• Dietary habits, oral hygiene practices, and genetic factors were not controlled, which could have influenced caries development among participants.• The TER test relies on visual interpretation of color changes, which may introduce subjective bias, despite efforts to standardize assessments.Future research should focus on longer follow-up periods, controlled dietary assessments, and combined fluoride-hydroxyapatite formulations to better understand their synergistic potential.
5. Conclusions
- This study confirms that fluoride-based toothpastes remain the most effective method for caries prevention, as evidenced by significantly lower DMFT scores in fluoride-containing groups compared to fluoride-free alternatives. However, the TER test results suggest that hydroxyapatite-based toothpastes offer superior enamel resistance to acid exposure, potentially reducing erosion and mineral loss. These findings indicate that a dual-action approach combining fluoride's antimicrobial and remineralization properties with hydroxyapatite’s structural reinforcement may offer optimal oral health benefits. Future research should focus on developing and evaluating hybrid formulations that leverage both fluoride and hydroxyapatite for enhanced caries protection and enamel preservation.
CRediT Authorship Contribution Statement
- SA contributed to the methodology, conducted the investigation, curated the data, wrote the original draft, and participated in manuscript preparation. FA was involved in the conceptualization, methodology, original draft writing, and manuscript preparation. BK and SA both contributed to the conceptualization, methodology and participated in writing through review and editing. FA contributed to the conceptualization, methodology, conducted the investigation and participated in writing through review and editing. All authors collaboratively wrote and revised the manuscript and read and approved the final version.
Funding
- This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing Interests
- All the authors declare no conflict of interest.