-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4124-4131
doi:10.5923/j.ajmms.20251511.83
Received: Nov. 2, 2025; Accepted: Nov. 22, 2025; Published: Nov. 24, 2025

Principles of Rehabilitation of Psycho-Neurological Changes in Autistic Spectrum Disorders
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSanoeva Matlyuba Jaxonkulovna, Nazarov Alisher Ilkhomovich
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Sanoeva Matlyuba Jaxonkulovna, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article is dedicated to improving methods for rehabilitating psychoneurological signs of autism spectrum disorders (ASD). Timely diagnosis and a comprehensive medical-social and pedagogical treatment-restorative approach contribute to preparing a child with ASD for social life, improving their social adaptation, developing self-governance skills, reducing disability, reducing the need for medical care, ensuring their education in general education institutions, and minimizing problems arising within the family. Purpose of the research. Improvement of rehabilitation methods for children suffering from ASD, taking into account the autism triad, social inadequacy of relationships with others, sensory impairments, limitations, and stereotypical behavioral patterns. Research results. Early comprehensive rehabilitation method using medical, social, pedagogical, psychological, medical-psychological, physical comprehensive restorative procedures allows for patient preparation for social life, improvement of their activity in daily practice, self-control, restoration of relationships with others, and is of great importance in solving family problems, the stage of child integration into kindergarten and school. The use of neurological studies, special tests, and scales contributes to monitoring the recovery dynamics in ASD. Conclusion. Undoubtedly, the proposed methods are important for early diagnosis of ASD in children, choosing comprehensive early rehabilitation, preparing children for social life in early childhood, timely restoration of changes in consciousness, speech, articulation, movements, feelings, and behavior, prevention of severe complications, and have a positive impact on socio-medical and economic efficiency.
Keywords: Autism spectrum disorders, Diagnostics, Rehabilitation, Psychological, Medical, Pedagogical, Physical, Social assistance
Cite this paper: Sanoeva Matlyuba Jaxonkulovna, Nazarov Alisher Ilkhomovich, Principles of Rehabilitation of Psycho-Neurological Changes in Autistic Spectrum Disorders, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4124-4131. doi: 10.5923/j.ajmms.20251511.83.
Article Outline
1. Actuality of the Research
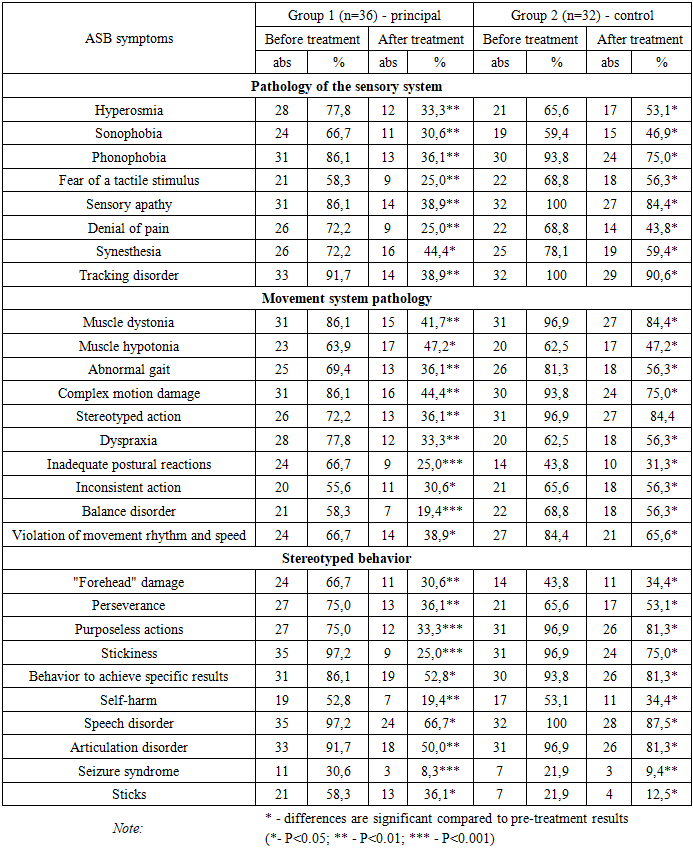
- The prevalence of Autism Spectrum Disorders (ASD) has shown a steady upward trend. According to earlier statistics, ASD was diagnosed in approximately 4–5 children per 10,000, whereas over the past 30–40 years this figure has increased to 50–116 cases in many countries. Such a sharp rise clearly underscores the high degree of relevance of this issue [2,7].In the process of clinical examination, data analysis, diagnosis, and the selection of treatment and rehabilitation methods for patients with ASD, it is essential to take into account not only the core clinical symptoms but also accompanying neurological alterations. In many cases, it is precisely the neurological manifestations that determine the specific nature of the disorder in autistic patients. The processes occurring in the brain play a crucial role in the manifestation of both the fundamental symptoms and associated neurological features of the disease.ASD encompasses a wide range of primary and neurological signs, among which significant difficulties in speech and language development are especially pronounced. Patients often experience challenges in communicating with close relatives, possess a limited vocabulary, and rely predominantly on nonverbal means of communication (such as gestures or pictograms) [3,9].Moreover, individuals with ASD frequently exhibit hypersensitivity to smell, taste, and light; may cover their ears tightly to avoid certain sounds (sonophobia); and display an extreme fear reaction to specific noises (e.g., from airplanes or vacuum cleaners) or tactile contact. At the same time, sensory indifference may be observed — such as failing to respond when called by name, ignoring loud noises, or showing apparent “deafness.” Other symptoms include self-injurious behavior, difficulty in recognizing facial expressions, and synesthesia (a condition in which stimulation of one sensory modality triggers perceptions in another — for example, auditory stimuli influencing visual or gustatory sensations).In addition, motor abnormalities are common: dystonia, atypical gait (such as walking on tiptoes), impaired balance and coordination, lack of control over complex motor actions, stereotyped or repetitive mechanical movements (such as finger, hand, or body rocking and circular motions), and a general preference for routine behavior. Motor system underdevelopment, muscle hypotonia, deficits in motor planning and organization (dyspraxia), inadequate postural responses, as well as disturbances in static and dynamic coordination, rhythm, and movement speed are also characteristic [4,10].Patients may exhibit slow, uncoordinated movements when walking, a forward-leaning head posture, absence of normal arm synergy, and an inability to maintain balance while standing. Alongside these symptoms, stereotypical behaviors are observed, including speech development disorders, impaired articulation, abnormal and self-injurious movements, seizures, and tics [5,12].
2. Initial Diagnosis and the "Autistic Triad"
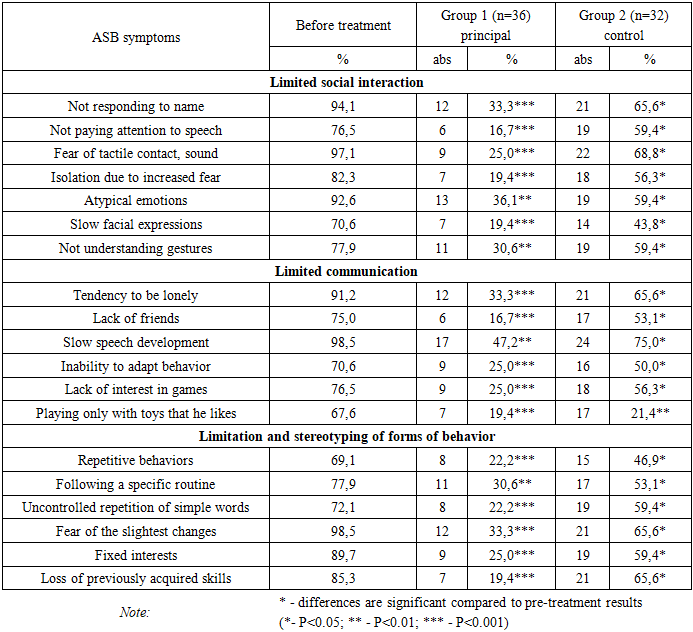
- The initial diagnosis of Autism Spectrum Disorder (ASD) is primarily based on the presence of what is known as the “autistic triad.” This triad manifests in various forms and includes the following three groups of characteristics [4,8,16]:• limitations in social interaction;• limitations in communication;• restricted and stereotyped patterns of behavior.When examining the features that fall within each group of the “autistic triad,” one encounters a number of distinctive and noteworthy phenomena.Limitations in social interaction are characterized by a lack of response to one’s name; disregard for speech directed toward the child; fear of tactile contact and certain sounds; social withdrawal resulting from anxiety in the presence of others; atypical emotional expression; poor facial mimicry; inability to interpret body language and gestures; and difficulty in maintaining eye contact [5,8].Limitations in communication involve a tendency toward solitude, absence of friendships, delayed speech development, inability to adapt behavior according to the situation, lack of interest in interactive games, and playing exclusively with personally preferred toys while ignoring others [1,16].Restricted and stereotyped patterns of behavior are marked by repetitive movements, strict adherence to routine, uncontrolled repetition of simple words, fear of minor changes, fixation on specific interests, and the loss of previously acquired skills [2,15].There are several distinct types of Autism Spectrum Disorders, which are differentiated based on the unique characteristics of each condition. According to the International Classification of Diseases, 11th Revision (ICD-11), ASD types are categorized primarily according to the degree of intellectual development and the presence or absence of functional language abilities. In the 10th Revision of the ICD (ICD-10), the following major types were identified [6,11,19]:1. Early Childhood Autism – characterized by delayed motor development, abnormal movements, avoidance of social contact, and limited vocabulary. For instance, an infant may fail to respond to their name by eight months of age; by twelve months, exhibit a limited number of gestures or movements; by eighteen months, demonstrate avoidance of communication, failure to comprehend speech, and engagement in unusual types of play; and by twenty-four months, show an inability to imitate actions, lack of social reciprocity, and the use of a restricted set of words. However, at this age, it remains difficult to predict the future severity of ASD [2,6,13].2. Kanner’s Syndrome – characterized by withdrawal into one’s inner world, lack of communication with the external environment, and echolalia (repetition of words or phrases). Although language may develop, it does not enable the individual to function fully in society and typically requires constant supervision [14].3. Asperger’s Syndrome – marked by egocentrism, perception of communication as insignificant, unusual or obsessive interests, and a low level of empathy. Despite these traits, motor development is generally normal, which often leads to this syndrome being mistaken for mere eccentricity [17].4. Rett’s Syndrome, although previously classified within ASD, is now regarded as a distinct genetic disorder associated with specific mutations. It occurs exclusively in females and is commonly characterized by the loss of purposeful hand movements and severe impairment of motor coordination [3,18].5. Adult Autism can manifest in two main forms. The first involves the persistence of childhood autism symptoms into adulthood, where the severity of manifestations may fluctuate over time; in such cases, psychotherapeutic intervention plays a crucial role. The second form appears in adulthood as a response to stress or other psychological factors — resembling a depressive condition. Over time, such individuals may experience significant deterioration in social functioning, actively avoid communication, neglect close relationships, withdraw from social contact, and show decreased concentration, passivity, and loss of interest. They often lose the ability to establish new relationships or interact effectively with others. Nevertheless, despite these communication difficulties, some individuals with adult autism are able to achieve notable professional success. Adult autism frequently presents atypically, meaning that not all components of the classical triad may be evident [18].6. High-Functioning Autism (HFA) – distinguished by a high level of intellectual ability and often regarded as a variant of Savant Syndrome, where superior IQ coexists with certain mental impairments. High-functioning autism may also coexist with other types of ASD, such as Kanner’s or Asperger’s syndromes [19].Thus, a review of the literature indicates that the diversity of ASD types, the variability of their clinical features and neurological manifestations, and the complexity of their progression — combined with pronounced cognitive and emotional disturbances and a profound impact on social life — present considerable challenges for both diagnosis and treatment. The limited efficacy of pharmacotherapy, the difficulties in selecting appropriate rehabilitation approaches, and the overlap of symptoms with other conditions emphasize the need for further refinement of early medical, neuropsychological, and pedagogical interventions. Such advancements are essential for improving rehabilitation outcomes, preparing children for social adaptation, and reducing disability rates.
3. Purpose of the Methodological Recommendations
- The purpose of the methodological recommendations is to improve rehabilitation approaches for children with Autism Spectrum Disorders (ASD), taking into account the limitations and stereotyped nature of the “autistic triad” — namely, restricted social interaction, impaired communication with others, sensory disturbances, and repetitive patterns of behavior and conduct.
4. Research Materials and Methods
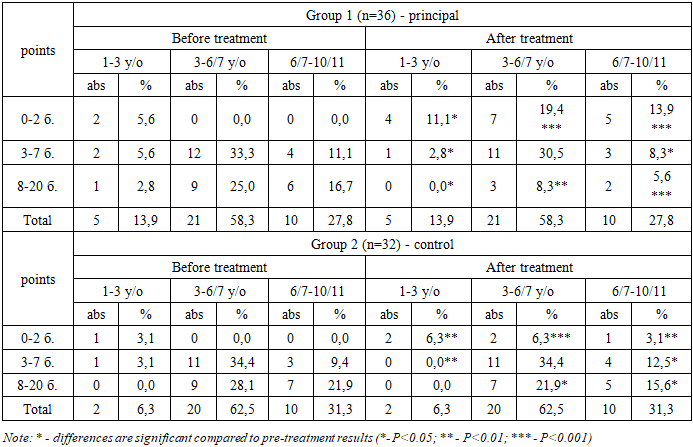
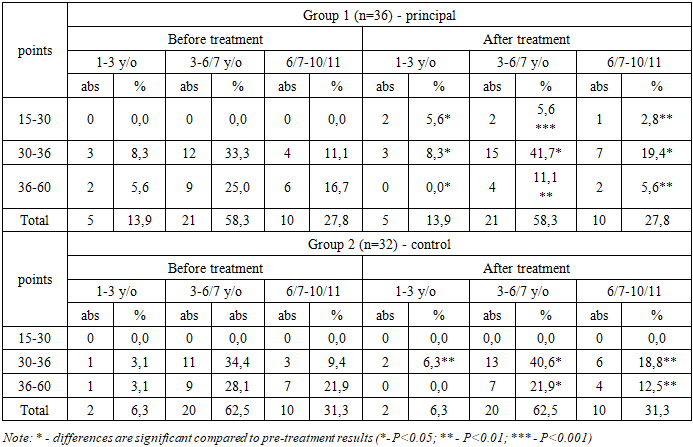
- This scientific study was devoted to analyzing the clinical features of Autism Spectrum Disorders (ASD) in children and, based on these findings, to developing and selecting appropriate rehabilitation methods.In total, 68 children (100%) — both boys and girls diagnosed with ASD — participated in the study. Based on the identified clinical characteristics, a comprehensive rehabilitation program was applied. The children were examined and treated at the Republican Mental Health Center (Bukhara Branch) and the “Alfa Medical Center” private clinic, both in inpatient and outpatient settings, during the period from 2022 to 2024.To ensure the reliability and validity of the research, all 68 children were divided into two groups:• Group 1 (Main Group) – 36 children (52.9%) who received the proposed comprehensive rehabilitation program;• Group 2 (Control Group) – 32 children (47.1%) with ASD who underwent conventional treatment (see Figure 1).
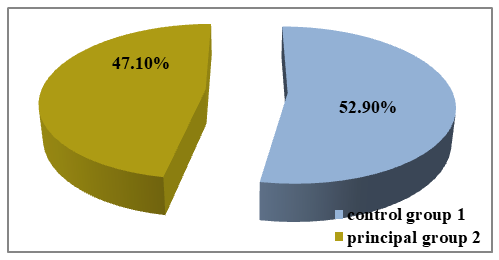 | Figure 1. Distribution of patients into groups |
|
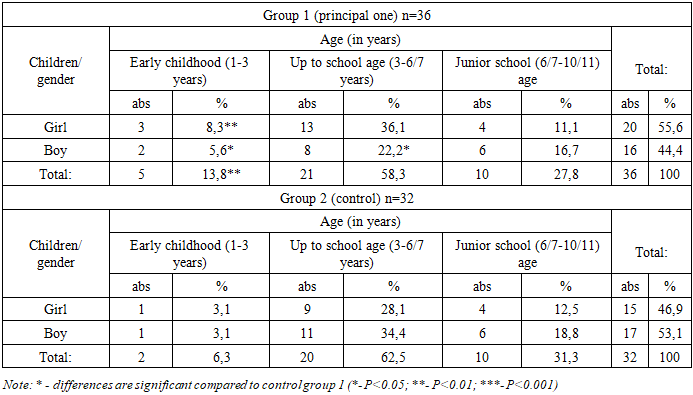
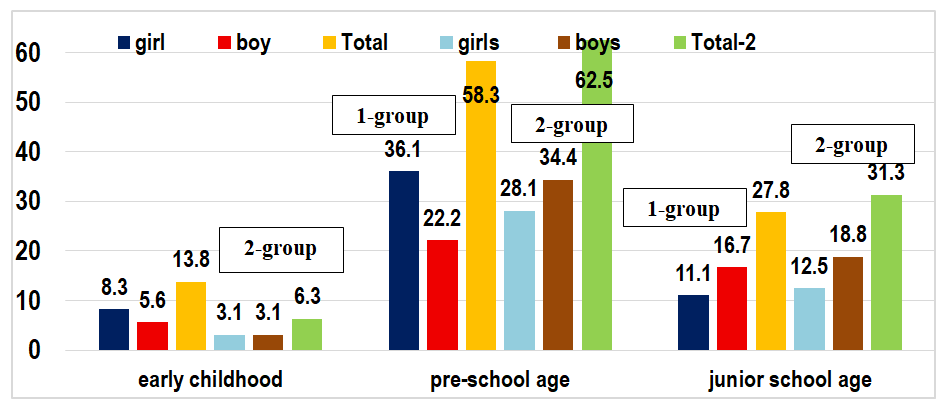 | Figure 2. Distribution of children in groups by age and gender |
|
|
|
|
5. Conclusions
- 1. Implementing the proposed comprehensive rehabilitation program from early childhood and continuing periodic interventions until the child reaches school age—incorporating medical, social, pedagogical, psychological, medical-psychological, and physical rehabilitation—prepares the child for social life, improves daily functioning, self-regulation, and social interaction, and significantly facilitates family-related challenges and the integration process into preschools and schools. The use of neurological markers, specialized tests, and scales allows for systematic monitoring of interventions in autism spectrum disorder (ASD).2. These methods enable early ASD diagnosis, selection of appropriate early rehabilitation strategies, preparation of the child for social life from infancy, and timely intervention in cognitive, speech, articulatory, motor, sensory, and behavioral domains. This reduces the risk of severe complications and positively impacts social, medical, and economic outcomes.3. The comprehensive rehabilitation program allows for early, qualified neurological, medical-psychological, pedagogical, and physical interventions, preventing profound disability, and supporting the child in independent functioning, social integration, and active participation in daily activities.