-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4117-4120
doi:10.5923/j.ajmms.20251511.81
Received: Oct. 28, 2025; Accepted: Nov. 20, 2025; Published: Nov. 24, 2025

Results of Endoscopic Examination of the Nasal Cavity in Patients with Deviated Nasal Septum Combined with Nasal Valve Insufficiency
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJamolbek A. Djurayev, Firdavs N. Norjigitov, Iroda T. Xudayberdiyeva, Gulnoza A. Abduholikova, Ilyosjon O. Soatov
Tashkent State Medical University, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

From a modern perspective, otorhinolaryngologists consider the nose as a paired organ, which implies the existence of certain coordination mechanisms for it as a single unit. The presence of a deviated nasal septum disrupts these mechanisms, leading to changes in the main functions of the nasal cavity and creating conditions for the formation of nasal obstruction. The leading role in the formation of chronic nasal obstruction is played by the nasal septum, nasal turbinates, and the lateral wall of the nasal cavity, which together form the nasal valve. Often, nasal obstruction associated with nasal septum deformation can create problems in the treatment of patients with severe concomitant somatic pathology. In patients with cardiovascular diseases, prolonged use of decongestants can have a systemic adrenomimetic effect (tachycardia, increased blood pressure).
Keywords: Nose, Nasal septum, Nasal valve, Nasal obstruction
Cite this paper: Jamolbek A. Djurayev, Firdavs N. Norjigitov, Iroda T. Xudayberdiyeva, Gulnoza A. Abduholikova, Ilyosjon O. Soatov, Results of Endoscopic Examination of the Nasal Cavity in Patients with Deviated Nasal Septum Combined with Nasal Valve Insufficiency, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4117-4120. doi: 10.5923/j.ajmms.20251511.81.
1. Introduction
- The displacement of the nasal septum can create certain technical difficulties when endonasal sanitizing or diagnostic surgical interventions are necessary. The classic submucosal resection of the nasal septum has several disadvantages [4,7]. First and foremost, there is insufficient visualization of the deep parts of the nasal cavity, which in turn leads to a greater risk of mucosal injury, excessive resection of its bone and cartilage framework, frequent damage to the sphenoid sinus, and sometimes to the structures of the sella turcica [8,11]. All of these shortcomings can be avoided during surgical interventions on the nasal septum under the supervision of video endoscopic systems. Targeted visualization allows for gentle manipulation in hard-to-reach sections of the nasal septum. Modern trends in septal surgery emphasize the importance of adhering to the principles of tissue-preserving and sparing resection of the bone and cartilage framework of the nasal septum. This is driven by surgeons' desire to reduce the risk of intra- and postoperative complications, which are largely associated with radical approaches during surgery.
2. Materials and Methods
- The use of endoscopic techniques in the preoperative stage allows for precise determination of the anatomical features of the structure and location of deformities in the bone and cartilage parts of the nasal septum, as well as structures forming the nasal valve, which can directly or indirectly influence the outcome of the operation.Modern endoscopic and radiological technologies have made it possible to differentiate a structure of the nasal septum known as the nasal septal swell body (NSB), which plays a significant role in regulating airflow in the nasal cavity. The nasal septal swell body is a thickening of the mucous membrane extending from the floor of the nasal cavity to the middle nasal concha. Histologically, the NSB differs from adjacent tissue in that it consists of layers of cylindrical ciliated cells, numerous mucous glands, and strips of connective tissue surrounding large vessels. This area contains more glandular elements than the inferior concha, but fewer than the nasal septum. It also has more venous sinuses than the rest of the nasal septum, but fewer than the inferior nasal concha. In clinical settings, little attention is paid to this area, although its histological structure and location in the nasal cavity indicate an important role in regulating airflow in the upper parts of the nasal cavity. Foreign literature describes cases of successful use of radiofrequency and cold plasma surgical devices to reduce the volume of this nasal septal zone and improve nasal breathing. The use of semiconductor lasers in correcting the nasal septal swell body is not described in current scientific literature and requires detailed study of the thermal effects of such lasers to determine a safe mode of exposure to the NSB area [17,22,23].
3. Results
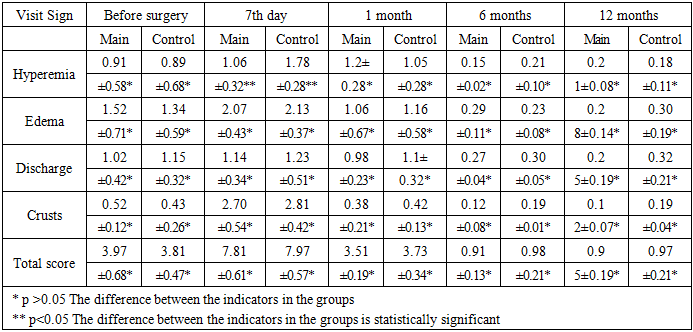
- We analyzed the outcomes of two surgical techniques for correcting nasal septum deformities and evaluated the effectiveness of surgical treatment in 135 patients randomized into two clinical groups: I (n=87, endoscopic septoplasty), II (n=48, classical nasal septum correction without endoscopic control).Dynamic monitoring of the prospective randomized clinical trial results was conducted using subjective (NOSE scale) and objective (CBCT of paranasal sinuses, MCT) examination methods. Additionally, we assessed the frequency of early and late postoperative complications: bleeding, nasal septal hematoma, nasal cavity synechiae, nasal septal perforations, secondary curvature of the septal framework, and saddle deformities of the external nose. The outlined patient examination protocol was performed before surgical treatment, then on the 7th day after surgery (nasal cavity endoscopy, questionnaires, MCT rate), after 1 and 3 months (nasal cavity endoscopy, questionnaires, MCT rate). Six months after surgical treatment (nasal cavity endoscopy, questionnaires, MCT rate, 3D CT).Endoscopic examination of the nasal cavity was conducted not only to determine the severity and type of nasal septal deformity but also to analyze the endoscopic clinical signs of the nasal cavity mucosa condition before and after surgery.We assessed the presence of mucosal edema in the nasal cavity, the degree of hyperemia, and the presence of discharge and crusts. Each clinical sign was evaluated on a point scale:0 - absence;1 - slight manifestation of the sign;2 - moderate presence of changes;3 - pronounced manifestation of the assessed criteria for the nasal mucosa condition.The condition of the nasal mucosa was evaluated during established observation periods. Then, the clinical sign scores were tallied, with the highest score corresponding to a negative result and vice versa. Before surgical treatment, the indicators were comparable in both groups, with the average total score for the studied features in the main (endoscopic) group being 4.11±0.76 points, and in the control (classical) group 4.52±0.41 points (p=0.37).Seven days after nasal septum correction, no statistically significant difference in the distribution of indicators was observed. The total score in the main group was 8.14±0.71, and in the control group 8.22±0.49 (p=0.59). Importantly, a positive trend was observed for the "hyperemia" parameter in the main (endoscopic) group - 1.18±0.29 points, compared to the control (classical) group - 2.12±0.19 (p<0.01). The remaining indicators of the mucosal condition were distributed without statistically significant deviations between the groups: edema in the main group was 1.89±0.48 points, in the control 2.24±0.29 (p=0.078); nasal discharge in the main group was 1.16±0.38 points versus 1.21±0.41 in the control group, (p=0.074); the presence of crusts in the nasal cavity in the main group was 2.65±0.49 points, in the control (classical) 2.81±0.42 points (p=0.083) (Table 1).
|
4. Discussions
- One month after the intervention, the average total score in the groups also showed no statistical difference: 4.1±0.34 in the main group and 4.22±0.41 in the control group (p=0.041). A similar trend in the distribution of the total score was observed in both groups after 3 and 6 months. At 3 months, the total score in the main group was 1.38±0.21, and in the control group 1.52±0.28 (p=0.06). The distribution of each criterion for the condition of the nasal mucosa was comparable in both groups. After 6 months, the total score decreased to 1.48±0.25 in the main group and to 1.36±0.32 in the control group. According to the results of long-term follow-up after 12 months, the total score in the main group was 1.44±0.25, and in the control group 1.31±0.33. Intragroup variance analysis for all final data at each observation point using post hoc analysis (Tukey test) showed that each criterion of mucosal condition and the total score differed significantly over time up to 6 months (p<0.05). This trend is clearly visible in the graph (Figure 1). No differences in indicators between 6-12 months were observed (p>0.05).
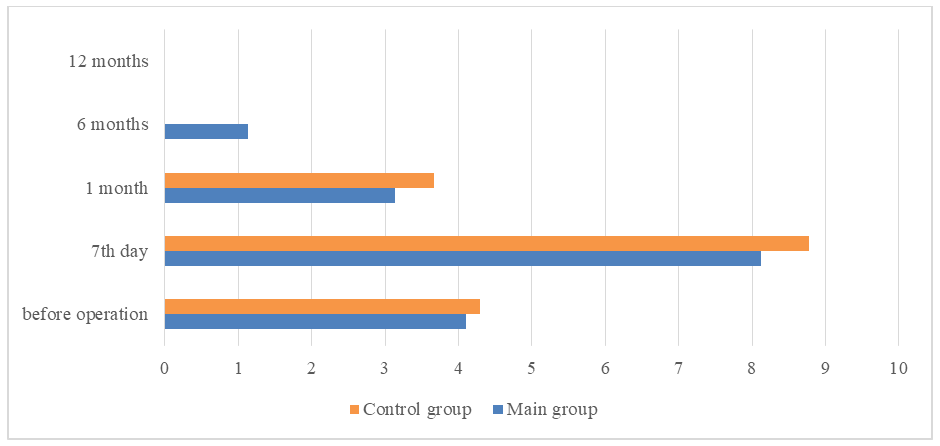 | Figure 1. Dynamics of total score distribution reflecting the nasal mucosa condition before and after surgery |
5. Conclusions
- Analysis of the obtained data revealed no differences between the studied groups in terms of the compared endoscopic indicators of nasal mucosa condition.Dynamic observation in both groups showed a decrease in scores characterizing the presence of specific endoscopic signs, indicating normalization of the nasal mucosa condition in both groups following surgical treatment.