-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4112-4116
doi:10.5923/j.ajmms.20251511.80
Received: Oct. 24, 2025; Accepted: Nov. 13, 2025; Published: Nov. 24, 2025

Modern and Improved Methods of Prevention of Acute Pancreatitis After Endoscopic Transpapillary Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAsadov Temur Shavkatovich, Hayitov Laziz Millionerovich, Askarov Pulat Azadovich, Daminov Firuz Asatulloevich, Abrorov Shahbozjon Nematzoda
Department of Surgical Diseases and Transplantology, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Askarov Pulat Azadovich, Department of Surgical Diseases and Transplantology, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction. Although it has already been proven that the treatment of patients with complicated cholelithiasis and mechanical jaundice using endoscopic transpapillary interventions is the gold standard, studies and experiments show that various complications are observed in this practice and confirm that it is not completely safe. The aim of this study based on our experience, was to analyze the percentage of acute postoperative pancreatitis and determine tactics to reduce the percentage of this complication. Materials and methods. A retrospective analysis of endoscopic transpapillary interventions outcomes was conducted in 244 patients from 2022 to 2025. Patients with signs of acute pancreatitis after admission to the clinic were excluded from the study. Although 90% of these patients successfully underwent endoscopic transpapillary interventions, halting disease progression and avoiding fatal complications, we excluded them from the study group, as our primary goal was to determine the incidence of acute postoperative pancreatitis specifically after endoscopic transpapillary interventions. Results. In the postoperative period, transient hyperamylasemia, with a rise no more than three times above normal, without clinical signs of pancreatitis, was observed at approximately the same rate in each group, averaging 13-18% of cases. To determine the severity of acute pancreatitis, we followed the classification adopted at the 1992 Atlanta expert meeting. The clinical picture of mild acute postoperative pancreatitis (APP), with complete relief by conservative treatment, was more often observed in the third group - 7.9%, in the first group - 4.4%, in the second group - 2.5%. Conclusion. Therefore, the problem of preventing acute postoperative pancreatitis developing after endoscopic endoscopic pancreatitis is still controversial and requires more in-depth research. In our opinion, the main causes of this complication are a combination of patient and interventional risk factors, as well as tactical and technical errors during its implementation.
Keywords: Endoscopic transpapillary interventions, Acute postoperative pancreatitis, Stenting of the main pancreatic duct
Cite this paper: Asadov Temur Shavkatovich, Hayitov Laziz Millionerovich, Askarov Pulat Azadovich, Daminov Firuz Asatulloevich, Abrorov Shahbozjon Nematzoda, Modern and Improved Methods of Prevention of Acute Pancreatitis After Endoscopic Transpapillary Surgery, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4112-4116. doi: 10.5923/j.ajmms.20251511.80.
1. Introduction
- Although it has already been proven that the treatment of patients with complicated cholelithiasis and mechanical jaundice using endoscopic transpapillary interventions is the "gold standard," studies and experiments show that various complications are observed in this practice and confirm that it is not completely safe [1,2]. One of the most common complications after endoscopic transpapillary interventions (ETI) is the development of acute postoperative pancreatitis (APP). The risk of developing this complication has its own characteristics and largely depends on the intervention technique and the individual characteristics of the patient. According to experts in this field, acute postoperative pancreatitis is a complication that is insufficiently controlled and predictable from a preventive point of view. If this complication is observed despite timely, early and active treatment, it can rarely result in death [3,4]. An analysis of the literature has shown that the incidence of acute postoperative pancreatitis has an alarming rate of 1% to 34%. This is explained by the following factors.Firstly, there are clear discrepancies in the definition and analysis of the concept of transient hyperamylasemia (elevated blood α-amylase levels). According to some authors, the diagnosis of acute postoperative pancreatitis is based on any increase in blood α-amylase levels [5]. Other authors diagnose acute postoperative pancreatitis when it is combined with an elevated blood α-amylase level and pain syndrome, while other authors take into account structural changes in the pancreatic parenchyma based on the patient's developing clinical signs and ultrasound or CT findings [6].Secondly, the risk of developing this complication is directly related to the scope and cost of ETI and the purpose of its implementation. When comparing the incidence of acute postoperative pancreatitis with that of limited interventions in the gallbladder and transpapillary treatment for pancreatic pathology, they should be differentiated [7].Thirdly, in our opinion, correct assessment of the state of the major duodenal papilla (MDP) and its location relative to the diverticula during duodenoscopy, correct selection and use of the instruments available in our arsenal at each stage of the intervention, even control of the caulator mode and current during sphenctrotomy, skillful execution of actions at each stage of the intervention with 1-2 attempts, and most importantly, without rushing and without losing control when eliminating complications during surgery, the correct choice of methods for eliminating complications and the instruments used [8].Fourth, a clear correlation has been demonstrated between the specialist's experience and the number of ERCPs performed in a center with the incidence of postoperative complications. According to the data, the incidence of complications is 3 times higher (7.1%) in centers that perform fewer than 200 ERCPs per year, while in centers that perform more than 200 ERCPs, this figure was 2% (p < 0.001) [9].A study of the incidence and risk factors for acute postoperative pancreatitis has been the goal of a number of prospective analyses not only in our country but also in countries with developed medicine. In 1996, Freeman et al. noted that in patients who underwent ETI in 1963, acute postoperative pancreatitis developed in 6.7% of cases. Similar data were also recorded in experiments by M.I. Bykov in 2024, where an analysis of ETI in 1,600 patients showed that acute postoperative pancreatitis developed in 6.85% of cases, and the mortality rate from this complication was 0.33% [10].According to foreign authors, the main risk factors for the development of acute postoperative pancreatitis are: patient age, female gender, history of pancreatitis, presence of inflammation in the major duodenal papilla, difficult or complex cannulation and atypical papillosphincterotomy, introduction of contrast agent into the Wipsung duct and absence of biliary hypertension [11]. Based on the data obtained as a result of the study, it is observed in women 14.9% more often than in men, is 10% more common in patients under 50 years of age, 26.4% more common in patients with preoperative pancreatic pathology, significantly increases by 37.5% in the presence of CDS pathology (papillitis, parapapillary diverticulum), and the introduction of a large amount of contrast agent into the lumen of the pancreas and an increase in pressure there increases the risk of pancreatitis by 84.6% [12]. Most authors point to damage to the orifice or distal portion of the Wirsung duct due to mechanical and thermal effects on the endothelial duct, leading to smooth muscle spasm and edema. Inflammation of the Wirsung duct mucosa with localized edema or the insertion of special instruments into the duct cavity during surgery and mechanical tissue damage are also associated. Pancreatic damage is caused by changes in osmotic and hydrodynamic pressure during the administration of contrast medium into the pancreatic ducts. Bile and contrast leakage into the pancreatic ducts due to reflux during forced contrast injection into the bile ducts.Compression of the pancreatic parenchyma during aggressive extraction of stones from the bile ducts, balloon dilation of the terminal common bile duct or the large bile duct. Recently, prophylactic replacement of the Wirsung duct has been widely reported as one of the methods for the prevention and treatment of acute postoperative pancreatitis [13]. Despite the fact that stenting of the Wirsung lumen has demonstrated high efficiency in the complex treatment and prevention of ACS, some authors recommend using the stent with great caution, since its migration into the channel, if a very narrow stent cavity becomes blocked due to obstruction, can develop a severe complication leading to a fatal outcome, i.e., pancreatic necrosis. Thus, despite the widespread coverage and analysis of this problem in the literature, the introduction of improved interventional methods, the use of new models of endoscopic instruments, as well as the improvement of manipulation techniques, the etiopathogenetic factors causing this complication remain. The aim of this study based on our experience, was to analyze the percentage of acute postoperative pancreatitis and determine tactics to reduce the percentage of this complication.
2. Materials and Methods
- A retrospective analysis of ETI outcomes was conducted in 244 patients from 2022 to 2025. Patients with signs of acute pancreatitis after admission to the clinic were excluded from the study. Although 90% of these patients successfully underwent ETI, halting disease progression and avoiding fatal complications, we excluded them from the study group, as our primary goal was to determine the incidence of acute postoperative pancreatitis specifically after ETI.Given the literature data demonstrating that differences in study groups can influence the assessment of the incidence of acute postoperative pancreatitis, we conducted an analysis in three groups of patients. The first group consisted of 206 (84.7%) patients with complicated cholelithiasis. The second group consisted of 27 (11.3%) patients with malignant obstructive jaundice, recruited for the purpose of bile duct decompression. The third group consisted of 11 (4.0%) patients with jaundice due to benign diseases of the hepatopancreatoduodenal zone.For preoperative prophylaxis, most patients received Contrycal 10,000 IU intravenously. Literary data on the efficacy of Contrycal, a synthetic Sandostatin analogue, are conflicting. Contrycal has been shown to significantly increase basal pressure and the frequency of contractions of the simple medullary sphincter, which leads to impaired outflow through the tubular system. The decrease in pancreatic secretion during octreotide administration may, in itself, negate the rather positive effect. Many authors note that the use of the nonsteroidal anti-inflammatory (NSAID) Diclofenac rectal suppository in combination with a proteolytic enzyme is highly effective in the prevention of acute postoperative pancreatitis. Recently, we have begun using NUC rectal suppositories, and it should be acknowledged that the initial results demonstrate multiple advantages in terms of both efficacy and cost.In addition, to reduce the risk of developing acute postoperative pancreatitis, we comprehensively used various technical and tactical methods of preoperative preparation, performing interventions under intravenous or general combined anesthesia, conducting intensive care in the postoperative period, and, relying on our experience and capabilities (equipment in our arsenal), we improved various technical and tactical methods during surgery and, of course, did not neglect the initiation of conservative treatment for the presence of pancreatitis if our patients had factors confirming pancreatitis before surgery.Avoid unnecessary contrast injection into the GB: Using a soft-tip guidewire to determine the direction of the bile ducts and the Wirsung duct prevents unnecessary contrast injection into the Wirsung duct. When performing CDS cannulation, we precisely check the catheter position to visualize the common bile duct and the direction of the Wirsung duct, thereby preventing approximate contrast injection.Avoiding lengthy attempts at gallbladder cannulation: in the presence of anatomical changes in the duodenal canal area, such as deformity of the descending duodenum, the presence of diverticula, the size and length of the ampulla and longitudinal fold, variations in the duodenal canalization angle, or hemostatic disorders, we prefer to perform atypical EPST layer by layer to gradually prevent tissue differentiation impairment, thereby avoiding lengthy and complex cannulation attempts. In our opinion, the duration and number of gallbladder cannulation attempts should be strictly individualized and as short as possible.Preferring the "CUT" mode when performing EPST: To reduce burn injury to the large duodenal tissue, emphasis should be placed on performing EPST in the "CUT" mode whenever possible. Correct and rational use of this mode significantly reduces bleeding and burns to surrounding tissues, thereby preventing the development of acute postoperative pancreatitis.The use of two wires for prophylactic APP stenting, nasopancreatic drainage, or complex cannulations (Fig. 1). APP prosthetics is performed during prolonged procedures during pancreatic stenosis, in the presence of signs of impaired contrast medium flow from the stenotic papillary system and ducts (Fig. 2), to stop bleeding above the APP, and in the presence of multiple risk factors for acute postoperative pancreatitis.
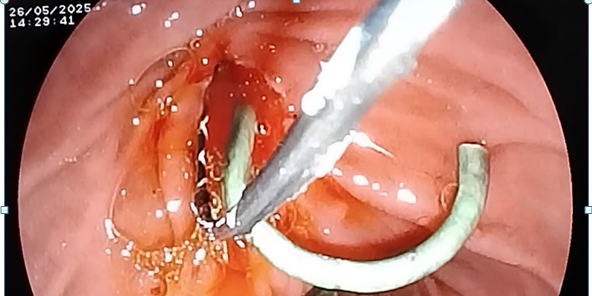 | Figure 1. Cannulation of the gallbladder with a guidewire (wire). Stanling of the APP road |
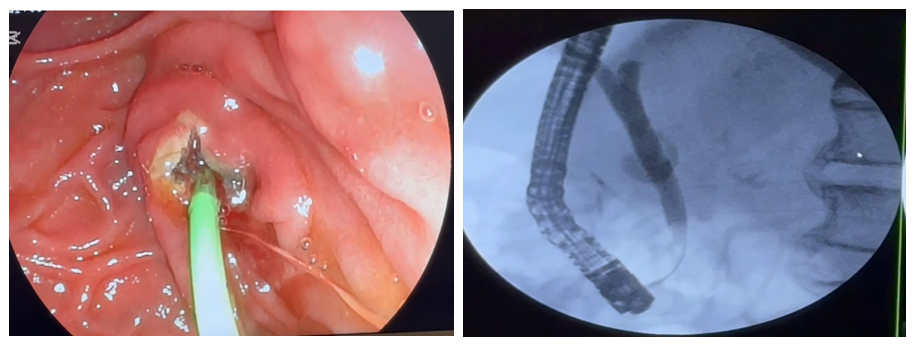 | Figure 2. To prevent the development of acute pancreatic insufficiency against the background of APP stenting, stenosing papillitis and impaired evacuation of contrast agent into the gallbladder |
3. Results
- In the postoperative period, transient hyperamylasemia, with a rise no more than three times above normal, without clinical signs of pancreatitis, was observed at approximately the same rate in each group, averaging 13-18% of cases. To determine the severity of acute pancreatitis, we followed the classification adopted at the 1992 Atlanta expert meeting.The clinical picture of mild acute postoperative pancreatitis (APP), with complete relief by conservative treatment, was more often observed in the third group - 7.9%, in the first group - 4.4%, in the second group - 2.5%.Severe acute postoperative pancreatitis (APP) developed in 4 patients (1.8%) in the first group, in 2 patients (7%) in the second group, and in 2 patients (20%) in the third group, which required long-term treatment of the patient in the intensive care unit or additional surgical interventions.In cases of acute postoperative pancreatitis, conservative treatment was used in most cases, along with minimally invasive procedures if complications arose. Patients lost their lives in four patients in the first group and one woman in the third group. The overall mortality rate was 0.2% across the three groups. Since 2022, if acute pancreatitis is diagnosed in the early preoperative period, we have been using endoscopic stenting of the pancreatic duct to restore normal pancreatic fluid outflow. Pancreatic stents with a diameter of 5 Fr and a length of 5-7 cm were used for prosthetic placement. Pigtail stents were preferred to prevent migration from the internal ducts. In the early preoperative period, stenting of the pancreatic duct was successfully performed in 14 (87.5%) of 16 attempts. In each case of successful stenting, the clinical picture of acute pancreatitis was predicted, but one patient died due to multiple organ failure. After the symptoms of acute pancreatitis subsided, the stent was removed within 5-14 days.It should be noted that in some cases, the stent may spontaneously migrate into the intestine, but endoscopic monitoring requires fluoroscopy to detect migration from the internal duct. We believe that prophylactic APP stenting is necessary to stop endoscopic bleeding, as any mechanical or thermal hemostasis methods can create a blockage over the pancreatic duct and cause acute pancreatitis (Fig. 3). In our practice, we also observed the development of clinically significant acute pancreatitis with ongoing bleeding from the EPST zone of the pancreatic duct in four clinical cases, and we identified the formation of dense blood clots in the ampulla area. These patients successfully eliminated the symptoms of pancreatitis and bleeding through delayed endoscopic hemostasis and APJ stenting.
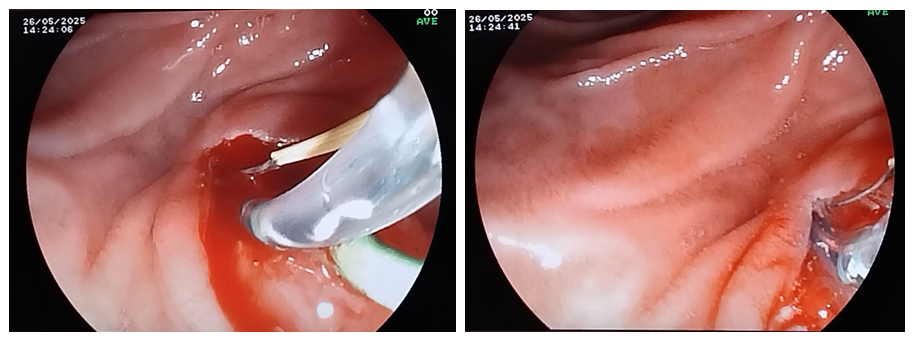 | Figure 3. Prophylactic stenting of the APP, performing thermocoagulation to stop bleeding from the papillotomy incision |
4. Conclusions
- Therefore, the problem of preventing acute postoperative pancreatitis developing after endoscopic endoscopic pancreatitis is still controversial and requires more in-depth research. In our opinion, the main causes of this complication are a combination of patient and interventional risk factors, as well as tactical and technical errors during its implementation. The mechanism for reducing the progression of acute postoperative pancreatitis is the presence of clear clinical indications for endoscopic pancreatitis, active monitoring of the patient's condition after the intervention, advanced training of physicians, and adherence to the algorithm of therapeutic and preventive measures, which implies a wider use of modern endoscopic treatment technologies. The algorithm for the prevention of post-manipulation complications developed by us, introduced into clinical practice, contributed to a decrease in the percentage of acute postoperative pancreatitis, and the obtained results demonstrate a relatively low percentage of acute postoperative pancreatitis, especially in its severe forms, compared with general literature data. Although in our practice, APP was a fairly effective method of endoscopic stenting, complex treatment and prevention of acute postoperative pancreatitis, we believe that its use is correct and effective only in the presence of clear indications and sufficient professional experience in performing interventions on the pancreatic ducts.