-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4108-4111
doi:10.5923/j.ajmms.20251511.79
Received: Oct. 21, 2025; Accepted: Nov. 19, 2025; Published: Nov. 24, 2025

Prediction and Prevention of Pathological Course of Pregnancy in Adenomyosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMadolimova N. Kh.
Department of Obstetrics and Gynecology, Reproductive Sciences, Tashkent State Medical University, Uzbekistan
Correspondence to: Madolimova N. Kh., Department of Obstetrics and Gynecology, Reproductive Sciences, Tashkent State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In recent years, determining the relationship between adenomyosis and the pathological course of pregnancy has generated considerable interest. A study of the pregnancy and childbirth course was conducted in 215 pregnant women from 2022 to 2024. The study group consisted of 103 pregnant women with varying degrees of adenomyosis and a comparison group of 112 pregnant women without adenomyosis. Comprehensive preconception preparation with epigenetic therapy, by eliminating foci of adenomyosis and preclinical prediction and prevention of complicated pregnancy, reduced the incidence of pregnancy and childbirth complications, including the incidence of preterm birth by three times and perinatal fetal loss by more than three times.
Keywords: Complications of pregnancy and childbirth, Adenomyosis
Cite this paper: Madolimova N. Kh., Prediction and Prevention of Pathological Course of Pregnancy in Adenomyosis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4108-4111. doi: 10.5923/j.ajmms.20251511.79.
Article Outline
1. Introduction
- Despite the steady decline in maternal and perinatal morbidity rates in Uzbekistan, the health of women of reproductive age continues to be characterized by significant somatic burden, an increasing incidence of gynecological pathologies, accompanied by obstetric and perinatal complications and a high level of morbidity in newborns upon the onset of pregnancy. Reserves for reducing maternal and perinatal morbidity include pre-pregnancy preparation with therapy for somatic pathology, elimination of gynecological diseases, and prediction and preclinical diagnosis of gestational complications [1].A pregnant woman with adenomyosis experiences significant stress, leading to an imbalance in the implantation and placentation processes. Therefore, it is important to identify biochemical markers for complications during pregnancy and childbirth in women with adenomyosis [4,5].In recent years, there has also been considerable interest in determining the relationship between various forms of endometriosis and abnormal pregnancy outcomes [3,7]. Epigenetic studies, which are closely linked to the programmed development of various pregnancy pathologies under the influence of various factors, are playing an important role. According to literature data, these changes have been established for some pathological conditions, such as preeclampsia and miscarriage [6].The identification of changes in the level of trophoblasticβ-1–glycoprotein in relation to gestational complications, as a marker of diagnosis and prognosis in women with adenomyosis, remains virtually unexplored, which determines the relevance of the problem and the conduct of research, the study of obstetric and perinatal complications resulting from adenomyosis, the characteristics of the course of pregnancy and childbirth, and the dependence on the management method requires further research. The obtained data can be used to formulate an optimal prevention strategy and optimize diagnostic and treatment tactics in pregnant women with adenomyosis [8,9,10].Despite the improvement of modern methods of diagnosis, prevention and treatment, many complications in pregnant women with adenomyosis remain unresolved, poorly studied and require further research in this area.
2. Purpose of the Research
- The aim of the study was to evaluate pregnancy and birth outcomes in patients with adenomyosis.
3. Materials and Methods
- The study was conducted in several stages. At the first stage, the aim of the study was to determine the frequency and structure of obstetric and perinatal complications in 103 women with various forms of adenomyosis aged 25 to 35 years (average age - 29.6 ± 4.2 years) who underwent outpatient treatment in the department of the 9th obstetric complex and the private clinic NS Medical in Tashkent for the period from 2021-2024. Depending on the type of adenomyosis, the women were divided into groups: Group 1 consisted of 82 women with diffuse adenomyosis, including 69 women with grades 1-2 adenomyosis and 13 women with grade 3 adenomyosis; Group 2 included 21 women with focal adenomyosis. One hundred and twelve women without adenomyosis served as controls.The second stage after adenomyosis treatment involved pregnancy planning. Upon pregnancy, 66 (64.1%) women with adenomyosis were assessed for trophoblastic β-1-glycoprotein levels during gestation, various obstetric and perinatal complications, and their prognostic significance was determined.Depending on the management, pregnant women were divided into subgroups. Subgroup 1 consisted of women (n=37), of which 26 women had a diffuse form of adenomyosis and 11 with a focal form, who were prescribed micronized progesterone at a dose of 400 mg per day up to 16 weeks of pregnancy and acetylsalicylic acid 75 mg per day from 12 to 36 weeks of pregnancy as a preventative measure against gestational complications. Subgroup 2 consisted of pregnant women (n=29), of whom 21 had diffuse adenomyosis and 8 had focal adenomyosis, who were managed conventionally. The comparison group consisted of 42 pregnant women without adenomyosis.Clinical research methods included collecting anamnesis with a study of the patient's complaints, assessing the nature of menstrual and reproductive function, studying the outcomes of pregnancy and childbirth, and somatic and gynecological history data. In some cases, patients were consulted by related specialists based on specific indications. A physical examination included a physical examination and a gynecological examination to determine the type and severity of adenomyosis. Serum trophoblastic β-1-glycoprotein levels were measured over the course of gestation.
4. Results and Discussion
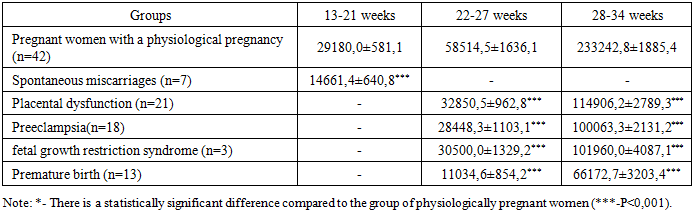
- In stage I, adenomyosis was treated with dienogest-containing oral contraceptives (Zhanin, diaenogest 2 mg/day) for 6 months (for greater lesion clearance and contraception) in combination with indole-3-carbinol (I3C) administered continuously (200 mg/day) for 1 year/until pregnancy, which affects the epigenetic link in the pathogenesis of adenomyosis. In adenomyosis, the mechanism of indole-3-carbinol is to reduce estrogen-dependent and estrogen-independent proliferation, suppress inflammation, stimulate apoptosis, stabilize the genome by inhibiting DNA methylation and suppressing DNA methyltransferase, and suppress proliferation and neoangiogenesis processes. An assessment of the severity of pain syndrome before the start of therapy during menstruation using a visual analogue scale (VAS) showed that 79.6% (n=82) of those examined in the main group characterized the pain as moderate to severe and rated it from 6 to 8 points (6.6±0.8 points).The next stage of the study was pregnancy planning with the elimination of pathology symptoms and improvement of blood circulation in the uterine vessels after treatment of adenomyosis.Within a year of completing therapy, 66 out of 103 women (64.1%) became pregnant. Among those with diffuse adenomyosis, pregnancy occurred in 47 of 82 women (57.3%), which is 1.6 times less frequent than in those with focal adenomyosis (90.5%) (19 of 21). Pregnancy rates also varied depending on the treatment method.To prevent miscarriage in women with adenomyosis, micronized progesterone was prescribed at a dose of 400 mg per day until the 16th week of pregnancy and acetylsalicylic acid 75 mg per day from 12 to 36 weeks of pregnancy.Based on management, 66 pregnant women with adenomyosis were divided into groups. Group A consisted of 37 women who received prophylaxis for complications, including 26 women with diffuse adenomyosis and 11 women with focal adenomyosis. Group B consisted of 21 women who did not receive prophylaxis for complications, including 21 with diffuse adenomyosis and 8 with focal adenomyosis.An analysis of the course of pregnancy in women with adenomyosis showed that in the group of pregnant women who received prophylaxis, a more favorable course of pregnancy was observed, as evidenced by a lower number of gestational complications than in the group without prophylaxis of complications. In women with adenomyosis, pregnancy was complicated by spontaneous miscarriages and premature births in 13.8% and 24.1% of women with adenomyosis, managed traditionally, and were higher than the rates of pregnant women with prophylaxis by 1.7 (8.1%) and 1.5 (16.2%) times. A distinctive feature of pregnant women with adenomyosis, managed traditionally, was the presence of a higher number (13.8%) of very early and early premature births, the frequency of which was 2.6 times higher than in the group of women receiving prophylaxis.In pregnant women with adenomyosis who did not receive prophylaxis for obstetric complications, a significant (p<0.05) increase in the incidence of hypertensive disorders was observed – 27.6%, with severe preeclampsia developing in 10.3%. This complication was 2 times less common in the group of women with adenomyosis who received prophylaxis (13.5%) and did not differ from the control group (10.9%).Serious obstetric pathologies such as placenta previa and placenta previa were more frequently observed in the group of women with adenomyosis who did not receive comprehensive treatment, accounting for 6.9% and 10.3%, respectively. Placenta previa was also observed in the group of women receiving indole-3-carbinol and prophylaxis, but at a 1.9-fold lower rate (5.4%).A study of the course of labor showed that 13.8% of women in labor with adenomyomas developed weakness of labor, which is 1.7 times more common than the group receiving indole-3-carbinol and prevention of gestational complications. Another relatively common complication during childbirth was abnormally dense placental attachment, with a rate of 10.3% and 8.1%. The rate of cesarean section in pregnant women with adenomyosis who did not receive indole-3 carbinol or prophylaxis for complications was higher than the population average and was 27.6%.A complication in women with adenomyosis was early postpartum hemorrhage, which was observed in 17.2% of women in labor with adenomyosis who received traditional care and in 13.5% who received prophylaxis. The postpartum period in women with adenomyosis was also characterized by high rates of uterine subinvolution (37.9%), which was 1.6 times higher than the rates in the group of women with adenomyosis who received comprehensive care (24.3%).The frequency of timely births was significantly higher in the group of women with adenomyosis who received indole-3 carbinol before pregnancy and micronized progesterone and acetylsalicylic acid before 16 weeks of gestation (χ2=6.37; p<0.05), while the frequency of premature births was significantly lower by 1.5 times (χ2=3.52; p<0.02), and the frequency of fetal loss was more than 1.5 times (χ2=3.69; p<0.05).A more favorable course of pregnancy and childbirth was reflected in the condition of the newborns. The weight and height indicators of full-term newborns in the group of women with adenomyosis who received prophylaxis ((3413.07±70.05 g va 51.24±0.45 cm) were significantly higher than in the compared group of women without therapy ((3080.3±90.06 g va 49.98±0.62 cm). The fetal Apgar scores were 7.6±0.1, 6.8±0.2, and 6.6±0.2 (P<0.01), respectively. As a result of comprehensive management of pregnant women with adenomyosis, the number of healthy newborns increased more than threefold, and their incidence decreased by half.We examined pregnant women in the main group (n=66), who were divided into subgroups based on management: Subgroup 1 consisted of 37 pregnant women with adenomyosis who received prophylaxis with micronized progesterone and acetylsalicylic acid, and subgroup 2 consisted of 29 pregnant women with adenomyosis who received traditional management. The comparison group consisted of 42 pregnant women without adenomyosis.In pregnant women with adenomyosis who developed the threat of preterm labor (TPL), even with prophylaxis, the TBG concentration was 25,859.44±2.99 ng/ml, which was 2 times lower than the values in the group with a normal pregnancy. In contrast, in pregnant women who developed the threat of preterm labor without prophylaxis, the TBG level dropped sharply by 3.6 times to 11,016.65±3.57 ng/ml. A strong inverse correlation (r=-0.95, p=0.0034) was established between the level of TBG at 32-34 weeks and clinical symptoms of termination of pregnancy.Despite maintenance therapy, 24.1% of pregnant women in the main group with adenomyosis developed premature birth, and 16.2% of women with adenomyosis who received prophylaxis, which is 1.5 times less common. Consequently, based on the change in the level of TBG in patients with the threat of premature birth, it is possible to judge the effectiveness of the preservation therapy, which is confirmed by the data of the correlation analysis (r=0.85, p=0.019).A study of TBG during labor revealed a sharp decrease in its level, averaging 72,698.7±6.3 ng/ml, which was 3.2 times lower than prenatal levels. This can be explained by the premature reduction of the placenta observed during preterm labor.This, in turn, will allow, based on the study of the level of TBG, to predict obstetric complications in women with adenomyosis at the preclinical stage.
|
5. Conclusions
- Comprehensive pre-conception preparation with epigenetic therapy due to the leveling of adenomyosis foci and preclinical prediction and prevention of complicated pregnancy course reduced the incidence of complications of pregnancy and childbirth (χ2=6.37; P<0.05), the incidence of premature birth by 3 times (χ2=3.52; P<0.02) and perinatal fetal loss by more than 3 times (χ2=3.69; P<0.05).From the above it follows that, based on the TBG indicator, it is possible to predict the outcome of pregnancy with a high degree of probability depending on the level of this marker. These indicators also make it possible to develop pregnancy management tactics, that is, the ability not only to predict premature termination of pregnancy, but also to carry out targeted treatment and preventive measures to prolong it.