-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4105-4107
doi:10.5923/j.ajmms.20251511.78
Received: Oct. 21, 2025; Accepted: Nov. 15, 2025; Published: Nov. 24, 2025

Features of Clinical and Neurological Status in Children with Delayed Speech Development
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBerdieva Khilolakhon Umarjonovna
PhD., Doctoral Student of the Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Berdieva Khilolakhon Umarjonovna, PhD., Doctoral Student of the Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

A total of 90 children aged 3 to 7 years were examined and divided into two groups: the first included children with delayed speech development (DSD) associated with attention deficit hyperactivity disorder (ADHD), and the second comprised children with DSD caused by residual-organic brain lesions (ROL). It was established that children with DSD combined with ADHD demonstrated a significantly higher speech development coefficient (mean 24.9 ± 3.9) compared to children with residual-organic brain damage (17.7 ± 6.7; p < 0.001). These findings indicate a more favorable functional prognosis in cases of functional speech pathology. In contrast, children with organic brain lesions showed more pronounced neurological and cognitive impairments, suggesting delayed maturation and reduced functional activity of cortical structures.
Keywords: Delayed speech development, ADHD, Residual-organic lesions, Children, Speech function, Cognitive development
Cite this paper: Berdieva Khilolakhon Umarjonovna, Features of Clinical and Neurological Status in Children with Delayed Speech Development, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4105-4107. doi: 10.5923/j.ajmms.20251511.78.
Article Outline
1. Introduction
- In modern pediatric neurology, delayed speech development (DSD) is considered one of the most common neuropsychological disorders of early childhood. The formation of speech in children is a complex, multilevel, and multifactorial process based on physiological mechanisms and closely linked with social, cultural, and psychological conditions [7,9].Speech function is highly sensitive to various adverse influences, and its disturbances often lead to significant consequences, including difficulties in cognitive and communicative activities, as well as deviations in neuropsychological and social development. These factors are especially critical during early childhood, when the fundamental mechanisms of speech are being formed, ensuring its further development [2,4].In recent years, the issue of speech disorders in children has gained particular importance for specialists in various fields—neurologists, speech therapists, psychologists, and educators. This relevance is determined not only by the growing prevalence of this disorder but also by the difficulties in its early diagnosis and timely correction. According to various studies, the prevalence of DSD among children ranges from 5% to 25% [1,6].Etiologically, DSD may result from both organic and functional factors. Among the organic causes, leading roles are played by perinatal lesions of the central nervous system, brain injuries, neuroinfections, cerebral palsy, epilepsy, neurosensory hearing loss, and other pathological conditions. These factors affect brain structures responsible for the regulation of motor and cognitive processes, thereby slowing down speech development [3,7,8].In contrast, functional forms of DSD are more often associated with adverse psychoemotional conditions, disturbances in family communication, limited speech environment, and pedagogical neglect [2,5].
2. Purpose of the Research
- The purpose of this research was to determine the clinical and neurological characteristics of delayed speech development (DSD) in children, to analyze the relationship between the etiology of speech delay and neurological status, and to identify prognostic markers that differentiate functional from organic forms of speech disorders. The study also aimed to establish clinical criteria that could facilitate early diagnosis and timely therapeutic intervention, thereby improving the overall outcomes of neurodevelopmental rehabilitation in affected children.Objective is to determine the clinical and neurological features and the relationship between the type of speech disorder and neurological status in children with delayed speech development of various origins.
3. Materials and Methods
- The study was conducted at the clinic of Tashkent Pediatric Medical Institute. A total of 90 children aged 3 to 7 years with delayed speech development were examined. All participants were divided into two equal groups: Group I (n = 45; 50%) — children with delayed speech development (general speech underdevelopment, level II) associated with attention deficit hyperactivity disorder (ADHD). Group II (n = 45; 50%) — children with delayed speech development (general speech underdevelopment, level II) due to residual-organic brain lesions (ROL).A control group of 15 children without any speech impairments was also included, matched for age and sex.
4. Results
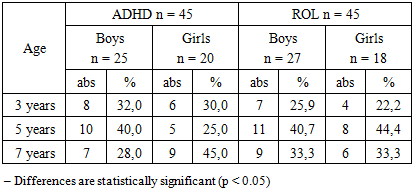
- To clarify the age and gender composition of the examined children, the distribution of both clinical groups by age and sex was analyzed (Table 1). The obtained data allow assessment of the age periods in which speech delay occurs most frequently and whether differences exist between the ADHD and ROL groups.
|
|

5. Discussion
- Children with delayed speech development associated with attention deficit hyperactivity disorder exhibit a significantly higher speech development coefficient (mean 24.9 ± 3.9) compared to those with residual-organic brain lesions (17.7 ± 6.7), suggesting a more favorable functional prognosis in functional forms of DSD. Children with organic brain lesions display more pronounced neurological and cognitive impairments, indicating delayed maturation and reduced functional activity of cortical structures. Early diagnosis and timely correctional interventions substantially improve rehabilitation outcomes and prevent the formation of persistent speech and cognitive disorders.
6. Conclusions
- The study established that the clinical and neurological profile of delayed speech development in children is largely determined by the underlying etiology. Children with DSD associated with attention deficit hyperactivity disorder (ADHD) demonstrated relatively mild neurological symptoms and higher speech development coefficients, which indicates a functional and reversible nature of their disorder. In contrast, children with residual-organic brain lesions (ROL) exhibited more profound neurological and cognitive impairments, reflecting structural brain dysfunction and delayed cortical maturation.
ACKNOWLEDGEMENTS
- The author expresses sincere gratitude to the staff of the Department of Neurology, Pediatric Neurology and Medical Genetics of the Tashkent State Medical University for their valuable guidance, constructive advice, and assistance during the research process. Special thanks are extended to the participating children and their parents for their cooperation and trust, which made this study possible. The author also appreciates the contribution of colleagues from the university clinic for their help in clinical observations and laboratory diagnostics.