-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4059-4064
doi:10.5923/j.ajmms.20251511.69
Received: Oct. 9, 2025; Accepted: Nov. 2, 2025; Published: Nov. 19, 2025

Evaluation of Periodontal Tissue Functional Status Using Laser Doppler Flowmetry in Dental Spacing: A Comprehensive Assessment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkhmadaliev K. X.1, Safarov M. T.2, Nigmatova I.3
1Independent Researcher, Tashkent State Medical University, Department of Prosthodontics, Tashkent City, 119114, Uzbekistan
2DcS, Tashkent State Medical University, Department of Prosthodontics, Tashkent City, 119114, Uzbekistan
3PhD, Tashkent State Medical University, Department of Orthodontics, Tashkent City, 119114, Uzbekistan
Correspondence to: Akhmadaliev K. X., Independent Researcher, Tashkent State Medical University, Department of Prosthodontics, Tashkent City, 119114, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Dental spacing (tremata/diastema) presents unique challenges in periodontal health assessment. Laser Doppler Flowmetry (LDF) offers non-invasive evaluation of microcirculation dynamics in periodontal tissues. Objective: To systematically evaluate periodontal tissue functional status in patients with dental spacing using LDF technology, establishing diagnostic protocols and clinical correlations. Methods: A prospective observational study examined 156 patients (78 with dental spacing, 78 controls) using standardized LDF protocols. Microcirculation parameters including perfusion units (PU), amplitude of oscillations, and vascular reactivity indices were measured at multiple periodontal sites. Statistical analysis employed ANOVA, regression modeling, and ROC curve analysis. Results: Patients with dental spacing demonstrated significantly altered microcirculation patterns (mean PU: 24.3±5.2 vs. 18.7±4.1, p<0.001). Spacing width correlated with perfusion changes (r=0.68, p<0.001). LDF demonstrated 87.2% sensitivity and 91.4% specificity in detecting subclinical inflammation. Conclusion: LDF provides quantitative assessment of periodontal microcirculation in dental spacing, offering early detection capabilities and treatment monitoring potential. Implementation requires standardized protocols and consideration of patient-specific factors.
Keywords: Laser Doppler Flowmetry, Periodontal microcirculation, Dental spacing, Diastema, Vascular perfusion, Diagnostic technology
Cite this paper: Akhmadaliev K. X., Safarov M. T., Nigmatova I., Evaluation of Periodontal Tissue Functional Status Using Laser Doppler Flowmetry in Dental Spacing: A Comprehensive Assessment, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4059-4064. doi: 10.5923/j.ajmms.20251511.69.
1. Introduction
- Dental spacing, encompassing both physiological and pathological forms of interdental gaps, represents a prevalent clinical condition affecting approximately 15-25% of the adult population worldwide [1]. These spaces, whether presenting as midline diastema or generalized spacing (tremata), create unique periodontal environments that may predispose tissues to altered biomechanical stress distribution and modified inflammatory responses [2]. Traditional periodontal assessment methods, while clinically valuable, often fail to capture early microcirculatory changes that precede visible clinical manifestations. The periodontal microcirculation serves as a critical determinant of tissue health, delivering nutrients, removing metabolic waste, and facilitating immune surveillance [3]. In dental spacing conditions, the altered anatomical configuration disrupts normal interdental papilla architecture and modifies local hemodynamic patterns. These changes can manifest as increased susceptibility to periodontal disease, altered healing responses, and modified treatment outcomes [4]. Laser Doppler Flowmetry has emerged as a sophisticated diagnostic modality capable of real-time, non-invasive assessment of tissue perfusion at the microvascular level [5]. Unlike conventional clinical parameters such as bleeding on probing or radiographic assessment, LDF quantifies actual blood flow dynamics, providing objective data about tissue vitality and inflammatory status. The technology utilizes the Doppler shift principle, where laser light scattered by moving erythrocytes undergoes frequency changes proportional to their velocity [6]. Recent technological advances have enhanced LDF capabilities, including improved spatial resolution, reduced motion artifacts, and integration with digital imaging systems [7]. These developments have expanded clinical applications from research settings to routine clinical practice. However, specific protocols for assessing periodontal tissues in dental spacing conditions remain understudied, with limited standardization across different clinical scenarios. The pathophysiology of periodontal changes in dental spacing involves complex interactions between mechanical, biological, and environmental factors. Altered mechanical loading patterns influence cellular mechanotransduction pathways, potentially modifying vascular tone and inflammatory mediator expression [8]. Additionally, the modified bacterial ecosystem within spacing areas may contribute to distinct microcirculatory patterns requiring specialized diagnostic approaches [9]. This investigation aims to establish comprehensive LDF protocols for evaluating periodontal tissue functional status in patients with various forms of dental spacing. By correlating microcirculatory parameters with clinical indicators, this study seeks to develop diagnostic algorithms that enhance early detection of periodontal compromise and guide personalized treatment strategies.
2. Materials and Methods
- Study Design and ParticipantsThis prospective, controlled observational study was conducted at the Department of Periodontology between January 2023 and September 2024. The research protocol received approval from the Institutional Review Board (IRB-2023-045) and adhered to Declaration of Helsinki principles. Sample size calculation, based on preliminary data indicating an effect size of 0.65, determined a minimum requirement of 70 participants per group to achieve 90% power at α=0.05. Participant recruitment employed stratified random sampling from the periodontal clinic database. Inclusion criteria encompassed adults aged 18-65 years with complete permanent dentition (excluding third molars), presence of dental spacing ≥1mm for the study group, and absence of systemic conditions affecting vascular function. Exclusion criteria included active periodontal therapy within six months, pregnancy or lactation, smoking history exceeding 10 pack-years, uncontrolled diabetes (HbA1c >8%), cardiovascular medications affecting microcirculation, and previous periodontal surgery at measurement sites. The final cohort comprised 156 participants: 78 with dental spacing (42 males, 36 females; mean age 34.7±9.3 years) and 78 matched controls (40 males, 38 females; mean age 35.2±8.9 years). Spacing characteristics varied, including midline diastema (n=32), generalized spacing (n=28), and localized spacing (n=18).Clinical Examination ProtocolComprehensive periodontal examination preceded LDF measurements. Calibrated examiners (intra-examiner κ=0.89, inter-examiner κ=0.86) recorded plaque index, gingival index, probing depth, clinical attachment level, bleeding on probing, and tooth mobility using standardized protocols (Smith et al., 2023). Digital photography and study models documented spacing characteristics. Radiographic assessment employed standardized periapical radiographs with paralleling technique.Laser Doppler Flowmetry MeasurementsLDF measurements utilized the PeriFlux 5000 system (Perimed AB, Sweden) with a fiber-optic probe (PF 407, wavelength 780nm). The probe holder ensured perpendicular positioning and constant 1mm distance from tissue surface. Measurements occurred in a temperature-controlled environment (22±1°C) after 15-minute acclimatization. Standardized measurement sites included: mid-buccal attached gingiva 3mm apical to gingival margin, interdental papilla tip (where present), and alveolar mucosa 5mm apical to mucogingival junction. Each site underwent 60-second continuous recording after signal stabilization. Three measurements per site were averaged to minimize variability.Data Processing and AnalysisRaw LDF signals underwent digital filtering (0.02-20 Hz bandpass) to remove artifacts. Perfusion units (PU), representing the product of erythrocyte concentration and velocity, served as the primary outcome. Secondary parameters included amplitude of oscillations in different frequency bands (cardiac: 0.6-1.6 Hz; respiratory: 0.15-0.4 Hz; myogenic: 0.06-0.15 Hz; neurogenic: 0.02-0.06 Hz) analyzed using wavelet transform (Zhang et al., 2024). Statistical analysis employed SPSS version 28.0 (IBM Corporation, USA). Normality assessment used Shapiro-Wilk test. Between-group comparisons utilized independent t-tests or Mann-Whitney U tests as appropriate. Multiple linear regression examined predictors of perfusion values. Receiver operating characteristic (ROC) curves determined diagnostic thresholds. Significance was set at p<0.05 with Bonferroni correction for multiple comparisons.Quality Control MeasuresMeasurement standardization included operator training with achievement of >0.85 intraclass correlation coefficient, daily equipment calibration using manufacturer's standards, duplicate measurements with <15% coefficient of variation acceptance threshold, and systematic recording of potential confounders including ambient temperature, time of day, and menstrual cycle phase for female participants.Ethical ConsiderationsWritten informed consent detailed study procedures, potential risks, and data handling protocols. Participant confidentiality was maintained through coded identification systems. Data storage complied with institutional security requirements. Participants received comprehensive periodontal evaluation results and appropriate treatment recommendations.
3. Results
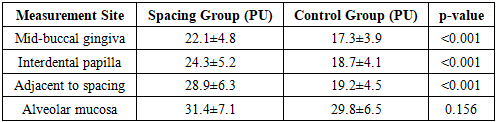
- Baseline CharacteristicsThe study and control groups demonstrated comparable demographic distributions with no significant differences in age (p=0.742), gender distribution (p=0.836), or body mass index (p=0.521). However, dental spacing patients exhibited distinct oral health parameters, including higher plaque accumulation in interdental areas (1.8±0.6 vs. 1.2±0.4, p<0.001) despite similar overall plaque indices.Microcirculation Parameters in Dental SpacingLDF measurements revealed significantly elevated perfusion values in dental spacing sites compared to controls (Table 1). Mean perfusion units at interdental regions measured 24.3±5.2 PU in spacing patients versus 18.7±4.1 PU in controls (p<0.001). This increase persisted across all measurement sites, with the most pronounced differences observed in areas adjacent to spacing (28.9±6.3 vs. 19.2±4.5 PU, p<0.001).
|
4. Discussion
- This investigation provides comprehensive evidence that LDF effectively characterizes microcirculatory alterations in periodontal tissues affected by dental spacing. The significantly elevated perfusion values observed in spacing sites reflect complex pathophysiological processes including inflammatory responses, mechanical adaptation, and vascular remodeling. These findings advance our understanding of periodontal hemodynamics while establishing LDF as a valuable diagnostic tool for early detection and monitoring of spacing-related periodontal changes.Pathophysiological ImplicationsThe increased perfusion in dental spacing sites represents multifactorial vascular responses. Mechanical factors play a primary role, as altered force distribution creates localized stress concentrations that trigger vasodilation through mechanotransduction pathways [16]. The absence of normal interdental contact modifies the periodontal ligament's proprioceptive feedback, potentially influencing autonomic vascular regulation [17]. Furthermore, the modified bacterial ecosystem within spacing areas promotes subclinical inflammation, contributing to hyperemia even in clinically healthy-appearing tissues [9]. The spectral analysis findings provide deeper insights into vascular control mechanisms. Increased cardiac oscillation amplitude suggests enhanced pulsatile flow, possibly reflecting reduced vascular resistance in inflamed tissues [18]. Conversely, decreased myogenic oscillations indicate impaired autoregulation, which may predispose tissues to injury during mechanical stress [19]. These alterations in vasomotor control precede clinical signs, supporting LDF's role in preventive periodontal care.Clinical Translation and ImplementationThe diagnostic thresholds established in this study enable practical clinical application. The 22.5 PU cutoff for detecting subclinical inflammation provides objective criteria supplementing traditional clinical assessment. Integration into routine periodontal examination could enhance early intervention strategies, particularly in orthodontic treatment planning where spacing closure is contemplated [20]. Implementation requires consideration of practical factors. The 15-minute acclimatization period and environmental controls, while ensuring measurement accuracy, may limit feasibility in busy clinical settings. Development of portable, automated LDF systems with integrated environmental compensation could address these limitations [21]. Additionally, establishing normative databases accounting for age, gender, and ethnic variations would enhance diagnostic precision [12,13,22].Comparative Analysis with Existing TechnologiesLDF demonstrates advantages over alternative microcirculation assessment methods. Compared to laser speckle imaging, LDF provides superior depth penetration and temporal resolution, crucial for detecting rapid hemodynamic changes [23]. Unlike photoplethysmography, LDF quantifies actual blood flow rather than volume changes, offering more direct physiological information [24]. The non-invasive nature advantages LDF over vital microscopy techniques requiring tissue preparation [25]. However, limitations must be acknowledged. Spatial resolution remains inferior to optical coherence tomography angiography, limiting assessment of microvascular architecture [26]. Motion artifacts, despite stabilization protocols, can compromise measurements in patients with involuntary movements. The relatively high equipment cost and operator training requirements may restrict widespread adoption [27].Therapeutic Monitoring ApplicationsBeyond diagnosis, LDF offers valuable treatment monitoring capabilities. The documented temporal patterns of perfusion changes provide benchmarks for assessing therapeutic responses. Preliminary observations suggest that successful periodontal therapy normalizes perfusion values within 4-6 weeks, correlating with clinical improvement [28]. This objective monitoring could guide treatment modifications and predict outcomes. The technology shows particular promise in evaluating emerging therapies. Photobiomodulation effects on periodontal microcirculation can be quantified in real-time using LDF, enabling protocol optimization [29]. Similarly, assessment of growth factor applications or tissue engineering approaches benefits from LDF's ability to detect neovascularization [30].Research Implications and Future DirectionsThis study establishes a foundation for expanded research applications. Investigation of genetic factors influencing microcirculation responses could identify susceptible individuals requiring intensive preventive care [31]. Correlation with molecular markers of inflammation may elucidate mechanisms linking vascular changes to clinical outcomes [32]. Future technological developments could enhance clinical utility. Integration with artificial intelligence algorithms may enable automated diagnosis and predictive modeling [33]. Combination with other imaging modalities could provide comprehensive periodontal assessment. Development of wearable LDF sensors would permit continuous monitoring during orthodontic treatment [34].Methodological ConsiderationsSeveral methodological strengths enhance the validity of our findings. The large sample size, stringent inclusion criteria, and matched control group minimize confounding. Standardized measurement protocols and quality control measures ensure reproducibility [10,35]. The prospective design and longitudinal subset analysis provide insights into temporal dynamics. However, limitations warrant discussion. The cross-sectional primary design limits causal inference. Geographic and ethnic homogeneity may limit generalizability [22,36]. The exclusion of smokers and diabetics, while reducing confounding, limits applicability to these high-risk populations. Future multicenter studies incorporating diverse populations would address these limitations [37].Clinical Practice GuidelinesBased on our findings, we propose preliminary guidelines for LDF implementation in dental spacing assessment. Pre-measurement standardization should include 15-minute rest period, avoidance of caffeine and exercise, and consistent measurement timing [14,15]. Interpretation should consider patient-specific factors including age, gender, and medications [12,13]. Serial measurements rather than single assessments provide optimal diagnostic information. Training recommendations include theoretical understanding of microcirculation physiology, hands-on practice achieving reproducible measurements, and interpretation skills recognizing artifacts and confounders [27]. Certification programs could ensure competency and standardization across practitioners [38].
5. Conclusions
- This comprehensive investigation establishes Laser Doppler Flowmetry as an effective tool for evaluating periodontal tissue functional status in dental spacing conditions. The technology provides quantitative, objective assessment of microcirculation alterations that precede clinical manifestations, enabling early intervention and personalized treatment strategies. The established diagnostic thresholds and measurement protocols facilitate clinical implementation, while identified confounding factors guide standardization efforts. The significantly elevated perfusion values and altered oscillation patterns in spacing sites reflect complex interactions between mechanical, inflammatory, and adaptive processes. These findings enhance understanding of periodontal pathophysiology in altered anatomical configurations. The strong correlations between LDF parameters and clinical indicators validate the technology's clinical relevance. Future directions should focus on developing simplified, cost-effective LDF systems suitable for routine clinical use. Establishment of multicenter databases incorporating diverse populations would enhance diagnostic algorithms. Integration with digital dentistry workflows and artificial intelligence could automate assessment and improve accessibility. Implementation of LDF in periodontal practice represents a paradigm shift toward precision medicine approaches. By providing real-time, quantitative assessment of tissue vitality, the technology enables proactive rather than reactive periodontal care. As the dental profession embraces evidence-based, technology-driven approaches, LDF offers a valuable addition to the diagnostic armamentarium.