Nurmurzayev Zafar Narbay ugli
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Nurmurzayev Zafar Narbay ugli, Samarkand State Medical University, Samarkand, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The results of comprehensive examination and treatment of 424 patients with benign obstructive jaundice (BOJ) who were treated at the multidisciplinary clinic of Samarkand State Medical University from 2015 to 2024 are presented. All patients were divided into two groups: the main group consisted of 296 patients (2020-2024) who underwent a differentiated approach taking into account the etiology of BOJ with staged treatment methods and priority use of minimally invasive technologies; the comparison group consisted of 128 patients (2016-2020) who underwent traditional diagnostic methods and single-stage radical surgical interventions. It was established that the use of modern radiological diagnostic methods, including ultrasound with Doppler imaging, magnetic resonance cholangiopancreatography, endoscopic retrograde cholangiopancreatography, and percutaneous transhepatic cholangiography, allows for highly accurate determination of the level and cause of biliary obstruction. Doppler studies of hepatic hemodynamics revealed a significant decrease in maximum portal vein blood flow velocity by 1.3 and 1.7 times in class B and C obstructive jaundice, respectively. The use of minimally invasive biliary drainage methods in the main group reduced the frequency of postoperative complications from 28.9% to 15.2% and mortality from 7.8% to 3.4%.
Keywords:
Obstructive jaundice, Hepatic insufficiency, Radiological diagnosis, Ultrasound examination, Magnetic resonance cholangiopancreatography, Endoscopic retrograde cholangiopancreatography, Percutaneous transhepatic cholangiography, Minimally invasive drainage, Biliary decompression, Hepatic Doppler imaging
Cite this paper: Nurmurzayev Zafar Narbay ugli, Diagnostic Role of Radiology in Obstructive Jaundice and Liver Dysfunction, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4020-4025. doi: 10.5923/j.ajmms.20251511.61.
1. Introduction
Obstructive jaundice remains one of the most relevant problems in modern surgery and radiology, representing a syndrome that develops due to impaired bile outflow through the biliary tract into the duodenum. The incidence of this pathology in the structure of surgical diseases of the abdominal organs ranges from 10 to 15%, with a steady increase in morbidity, especially among elderly and senile patients [1,2,3].The etiological structure of obstructive jaundice is characterized by a significant diversity of causes, among which cholelithiasis and its complications predominate (35-40%), malignant neoplasms of the pancreatobiliary zone (30-35%), bile duct strictures of various genesis (15-20%), as well as parasitic diseases and congenital anomalies of the biliary tract (5-10%). Benign causes of obstructive jaundice, despite a relatively favorable prognosis with timely diagnosis and adequate treatment, present significant difficulties in differential diagnosis and selection of optimal treatment tactics [4,5,6,7,8,9].The development of obstructive jaundice is accompanied by a cascade of pathophysiological changes leading to liver dysfunction, development of hepatic insufficiency, cholangitis, sepsis, and multiple organ failure. Hyperbilirubinemia has a toxic effect on all organs and systems of the body, causing disorders of hemostasis, immune status, kidney and cardiovascular system function. With prolonged biliary obstruction, irreversible changes develop in the liver parenchyma in the form of cholestatic hepatitis with outcome in biliary cirrhosis [10,11,12,13].Modern radiology has a wide range of diagnostic methods that allow highly accurate determination of the level and cause of biliary obstruction. Ultrasound examination remains the primary diagnostic method, having high sensitivity in detecting bile duct dilatation (95-98%) and determining the level of obstruction (85-90%). The use of Doppler imaging allows assessment of hepatic hemodynamic status and detection of early signs of portal hypertension [14,15,16].Magnetic resonance cholangiopancreatography is a non-invasive method of visualizing the biliary tract and pancreatic ducts, with a sensitivity of 95-97% and specificity of 98-99% in diagnosing the causes of biliary obstruction. The method allows obtaining three-dimensional images of the biliary tree without contrast agent administration, which is especially important in patients with severe hepatic insufficiency and hemostatic disorders [17,18,19,20].Endoscopic retrograde cholangiopancreatography and percutaneous transhepatic cholangiography are invasive diagnostic methods that in modern conditions are considered not only as diagnostic but also as therapeutic procedures. The ability to perform biliary decompression during diagnostic examination significantly improves the patient's condition and prepares them for radical surgical intervention [21,22].The development of minimally invasive biliary drainage technologies has opened new opportunities in the treatment of patients with obstructive jaundice. Endoscopic and percutaneous methods of biliary decompression allow rapid and effective resolution of jaundice, prevention of hepatic insufficiency development, and preparation of the patient for radical treatment under more favorable conditions. The use of a staged approach with initial biliary decompression and subsequent radical intervention significantly reduces the frequency of postoperative complications and mortality [23].Despite significant achievements in the diagnosis and treatment of obstructive jaundice, a number of unresolved issues remain regarding optimization of the diagnostic algorithm, determination of indications for various methods of biliary decompression, and selection of optimal timing for radical interventions. The influence of various drainage methods on the functional state of the liver and long-term treatment results requires further study [24,25].Aim of the study. To improve the results of diagnosis and treatment of patients with benign obstructive jaundice and hepatic insufficiency by optimizing the diagnostic algorithm using modern radiological diagnostic methods and implementing a differentiated approach to the selection of minimally invasive biliary drainage methods.
2. Materials and Methods
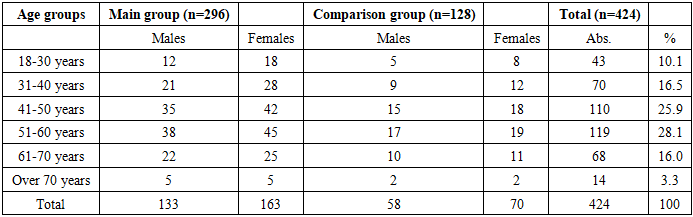
This work was performed at the Departments of Surgical Diseases and Radiology of Samarkand State Medical University based at the multidisciplinary clinic of SamSMU. The study is based on the results of comprehensive examination and treatment of 424 patients with benign obstructive jaundice who were in the clinic from 2015 to 2024.All patients with BOJ were divided into two groups. The first main group included 296 patients treated in 2020-2024, who underwent a differentiated approach taking into account the etiology of BOJ with staged treatment methods and priority use of minimally invasive technologies. The comparison group included 128 patients who underwent traditional research methods in diagnosis and treatment, as well as single-stage radical surgical interventions, treated in the period 2016-2020.Inclusion criteria for the study were: presence of clinical and laboratory signs of obstructive jaundice (jaundice of skin and sclera, increase in total bilirubin level above 20 μmol/L with predominance of direct fraction); benign nature of biliary obstruction confirmed by a complex of instrumental research methods and morphological verification; patient age from 18 to 85 years; informed consent of the patient to participate in the study.Exclusion criteria were: malignant neoplasms of the pancreatobiliary zone; terminal stage of hepatic insufficiency; decompensated comorbid pathology; patient refusal to participate in the study.Table 1. Distribution of patients by age and gender
 |
| |
|
The mean age of patients was 48.7±14.3 years in the main group and 49.2±13.8 years in the comparison group. Women predominated - 233 (55.0%) patients, men were 191 (45.0%). The largest number of patients was in the age group 51-60 years - 119 (28.1%) people.The etiological structure of benign obstructive jaundice was represented by the following diseases: choledocholithiasis - 178 (42.0%) patients; bile duct strictures of various genesis - 89 (21.0%); stenosis of the major duodenal papilla - 67 (15.8%); chronic pancreatitis with choledochal compression - 54 (12.7%); Mirizzi syndrome - 23 (5.4%); hepatic echinococcosis with rupture into bile ducts - 13 (3.1%) cases.All patients underwent comprehensive clinical-laboratory and instrumental examination. Laboratory research methods included complete blood count with determination of leukocyte formula, biochemical blood analysis with determination of total bilirubin level and its fractions, aminotransferases, alkaline phosphatase, gamma-glutamyl transpeptidase, total protein and its fractions, urea, creatinine, electrolytes, coagulation system parameters.Instrumental diagnostic methods in the main group included: ultrasound examination of abdominal organs with Doppler imaging of liver vessels - performed in all 296 (100%) patients; magnetic resonance cholangiopancreatography - 187 (63.2%) patients; computed tomography with intravenous contrast - 76 (25.7%) patients; endoscopic retrograde cholangiopancreatography - 142 (48.0%) patients; percutaneous transhepatic cholangiography - 76 (25.7%) patients.In the comparison group, the structure of instrumental diagnostic methods was as follows: ultrasound examination was performed in all 128 (100%) patients; computed tomography - 42 (32.8%) patients; endoscopic retrograde cholangiopancreatography - 38 (29.7%) patients; intraoperative cholangiography - 86 (67.2%) patients.Ultrasound examination was performed on expert-class devices using convex transducers with a frequency of 2.5-5.0 MHz in B-mode, color Doppler mapping mode, and pulse-wave Doppler imaging. The following were assessed: liver size, echogenicity and structure of parenchyma, diameter of intra- and extrahepatic bile ducts, presence of stones in the biliary tract, condition of the gallbladder, pancreas, presence of free fluid in the abdominal cavity.Doppler examination included assessment of diameter and blood flow velocity parameters in the portal vein, hepatic artery, and hepatic veins. The following parameters were determined: portal vein diameter, maximum (Vmax) and minimum (Vmin) blood flow velocity in the portal vein, peak systolic velocity (PSV) and end-diastolic velocity in the hepatic artery, resistance index, pulsatility index.Magnetic resonance cholangiopancreatography was performed on a tomograph with a magnetic field strength of 1.5 Tesla using specialized protocols for obtaining T2-weighted images with fat signal suppression. The examination was performed without contrast agent administration, which allowed it to be performed in patients with impaired renal function and allergic reactions to iodine-containing contrast agents.Endoscopic retrograde cholangiopancreatography was performed using side-viewing duodenoscopes under fluoroscopic control. After cannulation of the major duodenal papilla, water-soluble contrast agent was administered followed by assessment of the condition of bile ducts and pancreatic duct. When pathology was detected, therapeutic manipulations were performed: papillosphincterotomy, stone extraction, nasobiliary drainage, choledochal stenting.Percutaneous transhepatic cholangiography was performed under ultrasound and fluoroscopic control using 22G Chiba needles. After puncture of dilated intrahepatic ducts, contrast agent was administered with assessment of the biliary tree condition. When necessary, external or external-internal biliary drainage was performed.The severity of obstructive jaundice was assessed according to a classification that takes into account the level of total bilirubin and the presence of complications: class A (mild) - bilirubin level 20-60 μmol/L without signs of hepatic insufficiency; class B (moderate) - bilirubin level 60-200 μmol/L with initial manifestations of hepatic insufficiency; class C (severe) - bilirubin level above 200 μmol/L with pronounced manifestations of hepatic insufficiency and multiple organ dysfunction.Statistical processing of the obtained results was performed using SPSS Statistics 23.0 software package. For quantitative indicators, arithmetic mean (M), standard deviation (SD), median (Me), interquartile range (Q1-Q3) were calculated. For qualitative indicators, absolute and relative frequencies were determined. Comparison of quantitative indicators between groups was performed using the Mann-Whitney test, qualitative ones - using Pearson's chi-square test. Differences were considered statistically significant at p<0.05.
3. Results and Discussion
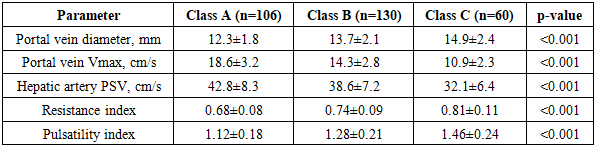
The use of modern radiological diagnostic methods in the main group significantly increased the accuracy of determining the level and cause of biliary obstruction. Ultrasound examination, performed in all patients at the first stage of diagnosis, revealed dilatation of intrahepatic bile ducts in 278 (93.9%) patients of the main group and 116 (90.6%) patients of the comparison group. Common bile duct dilatation greater than 8 mm was detected in 256 (86.5%) patients of the main group and 104 (81.3%) patients of the comparison group.Stones in the common bile duct lumen on ultrasound examination were visualized in 124 (41.9%) patients of the main group, which accounted for 69.7% of all cases of choledocholithiasis in this group. In the comparison group, stones in the common bile duct on ultrasound were detected in 38 (29.7%) patients, which accounted for 52.8% of all cases of choledocholithiasis in this group. The low sensitivity of ultrasound in detecting choledocholithiasis is due to difficulties in visualizing the distal parts of the common bile duct due to intestinal gas and small stone size.Doppler examination of hepatic hemodynamics revealed significant changes in portal and arterial blood flow parameters depending on the severity of obstructive jaundice. In patients with class A obstructive jaundice, the mean portal vein diameter was 12.3±1.8 mm, maximum blood flow velocity - 18.6±3.2 cm/s. In class B obstructive jaundice, there was an increase in portal vein diameter to 13.7±2.1 mm and a decrease in maximum blood flow velocity to 14.3±2.8 cm/s. In patients with class C obstructive jaundice, the portal vein diameter was 14.9±2.4 mm, and the maximum blood flow velocity decreased to 10.9±2.3 cm/s.Table 2. Hepatic hemodynamic parameters depending on the severity of obstructive jaundice
 |
| |
|
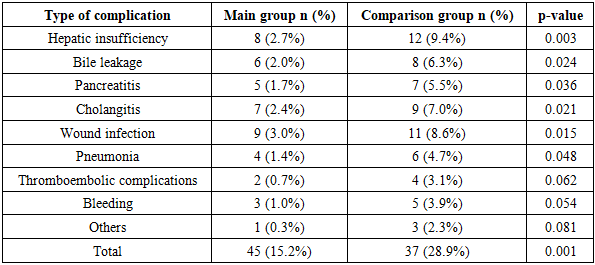
Thus, Doppler studies of hepatic hemodynamics revealed a significant decrease in maximum portal vein blood flow velocity by 1.3 and 1.7 times in class B and C obstructive jaundice, respectively, with an increase in vessel diameter. Peak systolic velocity of the hepatic artery with bilirubin levels above 100 μmol/L was 25% lower compared to patients with mild jaundice.Magnetic resonance cholangiopancreatography, performed in 187 (63.2%) patients of the main group, allowed highly accurate determination of the level and cause of biliary obstruction. The sensitivity of the method in detecting choledocholithiasis was 96.8%, specificity - 98.2%. MRCP detected stones in the common bile duct in all 118 patients with choledocholithiasis who underwent this examination, including small stones less than 3 mm in size that were not visualized on ultrasound.For bile duct strictures, MRCP allowed accurate determination of the location, extent, and degree of lumen narrowing. In 54 of 56 patients with strictures who underwent MRCP, it was possible to accurately determine the level and extent of the stricture, which allowed proper planning of the surgical intervention volume.Endoscopic retrograde cholangiopancreatography was performed in 142 (48.0%) patients of the main group and 38 (29.7%) patients of the comparison group. In the main group, ERCP was predominantly therapeutic in nature - in 126 (88.7%) patients, therapeutic manipulations were performed simultaneously with diagnosis. Papillosphincterotomy was performed in 98 patients, stone extraction in 72, nasobiliary drainage in 34, choledochal stenting in 18 patients.Percutaneous transhepatic cholangiography was performed in 76 (25.7%) patients of the main group in whom ERCP was impossible or ineffective. Indications for PTC were: high bile duct strictures - 42 patients; inability to cannulate the major duodenal papilla during ERCP - 18 patients; Mirizzi syndrome - 16 patients. In all patients, PTC was completed with biliary drainage: external drainage was performed in 48 patients, external-internal in 28 patients.The use of a differentiated approach to the selection of biliary decompression method in the main group allowed minimally invasive biliary drainage to be performed in 218 (73.6%) patients. Endoscopic decompression methods were used in 142 (48.0%) patients, percutaneous transhepatic in 76 (25.7%) patients. In the comparison group, minimally invasive decompression methods were used in only 38 (29.7%) patients.The effectiveness of biliary decompression was assessed by the dynamics of bilirubin level decrease, improvement of liver function parameters, and regression of clinical manifestations of jaundice. In patients of the main group after minimally invasive drainage, a more rapid decrease in bilirubin level was noted compared to patients who underwent open operations. The average rate of bilirubin decrease after endoscopic decompression was 28.4±6.2 μmol/L per day, after percutaneous drainage - 24.6±5.8 μmol/L per day, after open operations - 18.3±4.6 μmol/L per day.Normalization of bilirubin level (less than 20 μmol/L) in the main group was achieved on average after 7.2±2.3 days after minimally invasive drainage and after 11.4±3.6 days after open operations. In the comparison group, bilirubin normalization occurred on average after 14.2±4.8 days.Radical surgical interventions in the main group were performed predominantly in a delayed manner after resolution of jaundice and stabilization of the patient's condition. A staged approach was used in 186 (62.8%) patients of the main group. The average interval between biliary decompression and radical operation was 12.4±4.6 days. In the comparison group, single-stage radical operations at the height of jaundice were performed in 90 (70.3%) patients.The structure of radical surgical interventions in the main group was as follows: cholecystectomy with choledocholithotomy - 68 patients; cholecystectomy with biliodigestive anastomosis - 42 patients; transduodenal papillosphincteroplasty - 28 patients; choledochal resection with hepaticojejunostomy - 18 patients; Frey operation for chronic pancreatitis - 12 patients; echinococcectomy with biliary tract sanation - 8 patients.In the comparison group, the structure of surgical interventions included: cholecystectomy with choledocholithotomy - 48 patients; cholecystectomy with biliodigestive anastomosis - 24 patients; transduodenal papillosphincteroplasty - 12 patients; choledochal resection - 8 patients; Frey operation - 6 patients; echinococcectomy - 5 patients.Laparoscopic and laparoscopically assisted interventions in the main group were performed in 84 (28.4%) patients, in the comparison group - 12 (9.4%) patients. The use of minimally invasive technologies at all stages of treatment significantly reduced the trauma of interventions and accelerated patient rehabilitation.Analysis of postoperative complications showed a significant reduction in their frequency in the main group compared to the comparison group. The overall complication rate in the main group was 15.2% (45 patients), in the comparison group - 28.9% (37 patients).Table 3. Structure of postoperative complications
 |
| |
|
The most significant was the reduction in the frequency of hepatic insufficiency - from 9.4% in the comparison group to 2.7% in the main group (p=0.003). This is due to the use of a staged approach with preliminary biliary decompression and performance of radical operations after stabilization of liver function.Mortality in the main group was 3.4% (10 patients), in the comparison group - 7.8% (10 patients). The main causes of fatal outcomes were: progressive hepatic insufficiency - 8 cases; pulmonary embolism - 4 cases; acute myocardial infarction - 3 cases; multiple organ failure against the background of sepsis - 5 cases.The average duration of hospitalization in the main group was 12.8±4.2 days, in the comparison group - 21.3±6.7 days (p<0.001). The reduction in hospitalization time in the main group is due to the use of minimally invasive technologies, reduction in the frequency of complications, and faster patient rehabilitation.Long-term treatment results were traced in 234 (79.1%) patients of the main group and 86 (67.2%) patients of the comparison group at terms from 6 months to 5 years. Good results (complete recovery, absence of disease recurrences) were noted in 190 (81.2%) patients of the main group and 56 (65.1%) patients of the comparison group. Satisfactory results (presence of periodic pain, dyspeptic disorders not requiring hospital treatment) were identified in 38 (16.2%) patients of the main group and 22 (25.6%) patients of the comparison group. Unsatisfactory results (disease recurrence, need for repeated operations) were noted in 6 (2.6%) patients of the main group and 8 (9.3%) patients of the comparison group.Recurrence of choledocholithiasis in the long-term period developed in 4 patients of the main group and 6 patients of the comparison group. Restenosis in the biliodigestive anastomosis area required repeated intervention in 2 patients of the main group and 2 patients of the comparison group. All repeated interventions in the main group were performed using minimally invasive technologies.Quality of life of patients was assessed using the SF-36 questionnaire. Six months after treatment, physical functioning indicators in the main group were 78.4±12.3 points, in the comparison group - 68.2±14.7 points (p<0.01). Mental health indicators were 74.6±11.8 and 65.3±13.2 points, respectively (p<0.01).The economic effectiveness of using the developed diagnostic and treatment algorithm was expressed in reducing hospitalization time, reducing costs for treating complications, and reducing temporary disability periods. The average cost of treating one patient in the main group was 28.4% lower than in the comparison group, with significantly better clinical results.Thus, the use of modern radiological diagnostic methods in combination with a differentiated approach to the selection of minimally invasive biliary drainage methods significantly improves the treatment results of patients with benign obstructive jaundice. The use of MRCP as the main non-invasive method of biliary tree visualization allows highly accurate determination of the level and cause of obstruction, ensuring the correct choice of treatment tactics.Doppler assessment of hepatic hemodynamics is an important additional method that allows objective assessment of the degree of liver dysfunction and prediction of the risk of developing hepatic insufficiency. The identified correlation between the degree of hyperbilirubinemia and decreased portal blood flow can be used to determine the optimal timing of radical interventions.The use of a staged approach with initial minimally invasive biliary decompression and subsequent radical intervention under conditions of resolved jaundice reduces the frequency of postoperative complications by almost half and mortality by more than half. Endoscopic decompression methods are the method of choice for distal obstruction, while percutaneous transhepatic interventions are indicated for proximal strictures and when endoscopic decompression is impossible.
4. Conclusions
1. Diagnosis of benign obstructive jaundice should be comprehensive using the developed diagnostic algorithm, including modern non-invasive radiological methods (ultrasound, MRCP) of diagnosis, as well as invasive puncture and endoscopic (ERCP, PTC) methods with transition to biliary decompression, which was performed in 73.64% of patients in the main group.2. Doppler studies of hepatic hemodynamics revealed a significant decrease in maximum portal vein blood flow velocity by 1.3 and 1.7 times in class B and C obstructive jaundice, respectively, with an increase in vessel diameter. Peak systolic velocity of the hepatic artery with bilirubin levels above 100 mmol/L was 25% lower.3. Magnetic resonance cholangiopancreatography has high sensitivity (96.8%) and specificity (98.2%) in diagnosing the causes of obstructive jaundice and should be considered as the method of choice for non-invasive visualization of the biliary tree in patients with obstructive jaundice.4. The use of a differentiated approach to the selection of biliary decompression method, taking into account the level and cause of obstruction, allows minimally invasive biliary drainage to be performed in 73.6% of patients, ensuring more rapid normalization of liver function parameters.5. A staged approach to treatment with initial biliary decompression and performance of radical operations after resolution of jaundice reduces the frequency of postoperative complications from 28.9% to 15.2% and mortality from 7.8% to 3.4%.6. Comprehensive use of modern radiological diagnostic methods and minimally invasive biliary drainage technologies provides good long-term treatment results in 81.2% of patients and significant improvement in quality of life.
References
| [1] | Alperovich B.I., Tskhai V.F., Khabas G.N. Obstructive jaundice: diagnosis and treatment. Tomsk: Red Banner, 2016. 312 p. |
| [2] | Borisov A.E., Zemlyanoy V.P., Nepomnyashchaya S.L. et al. Endobiliary interventions in the treatment of obstructive jaundice. St. Petersburg: Aesculapius, 2018. 286 p. |
| [3] | Vinnik Yu.S., Pakhomova R.A., Kochetova L.V. Benign obstructive jaundice: pathogenesis, diagnosis, treatment. Novosibirsk: Science, 2019. 168 p. |
| [4] | Galperin E.I., Vetshev P.S. Guide to biliary surgery. Moscow: Vidar-M, 2020. 568 p. |
| [5] | Dadvani S.A., Vetshev P.S., Shulutko A.M., Prudkov M.I. Cholelithiasis. Moscow: Vidar-M, 2017. 144 p. |
| [6] | Ermolov A.S., Upyrev A.V., Ivanov P.A. Surgery of cholelithiasis: from traditions to minimally invasive technologies. Surgery. N.I. Pirogov Journal. 2018; (4): 92-107. |
| [7] | Zatevakhin I.I., Tsitsiashvili M.Sh., Budurova M.D. Obstructive jaundice: diagnostic algorithm and treatment. Annals of Surgical Hepatology. 2019; 24(4): 88-95. |
| [8] | Kubyshkin V.A., Vishnevsky V.A. Pancreatic cancer. Moscow: Medpraktika-M, 2017. 328 p. |
| [9] | Leuschner U. Practical guide to biliary diseases. Moscow: GEOTAR-Media, 2018. 264 p. |
| [10] | Maistrenko N.A., Stukalov V.V. Choledocholithiasis. St. Petersburg: ELBI-SPb, 2020. 288 p. |
| [11] | Nazyrov F.G., Akbarov M.M., Ikramov A.I. et al. Diagnosis and treatment of benign obstructive jaundice syndrome. Annals of Surgical Hepatology. 2018; 23(3): 84-91. |
| [12] | Okhotnikov O.I., Grigoriev S.N., Yakovleva M.V. Percutaneous transhepatic endobiliary interventions in obstructive jaundice. Annals of Surgical Hepatology. 2019; 24(2): 89-95. |
| [13] | Prudkov M.I., Natroshvili A.G., Shulutko A.M. Minimally invasive surgery of choledocholithiasis. Ekaterinburg: Ural Worker, 2019. 112 p. |
| [14] | Savelyev V.S., Petukhov V.A. Gallbladder cholesterosis. Moscow: VEDI, 2018. 192 p. |
| [15] | Timoshin A.D., Shestakov A.L., Yurasov A.V. Minimally invasive interventions in abdominal surgery. Moscow: Triada-X, 2017. 216 p. |
| [16] | Fedorov I.V., Slavin L.E., Chugunov A.N. Endoscopic surgery. Moscow: GEOTAR-Media, 2020. 352 p. |
| [17] | Shapovalyants S.G., Ardasenov T.B., Freidovich D.A. et al. Problems of modern diagnosis of choledocholithiasis. Russian Journal of Gastroenterology, Hepatology, Coloproctology. 2019; 21(2): 5-10. |
| [18] | Baron T.H., Kozarek R., Carr-Locke D.L. ERCP. Philadelphia: Elsevier Saunders, 2018. 512 p. |
| [19] | Barkun A.N., Barkun J.S., Fried G.M. et al. Useful predictors of bile duct stones in patients undergoing laparoscopic cholecystectomy. Ann Surg. 2018; 220(1): 32-39. |
| [20] | Beebe D.S., McNevin M.P., Belani K.G. et al. Evidence of venous stasis after abdominal insufflation for laparoscopic cholecystectomy. Surg Gynecol Obstet. 2019; 176: 443-447. |
| [21] | Bergman J.J., van Berkel A.M., Groen A.K. et al. Biliary manometry, bacterial characteristics, bile composition and histological changes fifteen to seventeen years after endoscopic sphincterotomy. Gastrointest Endosc. 2017; 45: 400-405. |
| [22] | Cotton P.B., Lehman G., Vennes J. et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc. 2018; 37: 383-393. |
| [23] | Cuschieri A., Lezoche E., Morino M. et al. EAES multicenter prospective randomized trial comparing two-stage vs single-stage management of patients with gallstone disease and ductal calculi. Surg Endosc. 2019; 13: 952-957. |
| [24] | De Palma G.D., Galloro G., Siciliano S. et al. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc. 2018; 53: 547-553. |
| [25] | Freeman M.L., Nelson D.B., Sherman S. et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med. 2017; 335: 909-918. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML