-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4009-4012
doi:10.5923/j.ajmms.20251511.58
Received: Oct. 11, 2025; Accepted: Nov. 8, 2025; Published: Nov. 17, 2025

Low-Flow Inhalation Anesthesia in Abdominal Surgery in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMamatkulov I. A., Yusupov A. S., Khakimov A. B., Turaev M. Z., Matyakubov U. Yu.
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In this article, the effectiveness and safety of low-flow inhalation anesthesia (LFA) in pediatric abdominal surgery are evaluated. The study included 42 children undergoing surgical treatment for Hirschsprung’s disease. Patients were divided into two groups: Group 1 received sevoflurane in combination with fentanyl, while Group 2 underwent anesthesia with propofol and fentanyl. Central hemodynamic parameters, including heart rate (HR), stroke index (SI), cardiac index (CI), ejection fraction (EF), and total peripheral vascular resistance (TPVR), were monitored throughout anesthesia. The findings demonstrated that sevoflurane-based LFA ensured stable hemodynamics, smooth induction and emergence from anesthesia, and the absence of significant intra- or postoperative complications. Patients in Group 1 exhibited calm awakening without agitation, vomiting, or respiratory disorders, which facilitated early extubation. Moderate circulatory hypodynamia observed during anesthesia was effectively corrected by infusion therapy. Thus, low-flow inhalation anesthesia with sevoflurane combined with fentanyl provides reliable anesthetic protection, reduces anesthetic consumption, and is safe and effective for pediatric abdominal surgical procedures.
Keywords: Anesthesia in children, Inhalation anesthetics, Sevoflurane, Fentanyl, Central hemodynamic parameters
Cite this paper: Mamatkulov I. A., Yusupov A. S., Khakimov A. B., Turaev M. Z., Matyakubov U. Yu., Low-Flow Inhalation Anesthesia in Abdominal Surgery in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4009-4012. doi: 10.5923/j.ajmms.20251511.58.
1. Introduction
- Inhalation methods of anesthesia, which stood at the origins of anesthesiology, today occupy a worthy place in the concept of modern multicomponent anesthesia. The advantages of inhalation anesthesia (IA) include the rarity of anaphylactoid reactions, the predictability of pharmacokinetics and pharmacodynamics, and a low risk of intraoperative awakening of the patient [1,3].The traditional method of IA involves supplying a large gas flow into the anesthesia circuit with a calculated and fixed ratio of gas mixture components. As a result, a large amount of unused anesthetic and medical gases is lost; moreover, unfavorable conditions are created for humidification and warming of the respiratory mixture, and excessive pollution of the environment occurs. All this makes anesthesiologists think about measures to possibly reduce the flow of fresh gas. Repeated attempts in the past to use low flows of inhalation anesthetics, however, did not lead to the widespread adoption of the low-flow anesthesia method [2,4,6]. The main reasons for this were an insufficient level of patient safety and the complexity of anesthesia management techniques.The recent development of modern medical equipment — the introduction into practice of “new generation” anesthesia and respiratory apparatuses and the expansion of multifunctional monitoring systems — makes it possible to implement effective and safe use of low-flow anesthesia (LFA), including in pediatric anesthesiology. The appearance on the commercial market of new inhalation anesthetics (sevoflurane, isoflurane, desflurane), which are characterized by low solubility in blood, low consumption, and relative costliness (therefore, their use in a circuit with high gas flow is impractical), stimulates the development of low-flow anesthesia methods [5,7,9]. The possibility of maintaining optimal temperature and humidity in the breathing circuit, significant reduction in anesthetic consumption, and hygienic and environmental safety — all these factors determine the considerable interest of anesthesiologists in LFA [8,10]. However, the experience of using this anesthesia method in pediatric anesthesiology is extremely limited and requires further study. Unlike traditional anesthesia performed in a non-rebreathing circuit with a gas flow exceeding the minute ventilation of the lungs, in low-flow anesthesia the fresh gas flow is reduced to 1 L/min or less. A variant of low-flow anesthesia is minimal flow anesthesia, with a fresh gas flow equal to 1 L/min [11,12]. In this regard, the purpose of our study is to evaluate the effectiveness and safety of the low-flow inhalation anesthesia method using sevoflurane or isoflurane in children, based on the study of oxygen transport parameters during abdominal surgeries in children.Purpose of the study: To improve the quality of anesthetic protection by using low-flow inhalation anesthesia with sevoflurane in combination with fentanyl during abdominal surgeries in children.
2. Materials and Methods
- To provide anesthetic protection in 42 pediatric patients undergoing abdominal surgery for Hirschsprung’s disease, the following combinations were used: fentanyl with sevoflurane — Group 1 (22 patients, 52%), and fentanyl with propofol — Group 2 (20 patients, 48%).Children aged 1–2 years accounted for 56.4%, 3–6 years — 25.2%, and 6–9 years — 18.4% of the total number of patients. Anesthesia was performed during abdominal surgeries. The duration of anesthesia in 62.8% of patients was up to 1 hour 50 minutes, and in 37.2% — up to 2 hours 25 minutes. In Group 1, after premedication, inhalation with sevoflurane up to 3.0 vol% was carried out, followed by intravenous administration of fentanyl solution at a dose of 5 μg/kg.In Group 2, induction began with intravenous administration of propofol at a dose of 4 mg/kg, along with intravenous fentanyl at a dose of 5 μg/kg.In both groups, tracheal intubation was performed under the administration of arduan at a dose of 0.006 mg/kg. Mechanical ventilation was performed using a Dräger “Fabius Plus” (Germany) apparatus in a semi-closed circuit. Muscle relaxation was maintained by administering one-third of the initial dose of arduan. Maintenance of anesthesia was achieved by repeated administration of fentanyl at doses corresponding to 50% or 25% of the initial dose. In the first group, anesthesia was maintained with inhalation of sevoflurane at a concentration of 1.0–1.5 vol% and repeated fractional administration of fentanyl (50% or 25% of the initial dose). In the second group, anesthesia was maintained by intravenous infusion of propofol at a dose of 4 mg/kg and repeated fractional administration of fentanyl (50% or 25% of the initial dose). Infusion therapy was carried out at a rate of 10–15 ml/kg/hour. After completion of the operation, the patient was transferred to the intensive care unit. Hemodynamic parameters were measured using a “SonoScape” echocardiograph (China) with a 3.5 MHz sensor according to the standard protocol. To assess the functional state of the cardiovascular system during anesthesia, the following parameters were studied: stroke index (SI), cardiac index (CI), and total peripheral vascular resistance (TPVR).The stroke index (ml/m²) = stroke volume / body surface area.The cardiac index (L/min/m²) = cardiac output / body surface area.Total peripheral vascular resistance = systolic arterial pressure / cardiac index.The ejection fraction (EF) of the left ventricle (LV) is an integral measure of myocardial contractility, characterizing the proportion of blood ejected by the LV relative to its diastolic volume. The results of clinical and functional studies were processed using variation statistics and Student’s t-test.
3. Results and Discussion
- The results of the hemodynamic parameter analysis in children of Group I (fentanyl + sevoflurane) are presented in Figure 1.
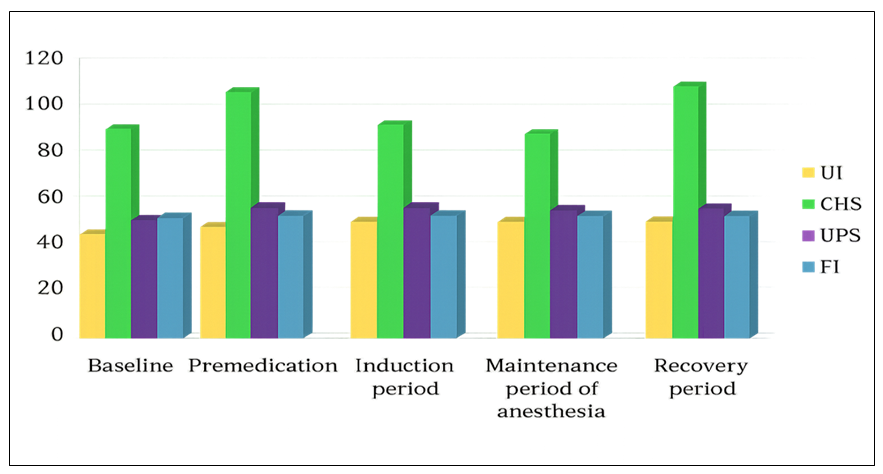 | Figure 1. Hemodynamic parameters during combined anesthesia using fentanyl and sevoflurane |
4. Conclusions
- Low-flow inhalation anesthesia with sevoflurane in combination with fentanyl provides optimal conditions for surgical correction, minimizes the negative effects of its individual components, and effectively fulfills the specific objectives of anesthetic management during abdominal surgical operations in children.