-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 4000-4003
doi:10.5923/j.ajmms.20251511.56
Received: Oct. 25, 2025; Accepted: Nov. 12, 2025; Published: Nov. 17, 2025

Clinical and Laboratory Assessment of Oral Mucosal Leukoplakia Associated with Cardiovascular Pathology and Optimization of Therapeutic Strategies
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIdiev Gayrat Elmurodovich1, Babayeva Nigora Mukhitdinovna2
1Associate Professor, Department of Orthopedic Dentistry and Orthodontics, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Assistant, Department of Hygiene No. 1, Bukhara State Medical Institute, Bukhara, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents the results of a comprehensive clinical and laboratory study of patients with oral mucosal leukoplakia occurring in the presence of cardiovascular diseases. A total of 120 patients were examined and categorized according to the clinical form and severity of leukoplakia. The study assessed the oral hygiene index, Schiller–Pisarev test, and hydrogen peroxide resistance to evaluate epithelial changes and inflammatory response. Modern treatment modalities, including ozone therapy and photodynamic therapy, were compared with conventional treatment regimens. The use of combined modern approaches led to a 25–30% improvement in epithelial regeneration, reduction of inflammatory signs, and normalization of mucosal biochemistry. The results emphasize the need for an integrated diagnostic protocol and pathogenetically based treatment methods to increase therapeutic efficiency in patients with leukoplakia on the background of cardiovascular pathology.
Keywords: Oral leukoplakia, Cardiovascular pathology, Oral mucosa, Epithelial regeneration, Schiller–Pisarev test, Hydrogen peroxide test, Ozone therapy, Photodynamic therapy
Cite this paper: Idiev Gayrat Elmurodovich, Babayeva Nigora Mukhitdinovna, Clinical and Laboratory Assessment of Oral Mucosal Leukoplakia Associated with Cardiovascular Pathology and Optimization of Therapeutic Strategies, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 4000-4003. doi: 10.5923/j.ajmms.20251511.56.
Article Outline
1. Introduction
- Leukoplakia of the oral mucosa is a common disease in medicine, occurring mainly in patients over 30 years of age. This disease is accompanied by the development of pathological hyperkeratosis in the oral mucosa and, if not diagnosed in time or treated inadequately, has a high risk of malignant transformation [1,2,3,4,5,6,7,8]. According to epidemiological studies, the incidence of leukoplakia in the general population is about 1-3%, but among risk groups (smokers, alcohol drinkers) this figure has been found to increase to 6-7%. The variety of clinical forms of the disease (flat, verrucous, erosive-ulcerative), as well as in more severe cases, complicates the treatment tactics [9,10,11,12].Leukoplakia diagnosis is based on clinical examination, laboratory and instrumental examinations. In addition to traditional approaches (vitamin A preparations, treatment with medicinal oils), modern methods are widely used in treatment - ozone therapy, photodynamic therapy, physiotherapeutic procedures. Therefore, the purpose of this study is to compare the clinical and laboratory effectiveness of various treatment approaches in leucoplakia [13,14,15].
2. Materials and Methods
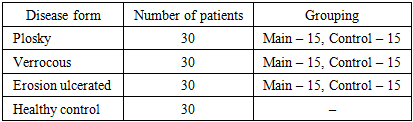
- The study was conducted in 2021–2024 with the participation of 120 patients. All patients were aged 30 to 60 years, and they were divided into groups according to gender, age, smoking and duration of alcohol consumption. Individuals with general somatic diseases and allergic reactions were excluded from the study.Patients were divided into 3 main groups and 6 subgroups:1. The first group consisted of 30 patients with flat leukoplakia. 15 of them received ozone therapy (general and local), and the remaining 15 were treated with healing oil and vitamin A.2. The second group consisted of 30 patients with varicose veins. 15 of them received general and local ozone therapy after the treatment process, and 15 were treated only with traditional means.3. The third group consisted of 30 patients with severe forms (varicose and erosive-ulcerative). 15 of them received photodynamic therapy, and the remaining 15 received only traditional treatments.Thirty healthy individuals were recruited as controls. During the study, clinical examination, oral hygiene indices, Schiller-Pisarev test, perhydrol test, as well as microscopic and immunological parameters were studied.
3. Research Results
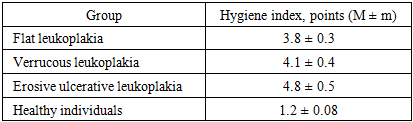
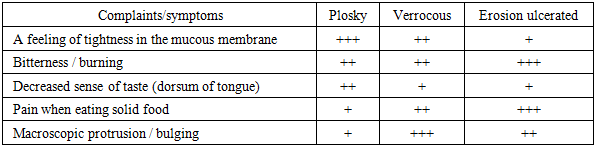
- The program of work with patients was designed in stages: first, oral hygiene and the general condition of the mucous membrane were examined, then the Schiller–Pisarev and perhydrol tests were used to assess the degree of inflammation, and then the treatment (traditional or modern) appropriate to the clinical form was selected. Intergroup comparisons were performed while maintaining the proportion of age, gender and harmful habits (smoking, alcohol). During the observation period, all patients were given hygienic education, as well as recommendations to reduce factors that increase inflammation. The results are presented in detail below.
|
|
|
|
|
4. Discussion
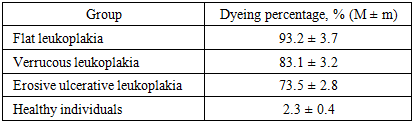
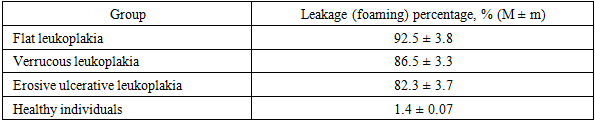
- In this study, the functional state of the mucous membrane and inflammatory markers in the forms of oral leukoplakia (flat, verrucous, erosive-ulcerative) were analyzed in a comprehensive manner. The results showed a sharp deterioration in hygiene indicators in all forms and a high positive response to tests (Schiller–Pisarev, perhydrol). This is explained, on the one hand, by the intensification of hyperkeratosis and parakeratosis, and, on the other hand, by the accumulation of microtraumas at the epithelial- connective tissue interface. If the high staining in the flat form indicates that the epithelial layer is preserved, but has undergone metaplasia, then in the erosive-ulcerative form the test percentage decreases due to the disruption of the epithelium - this indicates not a decrease in inflammation, but the loss of the protective layer.The parallel upward trend observed between the hygienic index and functional tests dictates the sequence of interventions: first, professional cleaning and home hygiene retraining, then inflammation control (antiseptic rinses, barrier gels/ointments), and then form-specific treatments (relief smoothing and stimulation of re-epithelialization in varicose veins, epithelialization and pain control in erosive ulcers) are appropriate.Modern approaches – ozone therapy and photodynamic therapy – seem promising in clinical practice. Ozone therapy can reduce symptoms more quickly by normalizing local redox balance, disrupting biofilms, and improving microcirculation; photodynamic therapy helps control pathological foci through selective photoinduced cytotoxicity. As a practical recommendation, these methods are expected to provide broader clinical benefits compared to small protocols limited to traditional oils and vitamins, especially in varicose and erosive ulcerative forms.However, several limitations of the study design should be acknowledged: (i) the fact that histological dynamic follow-up was not performed to the same depth in all cases limits long-term conclusions regarding the risk of malignant transformation; (ii) the use of a semiquantitative scale of clinical complaints is less sensitive than a precise percentage assessment; (iii) the final results cannot be guaranteed to be completely independent of lifestyle factors (smoking intensity, alcohol consumption frequency). Future studies with a multicenter, larger sample size, and enriched with complete histomorphological monitoring will further clarify the results.The lessons for clinical practice are summarized as follows: in the initial evaluation of a patient presenting with leukoplakia, measuring the hygiene index and performing two function tests provides sufficient information as a “quick filter” for diagnosis; the differential diagnosis of the form is consistent with the complaint pattern; and treatment should begin with hygiene and inflammation management, followed by form-specific modalities.
5. Conclusions
- This study showed that in the forms of oral leukoplakia, hygiene disorders and inflammatory markers increased sharply, and the high positivity of the Schiller-Pisarev and perhydrol tests paralleled the clinical severity; in the flat form, the high staining intensity reflected the background of metaplastic epithelium, and in the erosive lesions, a relative decrease due to the disruption of the protective layer; at the same time, in the verrucous form, a rough change in the relief had a dominant effect on the clinical picture. In practice, initially re-education of patients in professional and home hygiene, the introduction of complex anti-inflammatory measures, and then the use of modern treatments (ozone therapy, photodynamic therapy) appropriate to the form can accelerate the regression of symptoms and restore the stability of the mucosa. In the future, it is desirable to further refine treatment algorithms through multicenter and long-term follow-up, histological monitoring, and strict control of lifestyle factors.