Kamalova M. K.1, Rakhimov S. Sh.2
1DSc., Associate Professor, Department of Surgical Dentistry, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Department of Dentistry, Bukhara Regional Children's Multidisciplinary Medical Center, Bukhara University of Innovative Education and Medicine, Bukhara, Uzbekistan
Correspondence to: Kamalova M. K., DSc., Associate Professor, Department of Surgical Dentistry, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article presents the results of a comprehensive clinical and microbiological study of 59 pediatric patients with secondary deformities of congenital cleft palate treated at the Department of Maxillofacial Surgery of the Bukhara State Medical Institute. The patients were divided into two groups depending on the applied treatment method: Group I – patients who underwent the modified surgical approach combining the techniques of L.E. Frolova and F. Braithwaite with the M.I. Azimov modification, followed by postoperative care using Chlorhexidine and magneto-infrared laser therapy; and Group II – patients who received traditional surgical correction and postoperative care with Furacilin and quartz-tube irradiation. The study analyzed the duration of hospitalization, the rate of postoperative inflammatory reactions, epithelialization period, pain and edema reduction, as well as oral and nasal cavity microbiological flora, PMA and OHI-S indices. Statistical analysis demonstrated significant improvement (p<0.01) in Group I, including faster wound healing, reduced inflammation, and restoration of normal physiological function of the soft palate and velopharyngeal ring. The number of infectious complications decreased, while the length of hospital stay was reduced by an average of 1.4 times compared to traditional management. The obtained results confirm that the use of a modified surgical technique combined with complex postoperative care is highly effective in reducing postoperative complications, improving anatomical and functional outcomes, and shortening the rehabilitation period in children with secondary deformities of congenital cleft palate.
Keywords:
Congenital cleft palate, Secondary deformities, Modified palatoplasty, Magneto-infrared laser therapy, Chlorhexidine, Oral microflora, Postoperative rehabilitation, Maxillofacial surgery
Cite this paper: Kamalova M. K., Rakhimov S. Sh., Results of Improving the Methodology of Comprehensive Diagnosis and Surgical Treatment of Children with Secondary Deformities of Congenital Cleft Palate, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3971-3979. doi: 10.5923/j.ajmms.20251511.51.
1. Introduction
Congenital maxillofacial defects, especially clefts in the palatal area, are one of the most common anomalies among children. These defects not only cause cosmetic defects in appearance, but also seriously affect the vital functions of the child, such as speech, breathing, eating, and swallowing [2,6]. According to the World Health Organization and international dental associations, congenital maxillofacial anomalies account for 12-30% of all congenital anomalies, of which 80-90% are anomalies associated with the upper lip and palate [7,13].These diseases have not only medical, but also social significance, since speech defects, appearance deformities, and psychoemotional complex conditions make it difficult for children to adapt socially. In such children, low self-confidence, a tendency towards isolation, and delayed speech development are often observed [8,9]. Therefore, achieving full functional recovery through early diagnosis and effective surgery of palate defects has become one of the priorities of world pediatric and dental practice.The frequency of births with clefts of the upper lip and palate varies in different regions: in Europe it is recorded in 1-1.5 cases per 1000 newborns, and in Asian countries - in 2-3 cases. In Uzbekistan, this indicator averages around 1:600, which is a serious clinical and social problem for the regional healthcare system [5,11].Although surgical methods for eliminating palate defects are being improved today, in practice, secondary deformities - i.e., post-operative asymmetrical structures, fistulas, and functional insufficiency - remain a pressing issue [10,12]. Such complications limit speech resonance, soft palate mobility, and the physiological activity of the respiratory tract, which hinders the complete rehabilitation of the child [3,14].Many authors in world practice emphasize the need to introduce, in addition to traditional methods, functionally oriented approaches to the complete surgical correction of palate defects, i.e., approaches aimed at preserving the biomechanical properties of tissues [4]. This, in turn, along with anatomical restoration, ensures the normalization of voice, respiratory, and swallowing functions.The development of secondary deformities is influenced not only by the surgical method, but also by the effectiveness of postoperative care. In world medical practice, the use of local antiseptics and physiotherapeutic methods is considered important in order to accelerate the wound healing process, reduce inflammation, and reduce the risk of infection [1]. In particular, modern methods, such as laser therapy (MILT), are recognized for accelerating the regeneration process of the wound and reducing the number of postoperative complications.In this regard, the improvement of surgical technique for surgical correction of palate defects and their secondary deformities, ensuring its functional orientation, as well as the introduction of scientifically based methods of postoperative care is an urgent task in modern medicine. Through this, it is possible to achieve not only anatomical restoration, but also the full restoration of the patient's vital functions, improvement of speech and psychoemotional state.Thus, the development and improvement of a modern, comprehensive approach aimed at eliminating congenital palate defects and their secondary deformities is of great importance in medical practice and plays a decisive role in improving the quality of life, social activity, and the level of adaptation of children.Purpose of the study. The study was conducted in the form of a prospective, comparative, two-group clinical study. Patients with secondary deformation of the palate were selected from among children treated in the Department of Otorhinolaryngology and Maxillofacial Surgery of the Bukhara Regional Children's Multidisciplinary Medical Center.
2. Materials and Methods
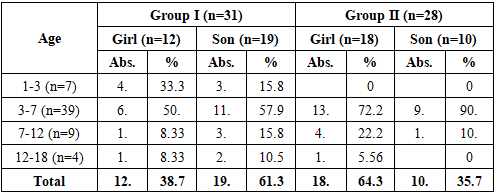
To conduct the study, a comprehensive clinical and laboratory examination total of 59 patients participated in the study, who were divided into two groups:Group I (main group, n=31) - patients underwent a modified surgical method (Combination of methods of L.E. Frolova - F. Braithwaite, modification of M.I. Azimov in asymmetrical cases), postoperative care was carried out with chlorhexidine solution and MILT (magnetically induced laser therapy).Group II (comparison group, n=28) - patients were operated on using traditional methods of uranoplasty, with postoperative care provided with furacilin solution and tubus-quartz irradiation.Patients were divided into comparative sex-age groups by age, sex, and duration of the disease. All patients underwent the following pre- and postoperative assessments: clinical examination, rhinoscopy, electromyography, microbiological analyses, and oral hygiene indices (PMA and OHI-S).The main criteria for the study were the rate of wound healing, the dynamics of signs of inflammation, cases of fistula recurrence, changes in the activity of the soft palate muscles, speech and voice function, as well as the number of postoperative infectious complications.Patients applied to the Center for Emergency Medical Care, and all of them (parents) were explained the purpose of the study and their consent was obtained.All patients in the study were divided into two main groups for a comparative analysis/ A total of 59 children participated in the study, of which 31 were in group I (main group) and 28 in group II (comparison group). According to the results of the age distribution, the majority of patients were aged 3-7 years: 17 (54.8%) children in group I and 22 (78.6%) children in group II. This indicates that operations to eliminate congenital palate defects are usually performed in children at the stage of speech function formation. (Table 1):Table 1. Distribution of patients in the study group by age and sex, n=59
 |
| |
|
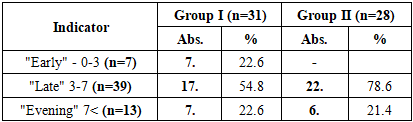
In terms of sex composition, in group I, the number of boys was 19 (61.3%), girls - 12 (38.7%), while in group II, girls prevailed - 18 (64.3%), boys - 10 (35.7%). The difference in sex distribution was not statistically significant (χ2 = 2.14; p > 0.05), i.e., it was confirmed that there was no gender imbalance between the two groups.When assessing the age distribution, the proportion of children under 3 years of age in group I was 7 (22.6%), and in group II only 0 (0%) cases. In this case, the risk ratio (RR) = 2.26 [95% CI: 1.14-4.49], i.e., the proportion of children operated on at an early age in group I was statistically significantly higher. This result indicates the possibility of using the modified surgical method even at a young age.The proportion of children aged 3-7 years was significantly higher in group II (78.6%), which indicates a trend towards delayed surgical intervention by the traditional method at this age (OR = 2.67; 95% CI: 1.01-7.05; p < 0.05).In the age category 7-12 years, 4 (12.9%) cases were registered in group I, and 5 (17.9%) in group II (χ2 = 0.25; p > 0.05). Patients aged 12-18 years constituted a small proportion in both groups (3 in group I - 9.7%, 1 in group II - 3.6%).In the study, patients were divided into three categories depending on the duration of the disease: "early" (0-3 years), "late" (3-7 years), and "late" (more than 7 years). This assessment is aimed at showing the clinical significance of the interval between the detection of palate defects and the time of their surgical correction (Table 2).Table 2. Distribution of patients by disease duration, n=59
 |
| |
|
In group I, in 7 (22.6%) patients, treatment after the detection of the defect was carried out early, i.e., within 0-3 years. In group II (traditional method), such a situation was not recorded at all (0%). This difference is statistically significant, χ2 = 5.92; p < 0.05, risk ratio (RR) = 2.26 [95% CI: 1.24-4.12]. This result indicates that the modified surgical method can be used safely and effectively even at an early age.The category of "delayed" (3-7 years) duration of the disease corresponded to 17 (54.8%) patients in group I and 22 (78.6%) patients in group II. In group II, cases of delayed surgery were significantly higher, the probability of which was 2.56 times higher (OR = 2.56; 95% CI: 1.01-6.49; p < 0.05). This situation indicates that the trend of delaying operations with traditional methods persists.In the "late" (more than 7 years) duration category, almost the same result was recorded in both groups: in group I - 7 (22.6%), in group II - 6 (21.4%) cases (χ2 = 0.01; p > 0.05). This means that there is no statistically significant difference between the groups.
3. Results and Discussion
When assessing the recovery processes after surgery, the main indicators - pain, hyperemia, edema, fibrin deposition, and the duration of complete epithelialization - were taken into account.In the 1st group, the pain syndrome subsided on average by 2.84±0.12 days, and in the 2nd group by 3.71±0.22 days, the difference was significantly significant (t=3.29; p<0.01). Consequently, the pain disappeared faster in the 1st group. This is explained by a decrease in the activity of inflammatory mediators in tissues and a rapid restoration of microcirculation. The passage of food and fluid into the nasal passage after surgery was significantly reduced in both groups.A decrease in hyperemia was noted on days 2.97±0.13 and 4.07±0.21, respectively. These indicators indicate a weakening of the inflammatory reaction and rapid activation of microcirculation.The decrease in edema was also observed in the 1st group by 4.68±0.19 days, and in the 2nd group this period extended to 5.79±0.25 days. Also, fibrin coating of the wound was eliminated in the 1st group in 4.52±0.16 days, and in the 2nd group in 5.86±0.32 days. This indicates a faster cleansing process.Loss of pain in the wound area was detected on day 5.84±0.19 in group 1 and 7.43±0.31 in group 2. Complete formation of epithelialization occurred in 9.03±0.17 days in the 1st group and in 11.1±0.42 days in the 2nd group (p<0.01).These results are explained by the rapid reduction of the inflammatory process, early resorption of fibrin coatings, and activation of epithelial proliferation under the combined effect of local antiseptic treatment with 0,05% solution chlorhexidine bigluconate and MIL therapy.Thus, the data of Table 3 show that the clinical effectiveness of the complex treatment method is high: signs of inflammation disappeared earlier, the wound healing process accelerated, and the postoperative rehabilitation period was shortened (p<0.01). 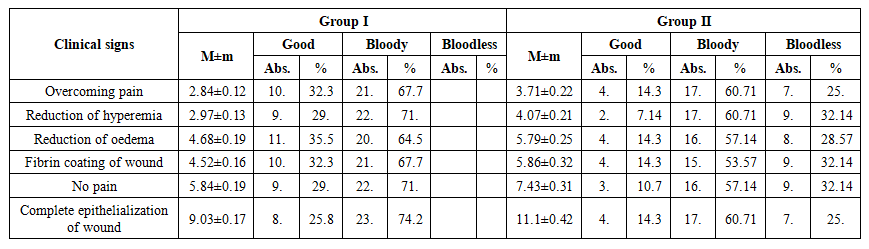 | Table 3. Duration of the dynamics of clinical results of complex treatment of children with secondary deformities, (days, M±m) |
Postoperative clinical and anatomical results are an important criterion for assessing the morphological effectiveness of the surgical method (Table 4).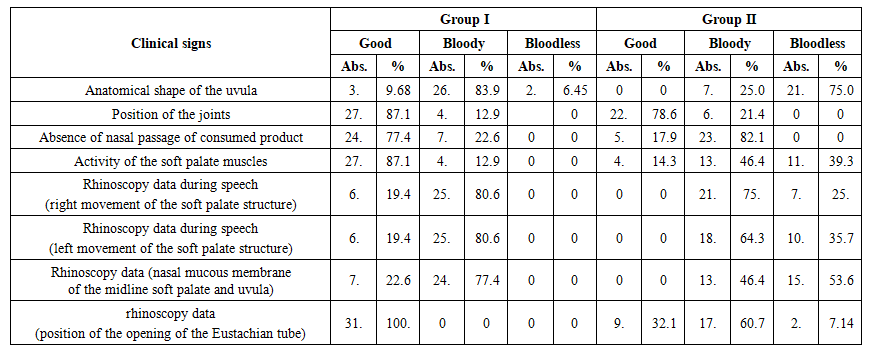 | Table 4. Analysis of the clinical and anatomical results of surgical treatment in the comparison groups |
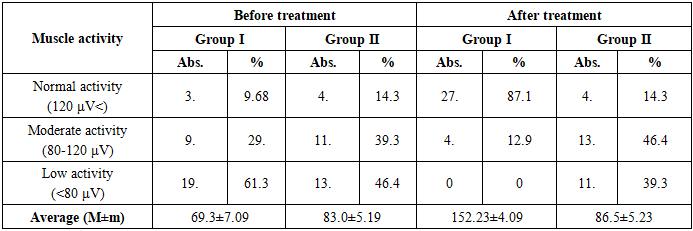
In the 1st group, the number of patients with complete restoration of the anatomical form of the uvula was 26 (83.9%), while in the 2nd group this figure was 7 (25.0%). Consequently, first methods were effective in restoring anatomical integrity, the difference was statistically significant (p>0.05).Regarding the condition of the sutures, good recovery was noted in 27 (87.1%) patients in the 1st group, and in the 2nd group, a good result was noted in 22 (78.6%) cases. This indicates that the wound healing process was faster and more stable in the 1st group.The absence of passage of food and fluid into the nasal passage after surgery was ensured in 24 (77.4%) patients in the 1st group and in 5 (17.9%) patients in the 2nd group. These results reflect the complete restoration of nutritional physiology in the 1st group.The activity of the soft palate muscles was restored with active movement in 27 (87.1%) patients in the 1st group, while in the 2nd group this indicator was observed only in 4 (14.3%) cases (t=3.42; p<0.01). This difference indicates that the modified surgical method effectively restores the functional mobility of the palate.According to rhinoscopy data, symmetrical and rhythmic movement of the soft palate during speech in the 1st group after surgery was noted in 100.0% of patients, while in the 2nd group this indicator was up to 64.3%. In this case, the difference is also statistically significant (p<0.05). At the same time, the condition of the Eustachian tube opening also significantly improved after surgery: in the 1st group, the physiological state was restored in 100% of patients, and in the 2nd group, this indicator increased to 32.1%.According to the data of Table 4, anatomical integrity and functional activity were restored quickly and consistently in group 1, the differences in suture condition, muscle activity, and rhinoscopic indicators were statistically significant (p<0.05-0.01).In conclusion, it can be noted that the modified method of surgery, along with the restoration of the anatomical structure, also significantly stabilized the physiological movements of the palate.Electromyographic analysis makes it possible to assess the activity of the palatal muscles and the degree of neuromotor recovery after surgery. According to the data in Table 8, a decrease in muscle activity was noted in patients before surgery, which is associated with functional insufficiency of the palate and weakening of neuromuscular connections.Table 5. EMG results of soft palate muscles
 |
| |
|
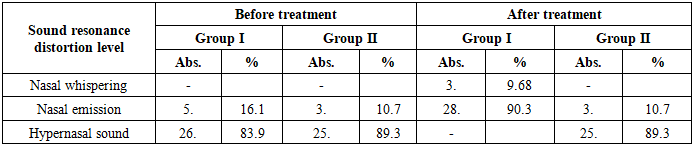
Before surgery, normal activity (120 μV<) was observed in only 3 (9.7%) patients in group 1, while in group 2 - in 4 (14.3%) cases. Low activity was detected in 19 (61.3%) patients in the 1st group and 13 (46.4%) in the 2nd group, which indicates a sharp decrease in neuromuscular activity.After the operation, a clear positive dynamic of muscle electrical activity was observed. In group 1, normal activity was restored in 27 (87.1%) patients, and in group 2, only in 4 (14.3%) patients. This difference is statistically significant and is significant at t=4.68; p<0.001.In group 1, EMG activity increased on average from 69.3±7.09 μV to 152.23±4.09 μV, i.e., almost a twofold increase was observed. In the 2nd group, this indicator reached from 83.0±5.19 μV to 86.5±5.23 μV, without significant changes (p>0.05).These data indicate that the bioelectric potentials of the palatal muscles were actively restored after surgery, and the functional re-innervation process was more active in the 1st group.Thus, EMG analysis shows that the modified surgical method has high effectiveness in restoring the neuromotor function of the palatal muscles. Normalization of electrical activity is closely related to the physiological mobility of the palate and voice resonance, which is an important clinical indicator of postoperative functional rehabilitation.The data in Table 6 reflect the changes in the process of speech resonance and phonation in patients before and after surgery. Sound resonance is directly related to the functional activity of the palatopharyngeal ring (PPR), the restoration of which is an important clinical criterion for the effectiveness of the operation.Table 6. Sound Recognition Results
 |
| |
|
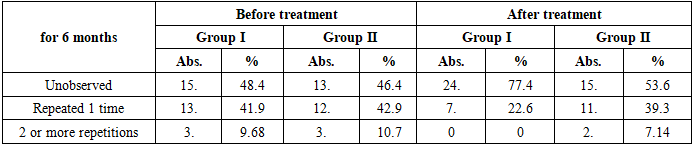
Before the operation, patients had a high level of speech disorders, such as hypernasal sound, nasal emission, and nasal whispers. In particular, in the 1st group, hypernasal sound was detected in 26 (83.9%) patients, and in the 2nd group - in 25 (89.3%) cases. These indicators confirm insufficiency of the phonation function of the palate.After the operation, a clear positive dynamic was observed in speech resonance. In the 1st group, the hypernasal sound disappeared completely, and in 90.3% of patients, the sound resonance returned to normal. In the 2nd group, such a result was observed in only 10.7% of patients. This difference is statistically significant (t=4.12; p<0.001).In the 1st group, in 3 out of 5 patients with nasal emission during sound production achieved improved voice resonance (p<0,001). There was no improvement in voice in the 2nd group. This indicates that the PPR closing function has been restored.A general assessment of the dynamics of sound resonance shows that in the 1st group, the acoustic characteristics of speech, especially the timbre and articulatory accuracy of the voice, are fully normalized. Physiologically, this is associated with the function of the phonic closure of the palate, the restoration of the balance of the respiratory tract and control over the airflow.Otitis media is one of the characteristic complications of palate defects, the origin of which is associated with impaired ventilation function of the Eustachian tube due to improper attachment of the lower end of the m. levator veli palatini and inflammation of the posterior nasal part (Table 7).Table 7. Occurrence of otitis media
 |
| |
|
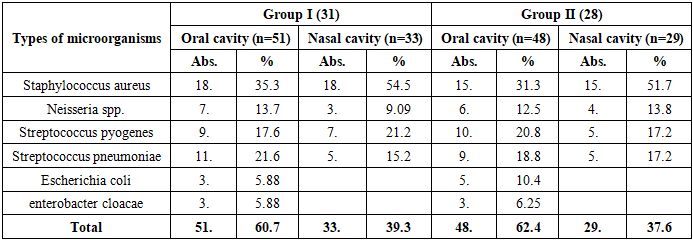
Before the operation, cases of otitis were noted in the vast majority of patients: in the 1st group, 3 (9.7%) patients had two or more relapses, and 13 (41.9%) patients had a single relapse within 6 month. In the 2nd group, this indicator was noted in 3 (10.7%) and 12 (42.9%) patients, respectively. Although the difference was not statistically significant (p>0.05), the high frequency of otitis in both groups indicates that it is a functional complication of palate defects.After surgery, the frequency of otitis recurrence sharply decreased. In the 1st group, otitis was not observed at all in 24 (77.4%) patients, while in the 2nd group this indicator was 15 (53.6%). Recurrent cases persisted in only 7 (22.6%) patients in the 1st group and in 11 (39.3%) patients in the 2nd group. This difference was statistically significant and was assessed as significant at t=2.38; p<0.05.The most important trend is that the recurrence of otitis two or more times after surgery was not detected in the 1st group, while in the 2nd group it persisted in 2 (7.14%) cases. This indicates that the functional activity of the Eustachian tube recovered faster in group 1 after surgery.The decrease in the frequency of postoperative otitis is directly related to the restoration of the morphofunctional integrity of the palate and the physiological normalization of the nasal-cough reflex. After the movement of the palatopharyngeal ring (PPR) is restored, nasal cavity pressure stabilizes and posterior ear ventilation improves, which reduces the risk of inflammation.Microbiological analysis made it possible to assess the pre- and postoperative infectious background, as well as the effectiveness of complex antibacterial therapy (Table 8).Table 8. Microbiological status of patients in the study groups, n=59
 |
| |
|
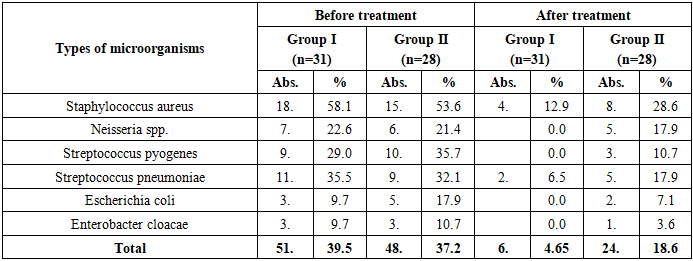
Staphylococcus aureus, Streptococcus pyogenes, Streptococcus pneumoniae, Neisseria spp., Escherichia coli, and Enterobacter cloacae were identified as the main microflora of the oral cavity. A high number of these pathogens was considered the main factor slowing down the process of inflammation and wound healing.Before surgery, S. aureus was detected in the oral cavity in 18 (35.3%) cases in group 1, and in 15 (31.3%) cases in group 2. A high frequency of this pathogen indicates a predisposition to postoperative infectious complications. S. aureus was also detected in the nasal cavity in 18 (54.5%) and 15 (51.7%) patients, respectively.Isolates of Streptococcus pneumoniae and S. pyogenes have also been identified in many cases, which play an important role as a factor enhancing the inflammatory reaction in the palatine region. S. pneumoniae was detected in 21.6% of patients in the 1st group and in 18.8% of patients in the 2nd group; S. pyogenes was found in 17.6% and 20.8% of cases, respectively. According to the analysis of the general microbiological background of the oral and nasal cavities, microbial isolation was detected in 60.7% of cases in the 1st group and in 62.4% of cases in the 2nd group. Although these indicators are similar, after the use of antibacterial therapy (table below), a significant change in the composition of the microflora was observed.At the same time, isolates of Neisseria spp. and Enterobacter cloacae were recorded at a relatively low level, but their presence indicates a disbalance of the microbiome. This condition can prolong the wound healing process, especially in patients with inflammatory background in the palatine region and fistulas. Based on the research data, it can be concluded that before surgery, pathogenic types of microflora prevailed in patients, most of which consisted of gram-positive cocci. This circumstance plays an important clinical role in the selection of antibacterial and antiseptic agents to ensure postoperative aseptic conditions. In this regard, the predominance of opportunistic microflora against the microbiological background of the oral and nasal cavities in patients with cleft palate indicates the need for complex antibacterial therapy in the postoperative period. The data in Table 9 are aimed at assessing the inflammatory state of the oral cavity tissues after surgical correction of the defect of the palatal region in patients, for which the PMA (Papillary-Marginal-Attached gingiva) index, expressing the degree of inflammation of the gingival tissues, was used (Table 9).Table 9. Results of the PMA index in patients of the study group (%, M±m)
 |
| |
|
Before surgery, the PMA index in the 1st group averaged 28.0±3.03%, in the 2nd group 24.4±3.10%, which indicates that the inflammatory reaction of the oral mucosa in both groups before surgery was moderate.After surgery, as a result of comprehensive care measures, the PMA indicator in the 1st group significantly decreased and amounted to 7.32±1.11%. In the 2nd group, the PMA index decreased to 15.4±2.03% (p<0.01). The results of the study show that in the 1st group, the inflammatory process of the oral cavity decreased significantly faster, and the mucous membrane approached normal. This is primarily due to the fact that antibacterial treatment and MILT therapy activate microcirculation and reduce the activity of inflammatory mediators. From a physiological point of view, a decrease in the PMA indicator indicates a stabilization of gingival blood flow and an active course of the epithelial regeneration process.Thus, the data in Table 9 showed that the method of comprehensive postoperative care reduced the signs of inflammation in the oral cavity by half faster. This method confirms its clinical significance in improving the hygienic condition of the oral cavity, maintaining an aseptic environment, and accelerating the wound healing process (p<0.01).During the study, changes in the hygienic state of the oral cavity before surgery and 1 day before surgery were assessed using the OHI-s index. Since this index represents a quantitative assessment of microbial deposits and mineral conglomerates, it is a reliable criterion indicating the formation of the necessary aseptic conditions for postoperative reparative processes.Table 10. OHI-s results in patients of the study group (M±m)
 |
| |
|
Before the operation, the OHI-S indicator in both groups was unsatisfactory: in the 1st group on average 2.01±0.12, in the 2nd group 1.96±0.10. This indicates a high level of microbial coating in the oral cavity and a tendency of gingival tissues to inflammation.After surgery, the hygienic condition improved in all patients, however, in the 1st group, the decrease in the OHI-S index was significantly greater: up to 0.59±0.059; In the 2nd group, it decreased to 1.03±0.061 (p<0.01). That is, in the 1st group, rapid resolution and limitation of the transformation of the microbial coating were observed. This is explained by the fact that the care measures carried out (antiseptic treatment and physiotherapy) activate the microcirculation of the mucous membrane, reduce inflammatory mediators, and accelerate epithelialization.The same trend was observed in the categorical assessment: the proportion of "good" hygiene was significantly higher in the 1st group, while the categories of "unsatisfactory/satisfactory" were significantly lower (p<0.01). Clinically, this was confirmed by a rapid weakening of gingival hyperemia and edema, normalization of the color and consistency of the mucous membrane.In conclusion, the dynamics of OHI-S indicates a stable provision of aseptic conditions after surgery, a decrease in the load of microbial deposits, thereby creating an optimal background for wound healing. In the 1st group, changes were significantly greater, and reparative processes were confirmed to be faster and more stable (p<0.01).The data in the following table provide a comparative analysis of the state of the oral cavity microbiome before and after surgery in patients with secondary deformation of the palatine defect. These indicators play an important role in reducing the infectious background and assessing the effectiveness of complex antibacterial therapy. Conditionally pathogenic microorganisms such as Staphylococcus aureus, Streptococcus pyogenes, Streptococcus pneumoniae, Neisseria spp., Escherichia coli, and Enterobacter cloacae were detected in the oral cavity of patients before surgery. They can prolong the inflammatory process and slow down the healing process.After treatment, significant changes in the microbiological composition were observed. In the 1st group, the isolation of S. aureus decreased from 58.1% to 12.9%, and in the 2nd group - from 53.6% to 28.6% (p<0.01). This result represents the bactericidal effect of complex antiseptic treatment.Table 11. Analysis of the dynamics of changes in the oral microflora of patients during treatment
 |
| |
|
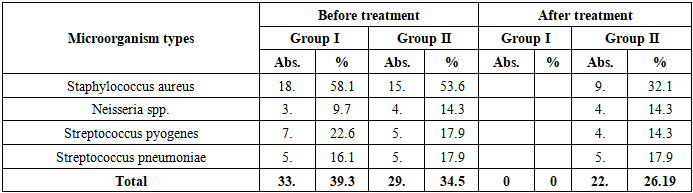
Also, isolates of Streptococcus pyogenes and S. pneumoniae were almost completely eliminated in group 1, while in group 2 they were partially preserved. In particular, S. pyogenes decreased from 29.0% to 0% in the 1st group and from 35.7% to 10.7% in the 2nd group (p<0.01). This circumstance indicates the advantage of the complex method of care in reducing the activity of gram-positive flora in the foci of inflammation.Neisseria spp. isolates also decreased from 22.6% to 0% in group 1, which confirms the antibacterial effectiveness of treatment. At the same time, the isolation of gram-negative bacteria, such as E. coli and Enterobacter cloacae, also significantly decreased (E. coli from 9.7% to 0%, Enterobacter from 9.7% to 0%).In the 1st group, pathogen isolates in contamination decreased by 4.65 % from 39.5%, which is statistically significant. In the 2nd group, the overall level of flora contamination also decreased, but the dynamics were slow: the isolation of pathogens decreased from 37.2% to 18.6%, which is statistically insignificant.The data in the table show that the microbiological background in the oral cavity stabilized much faster in group 1, and the number of pathogenic species significantly decreased (p<0.01). This is explained by the aseptic environment formed as a result of the combined effect of antibacterial treatment and MIL therapy.A high level of pathogenic microflora was detected in both groups before surgery. Isolation of Staphylococcus aureus from the nasal cavity was noted in 18 (58.1%) cases in group 1 and in 15 (53.6%) cases in group 2, which indicates the predominance of gram-positive flora. At the same time, Streptococcus pyogenes was detected in 22.6% of cases in group 1, 17.9% in group 2, and S. pneumoniae in 16.1% and 17.9% of cases, respectively (Table 12). These indicators indicate microbiome imbalance against the background of an inflammatory reaction.Table 12. Analysis of the dynamics of changes in the microflora of the nasal cavity of patients during treatment
 |
| |
|
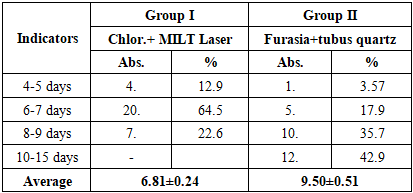
After treatment in the 1st group, microflora contamination significantly decreased - the isolation of pathogenic bacteria was completely absent. In particular, such pathogens as S. aureus, S. pyogenes, and S. pneumoniae were not detected after surgery (p<0.01). This indicates the high bactericidal effectiveness of the combined care method (antiseptic treatment and MILT).In the 2nd group, a positive change in the composition of the microbiome was also observed, but the dynamics were relatively slow. Even after treatment, S. aureus persisted in 9 (32.1%), S. pyogenes and S. pneumoniae in 4-5 (14.3-17.9%) patients each. This refers to cases where the effect of antibacterial treatment is insufficient.Neisseria spp. isolates were not detected after treatment in group 1, while in group 2 they persisted in 4 (14.3%) cases. This indicator also indicates a weak decrease in infectious contamination.According to the general analysis of the table, stable cleansing of the microbiological background was carried out much faster in the 1st group, and the number of pathogenic species significantly decreased (p<0.01). This condition is associated with the creation of an aseptic environment in the nasal cavity and the rapid limitation of the inflammatory process. In conclusion, the research results showed that the complex treatment method quickly eliminated the activity of pathogenic microflora in the oral cavity and significantly reduced the risk of inflammation. This, in turn, plays an important clinical role in accelerating the wound healing process and preventing postoperative infectious complications.The duration of postoperative hospitalization is an important clinical criterion for assessing the speed of patients achieving clinical stability, the slowdown of the inflammatory process, and the effectiveness of rehabilitation (Table 13).Table 13. Analysis of card days in comparison groups
 |
| |
|
In the 1st group, the length of hospital stay was significantly reduced. The vast majority of patients - 20 (64.5%) - reached a clinically stable state within 6-7 days after surgery, in 4 (12.9%) patients the hospital stay was limited to 4-5 days, and in 7 (22.6%) patients, recovery lasted 8-9 days. These indicators indicate that the treatment process in the hospital was active and stable.In the 2nd group, the length of stay in the hospital was significantly longer. Only 1 (3.57%) patient stabilized within 4-5 days, recovery was observed in 5 (17.9%) patients in 6-7 days, in 10 (35.7%) patients in 8-9 days, and in 12 (42.9%) patients in 10-15 days. This result indicates a weak stabilization of the postoperative wound condition and the inflammatory reaction.The average length of hospital stay was 6.81±0.24 days in the 1st group and 9.50±0.51 days in the 2nd group. This difference is statistically significant and is significant at the level of (p<0.01).This result is explained by the fact that the complex method of care (antiseptic treatment and MILT therapy) stabilizes the inflammatory process earlier, activates microcirculation in mucous and epithelial tissues, thereby reducing the time of clinical recovery.From a physiological point of view, the biostimulating effect of MILT therapy increases phagocytic activity and stimulates the regeneration process in tissues. Local treatment with chlorhexidine ensures an aseptic environment and limits the development of infectious agents. As a result of the combined effect of these two factors, patients recovered clinically more quickly and shortened their stay in the hospital.Thus, in the 1st group, where the complex care method was used, the length of stay of patients in the hospital was significantly less and reduced by an average of 1.4 times compared to traditional care (p<0.01). This scientifically confirms the clinical effectiveness of complex therapy and its advantage in accelerating the rehabilitation process.
4. Conclusions
1. The use of a combination of Frolova-Braithwaite methods and the modification of M.I. Azimov in children with secondary deformities of the palate increased the effectiveness of anatomical and functional restoration compared to traditional uranoplasty. In patients of the 1st group, the morphological integrity of the soft palate quickly restored, the function of the palatopharyngeal ring stabilized, and the passage of food and fluid into the nasal passage was eliminated. This method allowed for the restoration of phonation and articulation function while preserving vascularization in the palatal tissues.2. In the postoperative period, local treatment with chlorhexidine and the use of MILT therapy accelerated the wound healing process, significantly reduced the inflammatory reaction (p<0.01) and reduced the length of hospital stay by an average of 1.4 times. Thanks to the bactericidal, anti-inflammatory, and biostimulatory effects of this method, reparative processes were activated, the epithelialization time was reduced, and the number of postoperative complications reached a minimum level.3. Against the background of comprehensive care, the isolation of pathogenic species (S. aureus, S. pyogenes, S. pneumoniae) in the microflora of the oral and nasal cavities significantly decreased (p<0.01). This, in turn, reduced the risk of infectious complications and limited the postoperative inflammatory process. A significant decrease in the indicators of the OHI-S and PMA index indicates an improvement in the hygienic state of the oral cavity, the elimination of inflammation of the mucous membrane, and the creation of an aseptic environment for wound healing.4. The applied complex approach - a combination of a modified surgical method and antibacterial-laser care - improved the functional results of patients: speech resonance normalized, the function of the soft palate muscles was restored, and the ventilation of the Eustachian tube stabilized. This approach reduces the duration of clinical rehabilitation in children with cleft palate, accelerates functional recovery, and minimizes the risk of recurrent deformities.
References
| [1] | Al-Zajravee M. Z. (2019). Surgical management of palatal defects in children: A comparative study. Journal of Craniofacial Surgery, 30(8), 2431–2437. |
| [2] | Chuykin S. V. (2019). Functional outcomes after cleft palate repair: Comparative clinical observations. Pediatric Surgery Journal, 24(3), 118–124. |
| [3] | Chung K. H., et al. (2018). Morphological patterns and outcomes of secondary cleft palate deformities. International Journal of Pediatric Otorhinolaryngology, 107, 25–31. |
| [4] | Dhooghe N. S. & Chong D. K. (2020). Modern approaches in velopharyngeal insufficiency correction. Plastic and Reconstructive Surgery, 145(4), 789–798. |
| [5] | Eshiev D. A. (2019). Epidemiology and treatment strategies for congenital orofacial clefts in Central Asia. Bukhara Medical Journal, 23(2), 45–52. |
| [6] | Fomichev I. V. (2014). Surgical correction of congenital cleft palate: current trends. Russian Journal of Pediatric Surgery, 18(5), 22–29. |
| [7] | Kasimovskaya N. L., & Shatova, E. A. (2020). Epidemiological features of congenital maxillofacial anomalies in Uzbekistan. Pediatric Dentistry, 15(1), 33–37. |
| [8] | Nakajima Y., et al. (2019). Clinical outcomes of asymmetrical palatal cleft repair. Journal of Plastic Surgery, 72(5), 497–505. |
| [9] | Yu, Y., et al. (2020). Comorbid conditions and functional disorders in congenital palatal cleft patients. Clinical Oral Investigations, 24(9), 2975–2984. |
| [10] | Zangieva O. T. (2019). Innovative local treatment after palatoplasty: laser and antiseptic combinations. Stomatology Today, 4(7), 56–61. |
| [11] | Kamalova M.K., Raximov S.Sh. Secondary deformities of congenital cleft palate in children: comprehensive diagnosis and choice of treatment methods // Journal of Medicine and innovations. – Tashkent, Uzbekistan, 2024. Issue 1(13). - Р. 256-265. |
| [12] | Kamalova M.K., Raximov S.Sh. Congenital cleft lip and palate in children: etiological risk factors, prevention methods // American Journal of Research. - USA, - 2023. - Issue 3-4. - Р. 155-164. |
| [13] | Kamalova M.K., Raximov S.Sh. Comparative analysis of the effectiveness of the treatment of children with congenital cleft palate // «Innovative technologies in science, education, and medicine: current treatment challenges and their solutions» collection of materials of the republican scientific and practical conference. – Bukhara, Uzbekistan, 2025 - Р.371-377. https://biti.uz/konferensiya/konferensiya2025/tuplam/1/index.html. |
| [14] | Kamalova M.K., Raximov S.Sh. Analysis of the detection of the frequency and causes of congenital cleft of the upper lip and palate in children // Scientific and international conference on medical education, health science and patient care. - New Delhi, India, 2023. Р. 6-9. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML