Khasanova Sh. B., Nadjmitdinova D. A.
Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The aim of this study is to analyze the clinical and neurological manifestations and risk factors of cerebral circulatory disorders (CСD) in pregnant women. A retrospective analysis of 72 clinical cases was performed. The most common forms of CCD, concomitant somatic pathologies, as well as the dynamics of neurological symptoms depending on the duration of pregnancy and treatment were identified. The data obtained emphasize the importance of early diagnosis and a multidisciplinary approach to the management of pregnant women with vascular pathology.
Keywords:
CCD, Pregnancy, Diagnosis, Complications, Outcomes, Prevention
Cite this paper: Khasanova Sh. B., Nadjmitdinova D. A., Cerebrovascular Accident in Pregnant Women: Clinical Observations and Their Description, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3969-3970. doi: 10.5923/j.ajmms.20251511.50.
1. Introduction
Cerebral circulatory disorders (CСD) in pregnant women are a serious medical problem that can lead to adverse outcomes for both the mother and the fetus [2,7,8,10,12]. During pregnancy, physiological hypercoagulation, hemodynamic changes and concomitant diseases increase the risk of vascular catastrophes [1,3,6,9,11].
2. Materials and Methods
A retrospective analysis of 72 pregnant women with CСD admitted toShox International Hospital in the period from 2022 to 2025 was performed. Medical history, neurological status, MRI results, labor outcomes, and the presence of complications were evaluated.
3. Results and Their Discussion
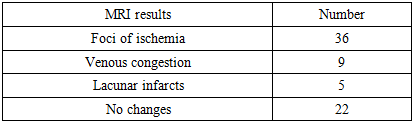
Foci of ischemia were found in 36 patients (50%) and were the most common finding. 9 patients (12.5%) showed signs of venous congestion, 5 (6.9%) had lacunar infarcts. In 22 (30.6%) patients, changes in MRI were not detected, despite clinical symptoms.Table 1. Results of MRI examination
 |
| |
|
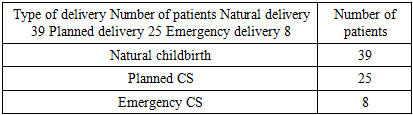
Visualization clearly demonstrates the predominance of ischemic foci in comparison with other forms of changes.Table 2. Labor outcomes
 |
| |
|
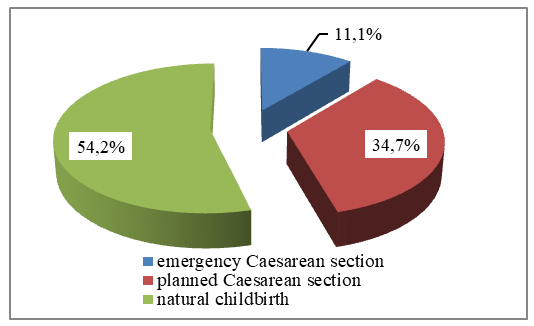 | Figure 1. Structure of delivery in women with CCD |
The chart shows the preference for natural childbirth when the condition of the mother and fetus is satisfactory.Table 3. Complications identified in patients
 |
| |
|
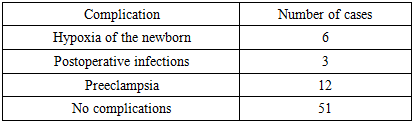
The most frequently noted Preeclampsia (12 cases) and neonatal hypoxia (6 cases) were the most common. Postoperative infectious complications were observed in 3 women. No complications were detected in 51 patients (70.8%).Prevail preeclampsia and hypoxia predominated, while infectious complications were less common.In pregnant women with impaired cerebral circulation, the most common foci of ischemia are found according to MRI data. It is important to emphasize that the detected changes on MRI in most cases correlated with the clinical picture, including headache, dizziness, paresthesia and focal neurological symptoms. This makes it possible to use MRI as a reliable method of objective assessment of the severity of vascular pathology during pregnancy.The choice of delivery method depended on the severity of the neurological deficit and the degree of compensation for the underlying disease. Some patients had a need for emergency delivery for vital indications, especially in cases of progressive ischemic processes.Pregnancy management in women with CCD requires the participation of a multidisciplinary team of specialists: obstetricians and gynecologists, neurologists, anesthesiologists, and neonatologists. This approach allows you to respond in a timely manner to changes in the condition of both the mother and the fetus.It is also necessary to emphasize the importance of timely diagnosis of hypercoagulable conditions that are common during pregnancy, especially in women with hereditary thrombophilia or a burdened vascular history. The use of low-molecular-weight heparins and antiplatelet agents in these cases can significantly reduce the risk of stroke and other vascular disasters.Thus, the integration of neurological and obstetric approaches can significantly improve the safety of pregnancy and delivery in patients with CCD.
4. Conclusions
1. CVA in pregnant women requires timely diagnosis and a specialized approach to treatment. More than a third of patients requiresurgical delivery.2. MRI remains an important method for visualizing vascular pathology during pregnancy.3. Prevention of complications requires multidisciplinary monitoring and individual tactics of pregnancy management.
References
| [1] | Bushnell, C., & Chireau, M. (2017). Pregnancy and stroke: Clinical presentation, evaluation, treatment, and prognosis. Stroke, 48(7), 1750–1755. https://doi.org/10.1161/STROKEAHA.117.016267. |
| [2] | Jaigobin, C., & Silver, F. L. (2000). Stroke and pregnancy. Stroke, 31(12), 2948–2951. https://doi.org/10.1161/01.STR.31.12.2948. |
| [3] | James, A. H. (2009). Venous thromboembolism in pregnancy. Arteriosclerosis, Thrombosis, and Vascular Biology, 29(3), 326–331. https://doi.org/10.1161/ATVBAHA.108.179689. |
| [4] | Lanska, D. J., & Kryscio, R. J. (2000). Risk factors for peripartum and postpartum stroke and intracranial venous thrombosis. Stroke, 31(6), 1274–1282. https://doi.org/10.1161/01.STR.31.6.1274. |
| [5] | Leffert, L. R., Clancy, C. R., Bateman, B. T., Bryant, A. S., & Kuklina, E. V. (2015). Patient characteristics and outcomes after hemorrhagic stroke in pregnancy. Circulation: Cardiovascular Quality and Outcomes, 8(6), S170–S178. https://doi.org/10.1161/CIRCOUTCOMES.115.002240. |
| [6] | Miller, E. C., & Elkind, M. S. V. (2021). Stroke in pregnancy and the postpartum period. Nature Reviews Neurology, 17(4), 229–240. https://doi.org/10.1038/s41582-021-00474-z. |
| [7] | Sare, G. M., Gray, L. J., Bath, P. M., & Freeman, D. J. (2013). Management of stroke in pregnancy and puerperium. Expert Review of Neurotherapeutics, 13(2), 205–214. https://doi.org/10.1586/ern.12.145. |
| [8] | Swartz, R. H., Cayley, M. L., Foley, N., Ladhani, N., Leffert, L., & Bushnell, C. (2017). The incidence of pregnancy-related stroke: A systematic review and meta-analysis. International Journal of Stroke, 12(7), 687–697. https://doi.org/10.1177/1747493017701940. |
| [9] | Wang, A., & Magee, L. A. (2019). Hypertensive disorders in pregnancy and stroke risk. Current Hypertension Reports, 21(8), 1–8. https://doi.org/10.1007/s11906-019-0964-0. |
| [10] | Wendelboe, A. M., & Raskob, G. E. (2016). Global burden of thrombosis: Epidemiologic aspects. Circulation Research, 118(9), 1340–1347. https://doi.org/10.1161/CIRCRESAHA.115.306841. |
| [11] | Wilkins, I. A., & Ugwumadu, A. (2020). Neurological emergencies in obstetrics: Recognition and management. Obstetrics, Gynaecology & Reproductive Medicine, 30(2), 47–52. https://doi.org/10.1016/j.ogrm.2019.11.001. |
| [12] | Zipursky, A., Ray, J. G., & Verma, A. (2018). Risk factors and outcomes of pregnancy-associated stroke. The Lancet Neurology, 17(9), 773–785. https://doi.org/10.1016/S1474-4422(18)30214-1. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML