-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3945-3947
doi:10.5923/j.ajmms.20251511.42
Received: Oct. 7, 2025; Accepted: Nov. 6, 2025; Published: Nov. 14, 2025

Features of Occurrence and Mortality from Ischemic and Hemorrhagic Stroke in the Fergana Valley for 2020
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMamataliyeva Janona Alimjanovna1, Usmanova Durdona Djurabayevna2
1Fergana Medical Institute of Public Health, Fergana, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The Fergana Valley is characterized by a continental climate with hot summers and cold winters, which can contribute to increased temperature strain on the body, increasing the risk of developing diseases associated with circulatory disorders, including strokes and other cerebrovascular diseases. High temperatures during the summer period can increase the load on the cardiovascular system, and in winter, cause vascular disorders, which contributes to increased morbidity. The climatic conditions of the Fergana Valley also contribute to the high level of air pollution, especially in cities with developed industrial centers.
Keywords: Ischemic stroke, Fergana Valley, Epidemiology, Occurrence, Mortality
Cite this paper: Mamataliyeva Janona Alimjanovna, Usmanova Durdona Djurabayevna, Features of Occurrence and Mortality from Ischemic and Hemorrhagic Stroke in the Fergana Valley for 2020, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3945-3947. doi: 10.5923/j.ajmms.20251511.42.
1. Introduction
- Stroke is one of the main medical and social problems of our time, occupying a leading place among the causes of death and disability. For regions with different climatic and geographical features, differences in stroke structure and outcome are characteristic. The Fergana Valley unites three regions - Fergana, Andijan, and Namangan, where there are significant differences in the level of medical infrastructure and accessibility of specialized care. The purpose of the study was to conduct a comparative analysis of the epidemiological characteristics of stroke in these regions [1].Increased concentrations of dust, sulfur dioxide, and other pollutants in the air can worsen the health of residents, leading to chronic diseases, including cardiovascular diseases and strokes. For example, in Fergana and Andijan, the concentration of pollutants in the air periodically exceeds permissible limits, which is a risk factor for the development of cerebrovascular diseases. Industrial enterprises located in the Fergana, Andijan, and Namangan regions also have an impact on the health of the local population. In these regions, the textile industry, cement plants, and the petrochemical and gas industries are actively developing, leading to the release of pollutants into the atmosphere [2]. Acute cerebrovascular disorders (CEB) remain one of the leading medical and social problems of modern healthcare, occupying a leading position in the structure of morbidity, mortality, and disability of the population worldwide. According to the World Health Organization, more than 15 million cases of stroke are registered annually worldwide, of which about 6 million result in death, making cerebrovascular diseases the second leading cause of death after coronary heart disease [3].Stroke is a heterogeneous group of diseases, the main forms of which are ischemic stroke (II), caused by a disruption in the blood supply of a section of brain tissue due to cerebral arterial thrombosis or embolism, and hemorrhagic stroke (GI), arising from the rupture of cerebral vessels with the formation of an intracerebral hematoma or subarachnoid hemorrhage. The ratio of these forms, their occurrence, and outcomes vary significantly across different populations, which is determined by a complex of genetic, demographic, socio-economic, and ecological factors [4].The global burden of stroke is characterized by pronounced regional differences in both morbidity indicators and the structure of disease subtypes. In developed countries, ischemic stroke accounts for 80-85% of all BMD cases, while in low- and middle-income countries, this figure is 65-70%, and the proportion of hemorrhagic stroke increases to 30-35%, respectively. These differences reflect the peculiarities of the prevalence of risk factors, accessibility of medical care, and the effectiveness of preventive programs [5].Ischemic stroke, being the most frequent form of ONMK, is characterized by a relatively more favorable prognosis compared to hemorrhagic stroke. Nevertheless, the absolute mortality rate from ischemic stroke remains high due to its significant prevalence. The mortality rate in ischemic stroke in the acute phase (first 7 days) is 8-12%, increasing to 15-25% by the end of the first month and reaching 25-40% within the first year of the illness [6].Hemorrhagic stroke, despite its lower frequency, is characterized by a more severe course and an unfavorable prognosis. Mortality in intracerebral hemorrhage in the acute period reaches 35-50%, and annual mortality is 50-70%. Subarachnoid hemorrhages are characterized by even higher mortality rates, reaching 45-60% on the first day and 60-80% throughout the year. The factors determining the occurrence of different types of stroke include age, gender, racial, and ethnic characteristics of the population. Ischemic stroke develops more often in older age groups, its frequency increases exponentially after 65 years, doubling every 10 years of life. Hemorrhagic stroke has a more uniform age distribution, often affecting people of working age, which determines its high socio-economic significance [7].Gender differences in stroke epidemiology are manifested in higher male morbidity in young and middle age groups, while in older age groups, female morbidity rates exceed male rates. This is due to the earlier development of atherosclerotic changes in men and the protective effect of estrogens in women during the reproductive period [8].Ethnic and racial differences in stroke structure are particularly pronounced for the hemorrhagic subtype. Representatives of Asian populations have a higher frequency of intracerebral hemorrhages, which is associated with the genetic characteristics of the vascular wall, the high prevalence of arterial hypertension, and specific nutritional factors. Temporal trends in stroke epidemiology demonstrate diverse changes for the ischemic and hemorrhagic subtypes. In most developed countries, there is a decrease in age-standardized rates of stroke morbidity and mortality, which is associated with improved risk factors control, development of preventive programs, and improvement of medical care. However, the absolute number of stroke cases continues to grow due to population aging [9].The mortality rate in stroke depends on many factors, including the patient's age, the severity of the neurological deficit, the location and extent of the lesion, the presence of comorbidities, the timing of treatment, and the quality of medical care. The introduction of a specialized care system for stroke, including pre-hospital diagnostics, transportation to specialized centers, thrombolitic therapy, and endovascular interventions, has led to a significant decrease in mortality, especially in ischemic stroke [10].Purpose of the study: to conduct a comparative analysis of the features of the occurrence and mortality of ischemic and hemorrhagic stroke to optimize the system of medical care and develop differentiated prevention strategies.
2. Materials and Methods
- The study is based on the analysis of regional registers of acute cerebrovascular disorders (ACD) in the Fergana, Andijan, and Namangan regions for 2020. A comparison of the proportion of ischemic and hemorrhagic strokes, mortality rates, and mortality rates was conducted. Descriptive and comparative statistics methods, as well as dynamic series analysis, were used.
3. Research Results
|
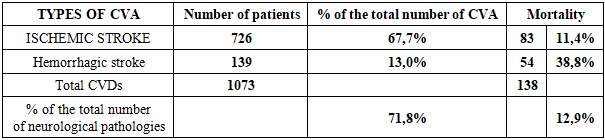
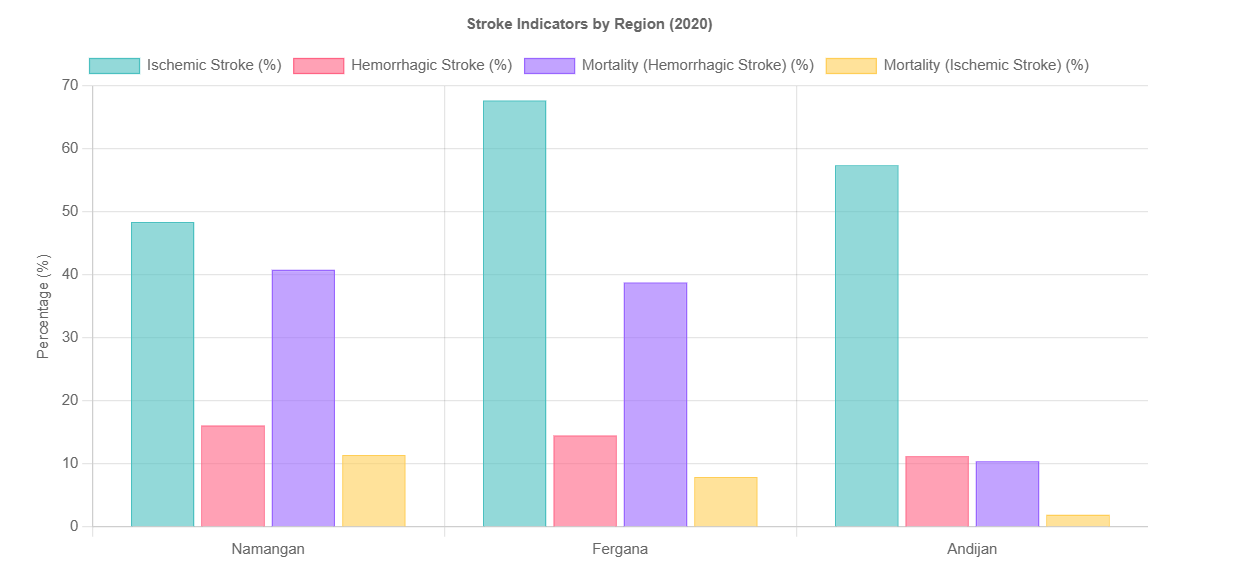 | Figure 1. Comparative Analysis of Stroke Indicators (2020) |
4. Conclusions
- Ischemic stroke is the dominant subtype of BMD in all three regions of the Fergana Valley, its proportion fluctuates within 48-68% of the total number of cerebrovascular diseases. Hemorrhagic stroke, although less common, is characterized by significantly higher mortality (up to 40.8%), which requires strengthening early diagnostic measures, improving neurosurgical care, and monitoring patients in the acute period. Regional differences in mortality and mortality are likely due to the heterogeneity of medical infrastructure, varying hospitalization periods, and socio-demographic factors. The high proportion of cerebrovascular diseases among all neurological pathologies (47-72%) confirms the significance of stroke as a leading medical and social problem in the Fergana Valley. To reduce mortality and disability, it is necessary to implement personalized prevention programs, develop regional vascular centers, and standardize protocols for managing stroke patients.