-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3907-3911
doi:10.5923/j.ajmms.20251511.31
Received: Oct. 16, 2025; Accepted: Nov. 10, 2025; Published: Nov. 14, 2025

Distinctive Features of Depressive Disorders in Parkinson's Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNaimov Olim Yunusovich, Matmurodov Rustambek Jumanazarovich, Muminov Bekzod Askarovich, Jumanazarova Shakhzoda Rustambekovna
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

One of the most pressing problems of modern neurology is neurodegenerative diseases of the nervous system. Depression is one of the most common non-motor psychoemotional disorders in Parkinson's disease. The aim of the study is to study the specific features of depression in Parkinson's disease. Materials and methods of the study. 120 patients with various clinical forms and stages of Parkinson's disease were enrolled. The control group consisted of 30 age-matched It consisted of patients without PK but with depression. The average duration of the disease was 6.3±4.1 years. We used the HAM-D (Hamilton Depression Rating Scale, HDRS) scale to assess depression in our patients. Results. Depression was more common in women than in men (55.6%). Moderate and severe depression was observed in the tremor form of the disease, as well as moderate and severe depression in stages 2 and 3 compared to stage 1. The data obtained show that the clinical picture of depressive syndrome in Parkinson's disease has its own characteristics. It is characterized by apathetic-abolic and somatovegetative manifestations rather than classic affective symptoms. Conclusion. Observation of depression in Parkinson's disease depends on the duration, clinical forms and stages of the disease.
Keywords: Parkinson's disease, Depression, Form, Phase
Cite this paper: Naimov Olim Yunusovich, Matmurodov Rustambek Jumanazarovich, Muminov Bekzod Askarovich, Jumanazarova Shakhzoda Rustambekovna, Distinctive Features of Depressive Disorders in Parkinson's Disease, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3907-3911. doi: 10.5923/j.ajmms.20251511.31.
1. Introduction
- Parkinson's disease is a chronic, progressive neurodegenerative disease characterized by high rates of mortality and disability, and is the second most common progressive neurological disease after Alzheimer's disease. According to the latest data from the World Health Organization (WHO), "...more than 4 million people worldwide suffer from Parkinson's disease, and this figure is expected to reach almost 9 million by 2030. The incidence of PD varies from 1.5% to 20.5% per 100,000 people per year." Parkinson's disease has been increasing rapidly globally over the past 30 years. This is also due to the aging population and improved medical diagnostics. According to the Global Burden of Disease (GBD) 2021, the number of people living with Parkinson's disease was 11.77 million in 2021. According to the GBD analysis, the global spread of the disease is increasing rapidly. The prevalence has increased 2.5-fold since 1990 [1-4,9-12].It is no secret that in Parkinson's disease, there is a deficiency of neurotransmitters such as dopamine, serotonin, and noradrenaline in the brain. These substances are responsible not only for movement, but also for mood, motivation, and emotional state [8]. Thus, the disease also affects the emotional centers of the brain, which is why patients with PD experience various psycho-emotional disorders. Up to 60% of patients experience various forms of psycho-emotional disorders. Although they are not severe, they have a significant negative impact on the quality of life and daily activities [9]. These disorders often manifest themselves in the form of depression, apathy, and anxiety. They increase as the disease progresses and significantly reduce the patient's quality of life. Early detection and provision of psychological/pharmacological assistance are very important for the patient's overall health [8].Depression is one of the most common psychoemotional symptoms in PD, with various studies reporting a prevalence of 30% to 50% or even higher [1,2,3]. Some studies have reported that 40-60% of patients with PD have depressive symptoms. A study conducted by a group of Chinese scientists to study the prevalence of depression in PD worldwide found the following: According to a meta-analysis of 129 studies, the overall prevalence of depression in patients with PD is 38%. A total of 38,304 patients from 28 countries participated in this study. [Cong S, Xiang C, Zhang S, Zhang T, Wang H, Cong S. Prevalence and clinical aspects of depression in Parkinson's disease: A systematic review and meta analysis of 129 studies].A 2022 study by Portuguese researchers involving more than 10,000 Parkinson's disease patients found a 30.7% prevalence of depressive disorders in Parkinson's disease [11]. A 2025 study titled “The Prevalence of Depression Among Parkinson's Disease Patients in Saudi Arabia: A Cross Sectional Study” reported a prevalence of depression in 84.8% of Parkinson's disease patients.These rates vary depending on demographic, clinical, and research methods. Depression can occur at different stages of the disease in PD. It often occurs early in the disease, even before motor symptoms appear [4]. Early depression is considered part of a common neurochemical and neurodegenerative process in its pathogenesis. Depression is also closely related to the duration of the disease, the severity of motor symptoms, social isolation, and functional limitations.Depression reduces the patient's quality of life, worsens the response to treatment, and worsens the prognosis. Understanding its underlying neurobiological mechanisms is important for the formulation of effective therapeutic approaches. The neurobiological mechanism of depression in Parkinson's disease is multifaceted, several factors are involved: imbalance of neurotransmitters (dopamine, serotonin, noradrenaline); atrophy and hypoactivity in brain structures; inflammation and oxidative stress; genetic and epigenetic changes; disruption of functional connections in the brain. Let's take a look at each of these below.In terms of dysfunction of neurotransmitter systems, we should first discuss the dopaminergic system. The main pathogenetic change in Parkinson's disease is a decrease in dopamine production in the neurons of the substantia nigra. This affects not only the motor systems, but also mood and motivation through the mesolimbic dopamine pathways. Dopamine deficiency causes depressive symptoms such as apathy, anhedonia (lack of mood), and lack of motivation [13]. Next, we will consider the role of the serotonergic system in the genesis of depression. Serotoninergic neurons in the raphe nuclei are also damaged in Parkinson's disease. Serotonin deficiency causes changes such as anxiety, emotional lability, and sleep-wake cycle disruption. PET studies Decreased number of serotonin transporters in PK patients with depression [6-7]. The noradrenergic system also plays an important role in the pathogenesis of PD. Damage to locus coeruleus neurons results in decreased noradrenaline production. This contributes to the pathogenesis of depression by causing symptoms such as fatigue, poor concentration, and weakness [10].Neuroanatomical changes observed in the nervous system were identified in another study conducted to study the causes of depression in PK. According to him, it is shown that there are changes in various structures of the brain in depression in PK:
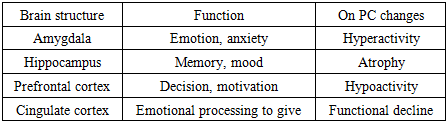 This neuroanatomical structure ar activity and in volume changes depression symptoms causes further increase [17].Another theory of the development of depression in PD is related to oxidative stress in the nervous system. With the activation of the immune system, the amount of cytokines (TNF- α, IL-6) increases in the brain. These biological processes: disrupt synaptic transmission, disrupt the balance of neurotransmitters, reduce neuroplasticity. Oxidative stress also causes neuronal degradation and mitochondrial dysfunction, which is the main biochemical basis of depression.The purpose of the study. Analysis of features of depression in Parkinson's disease according to disease duration, clinical forms, symptoms, age and gender of patients.
This neuroanatomical structure ar activity and in volume changes depression symptoms causes further increase [17].Another theory of the development of depression in PD is related to oxidative stress in the nervous system. With the activation of the immune system, the amount of cytokines (TNF- α, IL-6) increases in the brain. These biological processes: disrupt synaptic transmission, disrupt the balance of neurotransmitters, reduce neuroplasticity. Oxidative stress also causes neuronal degradation and mitochondrial dysfunction, which is the main biochemical basis of depression.The purpose of the study. Analysis of features of depression in Parkinson's disease according to disease duration, clinical forms, symptoms, age and gender of patients. 2. Research Material and Methods
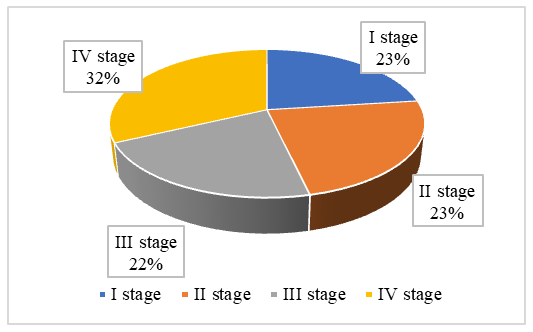
- In order to achieve the goal we set for ourselves and draw conclusions about the tasks set, 120 patients with various clinical forms of Parkinson's disease, who were treated in the inpatient and outpatient settings of the 7th City Clinical Hospital of Tashkent, were enrolled. In order to compare their indicators during the study, a control group of 30 age-matched It consisted of patients without PK but with depression. In our study, all patients with Parkinson's disease were analyzed by age and gender. Among women, the main proportion was in the age group of 40–60 years (57.6%), followed by those aged 60–70 years (19.2%). Also, women under 40 years old accounted for 13.4%, and those over 70 years old accounted for 9.6%. The average duration of the disease was 6.3±4.1 years. Analysis of the duration of the disease in patients showed that the majority (53.3%) were patients who had been living with the disease for 4–6 years. At the same time, 21.0% of patients had a disease duration of 7–10 years, and 15.0% had a disease duration of 1–3 years. A duration of more than 10 years was observed in 11.0% of cases. These data are important in assessing the risk of depression and other neurological disorders in Parkinson's disease. The diagnosis of Parkinson's disease was made based on the criteria developed by Postuma RB, Berg D., Stern M., Poewe W., Olanow CW, Oertel W. and co-authors (MDS clinical diagnostic criteria for Parkinson's disease, 2015). The Hoehn & Yahr scale (1967, modified in 2001) was used to determine the stages of Parkinson's disease [1]. According to this scale, the smallest number of patients was identified in stage I of the disease - 13 patients (10.8%). Stages II and III the number of patients is almost are the same, 48 (40%) and 45 (37.5 %) respectively In the IV stage and 14 (11.6 %) patients observed. V stage patients record It was not done.All patients underwent a standard clinical and neurological examination, during which tremor, akinetic-rigid and mixed variants of Parkinson's disease were identified. The largest number of patients was diagnosed with the tremor variant of Parkinson's disease - 52 (43.3%). The akinetic-rigid variant was observed in 38 patients (31.7%), and the mixed variant in 30 (25.0%). These data indicate that the tremor variant is the most common clinical form in our study. This is also consistent with the literature, since the tremor form is the classic and most common clinical manifestation of Parkinson's disease [8]. At the same time, the significant proportion of akinetic-rigid and mixed variants indicates that the disease has a variety of clinical features and requires an individual approach to each patient. These data are presented in the table below.Clinical-neurological examination and neuropsychological research methods were performed on all patients. We used the Hamilton Depression Rating Scale (HAM-D) to assess depression in our patients. The HAM-D is one of the most widely used scales in clinical trials and practice to assess the effectiveness of treatment, as well as to determine the severity of depression. It allows the clinician to assess the nature and severity of mood disorders in patients. The scale consists of 21 items, but only the first 17 items are used to calculate the result [5]. The questions cover a variety of symptoms: depressed mood, guilt, suicidal ideation, sleep disturbances, agitation, and somatic symptoms. The scale can be used in a variety of clinical and research settings. It is suitable both as a one-time assessment tool and to monitor the dynamics of symptoms during treatment. The sleep-related items (4–6) cover insomnia before bedtime, difficulty falling asleep during the night, and inability to get back to sleep in the morning. Other items are indirectly related to sleep difficulties, covering fatigue, psychomotor retardation, and somatic symptoms. There are also longer, shorter, and adapted versions of the scale for seasonal affective disorder.Modern statistical methods were used to process and analyze the obtained data. Clinical and psychometric indicators obtained from patients were entered into a special electronic database, and statistical analysis was performed using SPSS (Statistical Package for the Social Sciences, version XX) and MS Excel programs. The compliance of the data with a normal distribution was checked using the Shapiro–Wilk test. For indicators with a normal distribution, the mean value (M) was expressed as ± standard deviation (SD). In cases of deviation from normal distribution, the data were presented as the median (Me) and interquartile range (Q25–Q75).
3. Results
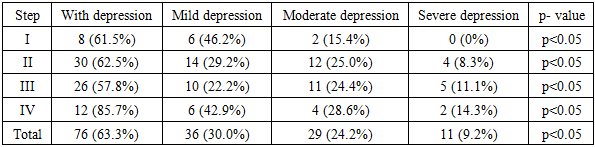
- A total of 120 patients with Parkinson's disease (PD) underwent clinical and neuropsychological evaluation within the framework of the study. The general data showed that the distribution of patients by age and gender covered various categories, with the majority of them being in the age range of 40–70 years. The study revealed a high prevalence of depressive disorders in patients with PD. was recorded. A total of 76 patients (63.3%) had a depressive syndrome.When analyzing the gender distribution of patients with depression, it was found that 42 (55.3%) of them were women, and the remaining 34 (44.7%) were men. This indicates that depressive disorders in Parkinson's disease are relatively more common, especially among women. At the same time, the fact that depression is also common in male patients means that it is a significant clinical problem in both sexes. Thus, the analyses conducted showed that depression is widespread in patients with Parkinson's disease, especially in women, and its clinical significance is high.Parkinson's disease duration the spread of depression with mutual dependence The study is of clinical importance. The analysis showed that among patients with an initial duration of 1–3 years, depression was relatively rare - 18 (15%). The highest rate was observed in the group of patients with a duration of 4–6 years, of whom 64 (53.3%) were diagnosed with depression (p<0.01). In recent years, this rate has decreased: depression was noted in 25 patients (21%) with a duration of 7–10 years, and in 13 patients (11%) with a duration of more than 10 years. Thus, the data obtained show that depression is most common in the middle stage of Parkinson's disease (4–6 years), and then there is a tendency to decrease with increasing disease duration, Table 1.This is probably due to the fact that neurodegenerative processes, dopaminergic and serotonergic imbalances, and psychoemotional changes peak in the middle stage of the disease. Later, part of the depressive syndrome becomes less pronounced in the clinical picture due to the "shutdown" of motor and cognitive disorders or adaptation mechanisms. The HAM-D (Hamilton Depression Rating Scale, HDRS) scale was used to assess the severity of depressive symptoms in patients with Parkinson's disease.The analysis found that as the stages of Parkinson's disease according to the Hoehn & Yahr classification increase, the prevalence of depression increases proportionally.Taken to the information according to, 120 people with depression syndrome observed in 76 patients (63.3%), Fig. 1.
 | Figure 1. Parkinson's disease to the stages looking at depression spread |
|
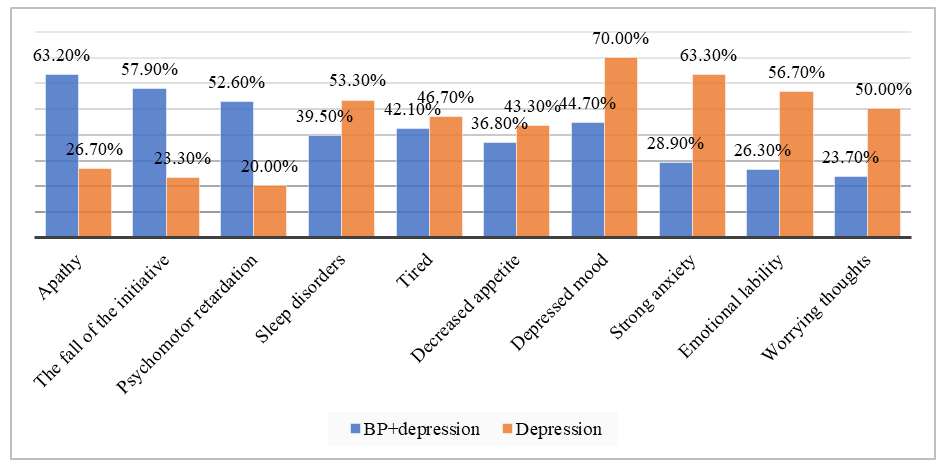 | Figure 2. Clinical features of depressive syndrome |
4. Conclusions
- The occurrence of depression in Parkinson's disease has its own characteristics, with patients with an average disease duration of 4-6 years exhibiting more moderate and severe depressive disorders in the tremor form than in the akinetic-rigid and mixed forms of the disease, and in the early stages than in the early stages. When comparing patients by gender, depressive disorders predominate in women compared to men in all cases.