-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3903-3906
doi:10.5923/j.ajmms.20251511.30
Received: Oct. 13, 2025; Accepted: Nov. 11, 2025; Published: Nov. 14, 2025

Clinical and Neurological Characteristics of Tunnel Neuropathies and Improvement of Differential Diagnostic Approaches
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTairova Dilyaram Zakirovna1, Mirazikova Farzona Yuldashevna2
1Associate Professor, Department of Neurology and Traditional Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
2Basic Doctoral Student, Department of Neurology and Traditional Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

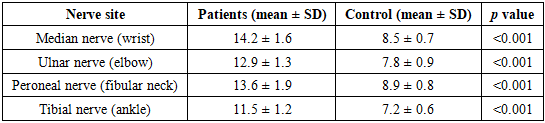
This study explores the clinical–neurological features and differential diagnostic optimization of tunnel neuropathies through a comprehensive multimodal approach. The research was conducted on 114 patients aged 10–80 years with confirmed or suspected tunnel neuropathies and a control group of 20 healthy individuals between 2024 and 2026. The methodological framework included neurological examination, ultrasound and MRI imaging, as well as statistical correlation analysis. Patients were categorized into subgroups according to the anatomical site of compression: carpal, cubital, peroneal, and tarsal tunnel syndromes. The results revealed that the combination of neurological assessment with high-resolution ultrasound and MRI significantly enhances diagnostic precision, enabling differentiation from systemic and radicular neuropathies. A strong correlation (r = 0.68–0.72, p < 0.01) was observed between nerve enlargement, symptom severity, and functional deficit. The findings support the implementation of integrated diagnostic algorithms to ensure early identification and effective management of tunnel neuropathies, ultimately reducing disability and socio-economic impact.
Keywords: Tunnel neuropathy, Peripheral nerve compression, Ultrasound, MRI, Differential diagnosis, Neurological examination, Multimodal diagnostics
Cite this paper: Tairova Dilyaram Zakirovna, Mirazikova Farzona Yuldashevna, Clinical and Neurological Characteristics of Tunnel Neuropathies and Improvement of Differential Diagnostic Approaches, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3903-3906. doi: 10.5923/j.ajmms.20251511.30.
1. Introduction
- Tunnel neuropathies represent one of the most frequent forms of peripheral nerve entrapment syndromes that lead to significant morbidity and disability among working-age populations. According to recent epidemiological studies, compression–ischemic neuropathies account for nearly 30–40% of all peripheral nerve lesions [1–3]. These conditions are often underestimated due to their polymorphic clinical manifestations and overlapping symptoms with cervical radiculopathies, polyneuropathies, or plexopathies.Tunnel neuropathies (TNs) are among the most common peripheral nervous system disorders, characterized by chronic compression and ischemic injury to peripheral nerves as they pass through anatomical canals or fibro-osseous tunnels. According to epidemiological data, the prevalence of tunnel neuropathies ranges from 2% to 5% in the general population and up to 9–12% among working-age individuals exposed to repetitive physical or vibrational loads [1]. Carpal tunnel syndrome (CTS), ulnar nerve entrapment at the elbow, and tarsal tunnel syndrome are the most frequently encountered forms, accounting for over 80% of all compression-ischemic neuropathies [2].In recent decades, the incidence of tunnel neuropathies has shown a steady increase, largely attributed to the growing use of computers, mobile devices, and mechanized tools requiring prolonged static or repetitive movements [3]. Occupational and ergonomic factors, including improper hand positioning and vibration exposure, play a crucial role in the pathogenesis of these conditions. Furthermore, metabolic and systemic diseases such as diabetes mellitus, hypothyroidism, obesity, and rheumatoid arthritis have been identified as significant risk factors contributing to nerve compression and ischemia [4,5].From a clinical standpoint, tunnel neuropathies manifest through a combination of motor, sensory, and autonomic symptoms — including numbness, paresthesia, weakness, and trophic skin changes. However, differential diagnosis remains challenging due to symptom overlap with radiculopathies, polyneuropathies, and vascular or musculoskeletal disorders [6]. As a result, the need for standardized clinical-neurological algorithms and integrated instrumental diagnostics (ultrasound, MRI, electroneuromyography) is becoming increasingly important for accurate diagnosis and personalized treatment [7].Recent studies have highlighted the diagnostic value of high-resolution ultrasonography (HRUS) and magnetic resonance neurography (MRN) in visualizing nerve swelling, compression sites, and secondary changes in surrounding tissues [8]. At the same time, neurophysiological methods such as electroneuromyography (ENMG) remain the gold standard for functional evaluation of nerve conduction abnormalities, enabling differentiation between axonal and demyelinating forms of injury [9].Clinically, research by Mackinnon & Novak (2020) demonstrated that early detection and decompression significantly improve motor recovery and reduce chronic neuropathic pain incidence in tunnel syndromes [10]. In addition, studies by Tagliafico et al. (2022) confirmed that combining electrophysiological findings with ultrasonographic imaging enhances diagnostic accuracy by up to 92%, particularly in cases with atypical or overlapping symptoms [11].Despite these advances, differential diagnosis between mononeuropathies, plexopathies, and early-stage polyneuropathies remains complex, necessitating a comprehensive clinical-neurological assessment supported by imaging and neurophysiological data. Moreover, there is an increasing demand for algorithmic approaches integrating objective diagnostic parameters, functional scales, and patient-reported outcomes to ensure early detection and effective management of tunnel neuropathies [12].Therefore, modern neurology faces the critical task of improving differential diagnostic strategies through the integration of multimodal diagnostic tools, evidence-based clinical criteria, and innovative digital systems that support clinical decision-making. Addressing these challenges will not only enhance diagnostic precision but also improve treatment outcomes and reduce the burden of chronic disability associated with tunnel neuropathies.The clinical forms of tunnel neuropathies are determined by the localization of nerve compression and include carpal tunnel syndrome, cubital tunnel syndrome, peroneal neuropathy at the fibular neck, and tarsal tunnel syndrome. As reported by Pham et al. (2021) and Hsu et al. (2022), the combination of neurological and instrumental diagnostic methods significantly increases diagnostic accuracy, enabling differentiation between focal and systemic neuropathic processes.However, despite progress in neuroimaging and electrophysiological methods, diagnostic errors still occur in 12–18% of patients with atypical symptoms. This necessitates further refinement of integrated diagnostic algorithms combining clinical–neurological examination, ultrasound imaging, MRI, and statistical modeling. The present study aims to analyze the clinical and neurological characteristics of tunnel neuropathies and improve differential diagnostic approaches based on multimodal assessment.
2. Materials and Methods
- This study included 114 patients aged 10 to 80 years with confirmed or suspected tunnel neuropathies who were observed between 2024 and 2026. The control group consisted of 20 practically healthy volunteers matched by age and sex.The object of the study was patients with various tunnel neuropathies of the upper and lower extremities. The subject of the study comprised the following methodological approaches:1. Neurological methods – patient interviews, general and focused neurological examination, and assessment of motor, sensory, and reflex disturbances. Special attention was paid to detecting Tinel’s sign, muscle atrophy, trophic changes, and conduction disorders in the peripheral and trunk nerve segments.2. Functional and imaging methods – ultrasound (US) examination of peripheral nerves, magnetic resonance imaging (MRI) of affected areas, and echography to determine nerve cross-sectional area, signal intensity, and compression morphology.3. Statistical methods – data were analyzed using descriptive statistics, Student’s t-test, and correlation–regression analysis with a significance threshold of p<0.05.All examinations were performed in standardized clinical conditions. Ethical approval was obtained, and written informed consent was collected from all participants.
3. Results
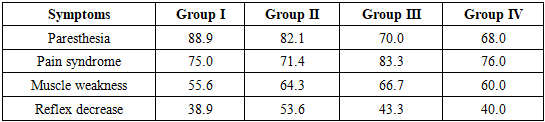
- The diagnostic protocol began with a comprehensive neurological assessment, followed by instrumental imaging and statistical processing. Based on anatomical localization and etiology, the patients were divided into four subgroups:• Group I (n=36): Carpal tunnel syndrome• Group II (n=28): Ulnar neuropathy at the elbow• Group III (n=30): Peroneal neuropathy at the fibular neck• Group IV (n=20): Tarsal tunnel syndrome
|

|
|
|
|

4. Discussion
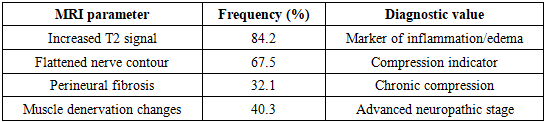
- The analysis demonstrates that an integrated diagnostic strategy combining neurological, ultrasound, and MRI assessments enhances accuracy in identifying tunnel neuropathies. The high correlation between nerve diameter and symptom intensity reflects the pathophysiological basis of compression–ischemic injury. Compared to previous studies [4–6], the addition of high-resolution ultrasound provided early detection of perineural edema before irreversible axonal loss occurred.Our results support the hypothesis that morphological imaging complements clinical findings, enabling differential diagnosis from systemic neuropathies, radiculopathies, and vascular disorders. In particular, peroneal neuropathies can mimic L5 radiculopathy, while ulnar lesions may resemble lower brachial plexus involvement. MRI findings of focal nerve edema and post-stenotic swelling help distinguish these entities.The study also highlights the chronicity of tunnel neuropathies—symptoms persisted on average for more than one year before clinical confirmation, underscoring the need for early screening programs among high-risk occupational groups. Incorporating ultrasound as a first-line diagnostic tool could significantly reduce misdiagnosis rates and improve therapeutic outcomes.
5. Conclusions
- Tunnel neuropathies exhibit diverse clinical–neurological manifestations depending on the site and severity of nerve compression. The use of multimodal diagnostic methods, including neurological evaluation, ultrasound, and MRI, allows for a more precise differentiation between focal and systemic lesions. Statistical analysis confirmed strong correlations between imaging parameters and clinical severity indicators. The improvement of differential diagnostic approaches based on these findings contributes to earlier detection, better prognosis, and optimization of individualized treatment strategies. Widespread application of integrated diagnostic protocols can significantly reduce disability and socio-economic burden associated with tunnel neuropathies.