-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3859-3863
doi:10.5923/j.ajmms.20251511.22
Received: Sep. 10, 2025; Accepted: Oct. 3, 2025; Published: Nov. 7, 2025

Improving Diagnosis and Prognosis in Hippocampal Sclerosis Epilepsy Through a Multimodal Model
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSultonova Dilbar Azamat kizi, Azizova Ra’no Bahodirovna
Neurology and Medical Psychology Department, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Sultonova Dilbar Azamat kizi, Neurology and Medical Psychology Department, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The diagnosis of Mesial Temporal Lobe Epilepsy (MTLE) with hippocampal sclerosis (HS) involves a combination of neuroimaging, biomarker analysis, and clinical evaluation. MTLE is the most common form of temporal lobe epilepsy, often associated with HS, which is characterized by neuronal loss and gliosis in the hippocampus. Accurate diagnosis is crucial for effective treatment, often involving surgical intervention. This study aimed to develop and validate a multimodal model for the diagnosis and prognostic evaluation of mesial temporal lobe epilepsy with hippocampal sclerosis.All patients underwent cognitive evaluation with the MoCA and HADS scales, video-EEG monitoring, MMP-9 analyses, and brain MRI in accordance with the HARNESS protocol.Four models were developed on the basis of the integrated analysis of clinical, cognitive, neurophysiological, and biochemical indicators, providing a structured framework for the diagnosis and prognostic evaluation of MTLE-HS.
Keywords: Mesial temporal sclerosis, Mesial temporal loe epilepsy with hippocampal sclerosis, Diagnostic model, Matrix metalloproteinase-9, Biomarker
Cite this paper: Sultonova Dilbar Azamat kizi, Azizova Ra’no Bahodirovna, Improving Diagnosis and Prognosis in Hippocampal Sclerosis Epilepsy Through a Multimodal Model, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3859-3863. doi: 10.5923/j.ajmms.20251511.22.
Article Outline
1. Introduction
- Mesial temporal lobe epilepsy (MTLE) is the most prevalent and treatment-resistant form of focal epilepsy, representing a major clinical challenge worldwide [1-4]. A substantial proportion of patients with chronic, pharmacoresistant seizures present with hippocampal sclerosis (HS) as the underlying substrate [5,6]. HS is pathologically characterized by selective neuronal loss, gliosis, and synaptic reorganization within the hippocampal formation, particularly in the CA1 and CA3 subfields [7-9]. These structural alterations not only contribute to epileptogenesis but also underlie the cognitive and psychological comorbidities frequently observed in affected patients [10].Despite significant advances in diagnostic approaches, the reliable identification and prognostic stratification of MTLE-HS remain challenging [11]. Traditional methods such as seizure semiology, long-term video-EEG monitoring, and conventional MRI provide valuable information, yet often fail to fully capture the heterogeneity of disease presentation and outcome [12]. The implementation of standardized MRI protocols, most notably the HARNESS (Harmonized Neuroimaging of Epilepsy Structural Sequences) protocol, has improved the sensitivity and reproducibility of structural imaging in detecting hippocampal sclerosis. HARNESS MRI provides high-resolution and standardized acquisition across centers, enabling more accurate identification of subtle hippocampal changes [13]. However, while neuroimaging remains indispensable, it must be complemented by other modalities to achieve reliable diagnostic and prognostic precision. Beyond imaging, cognitive and psychological assessment offers additional insights into disease burden. Patients with MTLE-HS commonly experience deficits in memory, executive functioning, and emotional regulation, all of which significantly affect quality of life [14,15]. Instruments such as the Montreal Cognitive Assessment (MoCA) and the Hospital Anxiety and Depression Scale (HADS) allow systematic evaluation of these domains [16]. Yet, these measures have rarely been incorporated into integrated predictive models of MTLE-HS.Emerging biochemical biomarkers provide another promising avenue. Among them, matrix metalloproteinase-9 (MMP-9) has gained increasing attention due to its involvement in extracellular matrix remodeling, blood–brain barrier disruption, and neuroinflammatory processes—all of which are implicated in epileptogenesis and seizure recurrence [17,18]. Elevated serum MMP-9 levels have been observed in patients with temporal lobe epilepsy, but its potential as part of a multimodal diagnostic and prognostic framework remains insufficiently explored [5,19].Considering the multifactorial nature of MTLE-HS, there is a strong rationale for developing multimodal approaches that integrate clinical, cognitive-psychological, electrophysiological, biochemical, and advanced neuroimaging data. Such models have the potential not only to improve diagnostic accuracy but also to stratify patients according to risk, predict disease course, and guide treatment strategies, including surgical interventions.In this study, we systematically assessed patients with MTLE-HS using a comprehensive battery comprising clinical-semiological evaluation, long-term video-EEG monitoring, standardized cognitive and psychological testing, biochemical assays with MMP-9 measurement, and brain MRI performed in accordance with the HARNESS protocol. Based on the integrated analysis of these multidimensional datasets, we developed and validated a multimodal prognostic model and diagnostic algorithm designed to enhance diagnostic precision and individualized prognostication in MTLE-HS.
2. Materials and Methods
- This analytical cross-sectional study was conducted between 2023 and 2025 at two clinical sites: the Department of Neurology, Clinical Hospital No. 1 of Tashkent State Medical University (TSMU), and the Central District Polyclinic of Khatirchi. A purposive sampling strategy was applied, and a total of 88 participants were enrolled. Subjects were divided into three groups: the main group (n = 30), consisting of patients diagnosed with mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS) according to the International League Against Epilepsy (ILAE) 2017 criteria; the comparative group (n = 36), including patients with other forms of epilepsy but without hippocampal sclerosis on MRI; and the control group (n = 22), comprising neurologically healthy individuals without epilepsy or structural brain pathology.All participants underwent structured clinical and semiological evaluation. Cognitive and psychological status was assessed using the Montreal Cognitive Assessment (MoCA) and the Hospital Anxiety and Depression Scale (HADS). Long-term video-EEG monitoring was performed for all patients in the epilepsy groups. Brain MRI was carried out in accordance with the standardized HARNESS (Harmonized Neuroimaging of Epilepsy Structural Sequences) protocol to evaluate structural alterations, particularly hippocampal sclerosis. Peripheral venous blood samples were collected from all participants via the antecubital vein, and serum was analyzed for biochemical marker, matrix metalloproteinase-9 (MMP-9).All data were statistically processed using the DataTab online platform. Based on the results of statistical analysis, four analytical modules were constructed: clinical-semiological, cognitive-psychological, EEG, and biochemical.
3. Results and Discussion
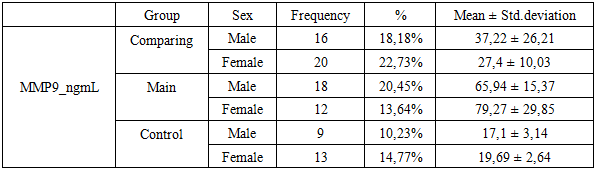
- The alterations of the MMP-9 biomarker in mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS) and its relationship with age and sex factors were investigated. The analysis demonstrated significant intergroup and sex-related differences in MMP-9 levels among patients with MTLE-HS. In the main group, the mean serum MMP-9 concentration was 71.27 ± 22.82 ng/ml, which was markedly higher compared with both the comparative group (patients with MTLE without hippocampal sclerosis) and the control group (healthy individuals), where the mean values were 31.76 ± 19.32 ng/ml and 18.63 ± 3.07 ng/ml, respectively (Table 1).
|
|
|
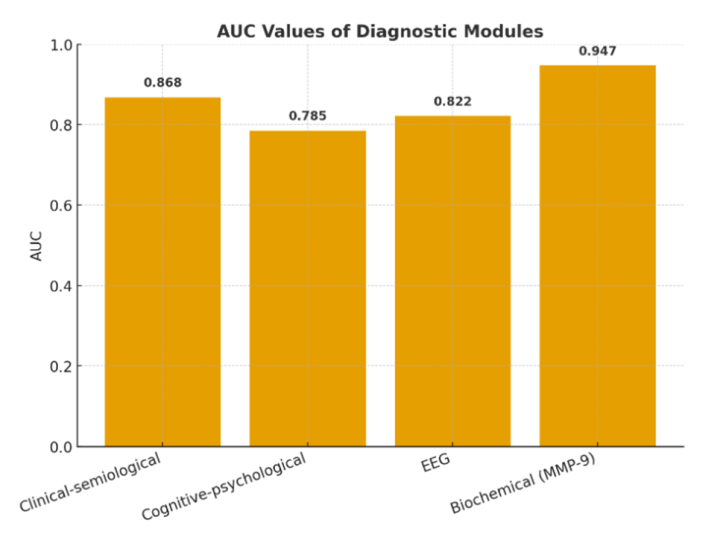 | Figure 1. AUC values of diagnostic modules |
4. Conclusions
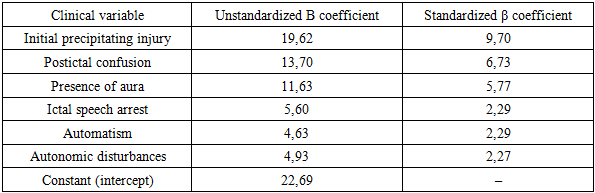
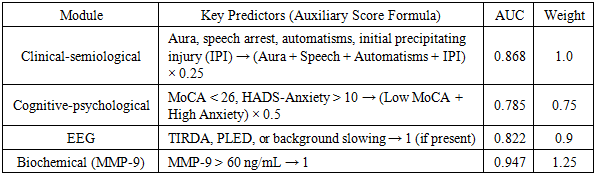
- This study demonstrates that a multimodular diagnostic model integrating clinical semiological features, cognitive-psychological indicators, EEG abnormalities, and the biochemical biomarker MMP-9 offers a systematic and reliable approach to the early identification of mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS). Each module contributes an independent auxiliary score, with diagnostic performance validated by AUC indices and statistically significant predictors. The weighted composite scoring system enables precise risk stratification into low, moderate, and high categories, each associated with tailored recommendations for further diagnostic testing and individualized treatment planning. Beyond improving diagnostic accuracy, the modular framework provides practical advantages for clinical practice by optimizing resource utilization, facilitating earlier detection, and supporting personalized therapeutic strategies. These findings underscore the potential of this integrated approach to improve outcomes in patients with MTLE-HS and highlight the need for validation in larger, multicenter cohorts.
ACKNOWLEDGEMENTS
- The authors sincerely thank all patients and their families for their participation and cooperation in this study. We also acknowledge the valuable contributions of the clinical and laboratory staff who assisted in data collection and analysis. Special appreciation is extended to our colleagues at the Department of Neurology and the Neurophysiology Unit for their technical support and constructive feedback during the course of this research.