Ruziboev D. R.1, Djumaniyazova M. D.2
1National Centre for Rehabilitation and Prosthetics of People with Disabilities in Tashkent, Uzbekistan
2Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Ruziboev D. R., National Centre for Rehabilitation and Prosthetics of People with Disabilities in Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: Currently, the global need for knee arthroplasty is growing dramatically due to the increasing prevalence of knee arthritis. According to prognosis, by 2030, the number of primary surgeries of this type will have reached 1.26 million procedures. Measures to achieve a full-fledged result of the operation include adequate, individual social and vocational rehabilitation, especially relevant for patients of working age. Objectives: To evaluate the effectiveness of social and vocational rehabilitation in patients of working age following knee endoprosthetics. Materials and methods: The study involved 235/147 patients (73 males, 74 females) who underwent knee endoprosthetics. The effectiveness of restoring the static-dynamic function, as well as the supportive ability of the leg, was evaluated by X-ray and electromyography in the following periods: 3, 6, and 12 months after surgery. The improvement of the medical, social and professional condition of the patients, as well as the quality of their lives after surgery were analyzed on the basis of outpatient cards, medical examination certificates, and conclusions of the medical and social expert commission. The obtained information was evaluated according to the developed point scale. Results: The criteria for determining the employment opportunities of patients with an endoprosthesis have been developed. They included the findings on the static-dynamic function of the operated leg; its supportive capacity was of particular importance. Both of them ensure the activation of patients after total knee endoprosthetics. Depending on the compensation of the static-dynamic function of the operated leg (legs), three categories of patients were identified; for each of them, a number of types of work activities were proposed after the rehabilitation. Conclusions: Early comprehensive, individual, continuous rehabilitation, elaborated taking into account the pathology of other parts of the musculoskeletal system, allowed an increase in the share of patients with high efficiency of rehabilitation after total knee endoprosthetics and reduced the number of cases with moderate effectiveness of rehabilitation in this category of patients. A timely assessment of the disability of patients after total knee endoprosthetics, including the emerging changes in the static-dynamic function and supportability of the operated leg, pathology of adjacent joints, and other parts of the musculoskeletal system, increased the number of patients continuing their professional activities after the rehabilitation measures proposed to them.
Keywords:
Socio-professional rehabilitation, Efficiency, Endoprosthetics, Knee joint
Cite this paper: Ruziboev D. R., Djumaniyazova M. D., Evaluation of Effectiveness of Medical, Social and Vocational Rehabilitation After Total Knee Endoprosthetics in Patients of Working Age, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3835-3840. doi: 10.5923/j.ajmms.20251511.17.
1. Introduction
Knee endoprosthetics (KE) is a widely used effective method of treating degenerative diseases of this joint. Currently, the global need for KE is increasing dramatically, primarily due to the growing prevalence of knee arthritis. According to prognosis, by 2030, the number of primary KE procedures will increase by 85%, reaching 1.26 million procedures [1,2]. According to the literature, after the primary KE, various functional disorders may occur when complex rehabilitation measures are not followed in the postoperative period [3,4,5]. According to R.V. Petrova et al. (2022), revision interventions are required in 60-80% of cases during the first 2-5 years after primary surgery [6]. Many scientific papers have been devoted to the rehabilitation of patients after total KE (TKE), but few of them reflect the features of social and vocational rehabilitation of patients of working age.
2. Purpose of the Research
The study objectives were to increase the effectiveness of the complex of rehabilitation measures associated with TKE and to assess the changes in the quality of life of patients with osteoarthritis after endoprosthesis achieved through socio-vocational rehabilitation.
3. Materials and Methods
We observed 147 patients (73 males, 74 females) with knee osteoarthritis who were treated at the clinic of the National Center for Rehabilitation and Prosthetics of People with Disabilities and Traumatology Department of Multidisciplinary clinic of the Center for the development of the qualification of medical workers from 2016 to 2023. Out of the total number of patients, 147 were of working age; the working age in Uzbekistan is 16-60 y for men and 16-55 y for women. All patients were divided into 2 groups: the main group (n=75) and the control group (n=72). The main group patients underwent surgery according to our proposed method and received rehabilitation measures, while the control group patients received traditional surgical treatment and did not participate in the rehabilitation program (Fig. 1.). | Figure 1. The number of male and female patients |
All patients underwent the following diagnostic tests: biomechanical (basometry and podometry), electromyographic and radiographic, since these indicators are the main ones for determining the static-dynamic function (SDF) of the operated limb and walking mode, as well as for assessing the quality of life of patients in the postoperative period.
4. Results and Discussion
In the course of the research, the results of TKE in 147 patients and the outcomes of their medical, social, and vocational rehabilitation were analyzed. In addition, we studied the leg SDF to evaluate the dynamics of the operated knee disability, postoperative functions, and patient work capacity since the degree of the SDF recovery associates with frequency, complexity and duration of rehabilitation.In the diagnosis of knee joint pathology, an X-ray examination is the main objective method that gives physicians the information to determine the tactics and results of surgical treatment.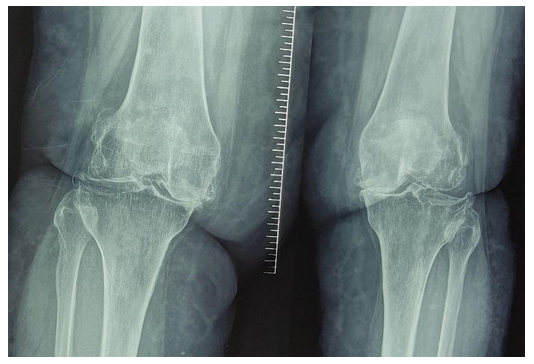 | Figure 2. Patient S., female, born in 1965. Radiography of the knee in direct and lateral projection before surgery (osteoporosis, knee deformity) |
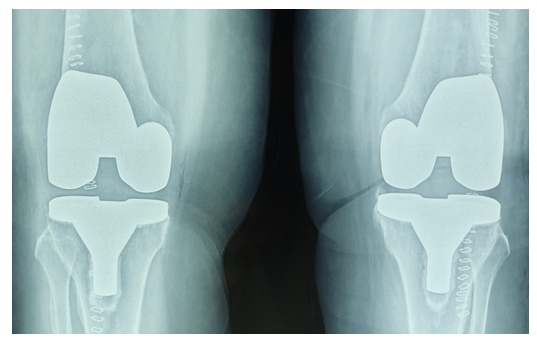 | Figure 3. The same patient after TKE (Total knee arthroplasty) |
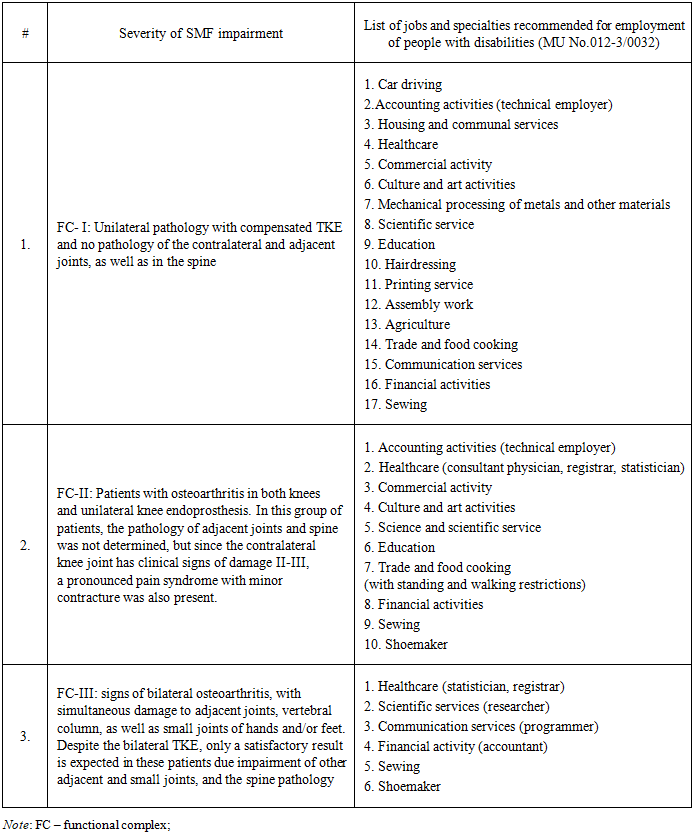
Electromyographic examination was conducted to study the muscular bioelectric activity of the leg (legs) to identify a contracture in the knee, the supportive capacity of the leg in patients with osteoarthritis and a decrease in muscle tone of the thigh which played a major role in the restoration of the SDF after surgery. The tension of the following muscles was checked: m.m. vastus medialis, lateralis and rectus, medial muscle group m. semimembranosus, muscle group m. biceps, as well as shin muscles m.m. tibialis anterior, gastrocnemius on both sides of both damaged and healthy legs synchronously.Social rehabilitation programSocial rehabilitation of disabled people is known to include comprehensive rehabilitation measures to ensure socio-environmental orientation and social adaptation aimed at restoring the ability to self-care, proper orientation, communication, behavior control, learning, etc. Legal consultations play an important role in the psychological rehabilitation of this category of patients.The specific features of organization and management of medical and social rehabilitation measures require active and conscious participation of patients after TKE in their implementation. The patients need to be confident in the beneficial and safe impact of the recommended individual rehabilitation program, which is created taking into account the underlying and concomitant diseases, the degree of damage to the leg SDF, age, marital status, as well as educational background and social status. However, as our practice shows, most patients do not know much about the problems of behavior and the lifestyle that may appear after TKE. The lack of necessary and reliable information contributes to low motivation of this category of patients to restore, strengthen and maintain their health through their own efforts. One of the important indicators of TKE results is the satisfaction of patients with the knee functions [8]. The degree of patient satisfaction can be assessed in two aspects: the determinants of satisfaction and the components of achieving satisfaction by patient. The first of them include age, gender, personality characteristics, expected TKE results, concomitant medical and psychiatric diseases as well as the severity of the patient's arthropathy that has led to TKE. The components of achieving satisfaction include all the processes and technical aspects of TKE (anesthesiological and surgical features, type of implants and postoperative rehabilitation). Sometimes the results reported by the surgeon and the patient are not comparable, so detailed discussion and explanations before surgery will reduce the unreasonable expectations of the patient after TKE [9]. Determining the degree of patient satisfaction before and at months 3 and 6 after TKE helps identify factors that may contribute to the emergence of dissatisfaction. These findings included the degree of patient satisfaction on the 5-point Likert satisfaction scale (R. Likert) [10]. Data adjustments were carried out according to the following parameters: age, gender, body mass index (BMI), Charlson Comorbidity Index (CCI) [11], marital status, smoking, education. An increased BMI, a higher CCI, a higher Oswestry Disability Index (ODI) [12] and an increase in other painful conditions in the joints of the leg were largely associated with the patient's dissatisfaction. Our findings agree with the data of other researchers that a higher level of dissatisfaction is observed in young patients with a low level of education [13]. Vocational rehabilitation programIn a complex of rehabilitation measures, undoubtedly, an important role is played by the vocational rehabilitation of TKE patients of working age. The patients need to be informed about recommended types of work. If it is not possible to return to their previous occupation, they are offered vocational training, assistance in adapting to the professional and industrial scope of activities.As a part of the scientific research, the criteria for determining the employment opportunities of patients following endoprosthetics have been developed. It includes the SDF of the operated limb; its supportive capacity is of particular importance, since they ensure the activation of patients after TKE. Depending on the compensation for the SDF of the operated lower leg (legs), three patient groups were made; for each of them a number of types of work were proposed. We have developed and obtained the patent for a software program (DGU No. 12980) to determine the ability to work for patients after TKE depending on the SDF of the operated leg.We have proposed the criteria for determining the disability of patients following TKE, depending on the violation of the limb SDF and possible types of work (Table 1).Table 1. Types of work after knee arthroplasty depending on the SDF of the operated leg
 |
| |
|
The Table demonstrates the effect of severity of osteoarthritis and SMF impairment on the number of job opportunities for TKE patients: the job lists for FC- I is more than twice longer than for FC- III (17 vs 6).The obtained clinical outcomes in the main and control groups were compared: in the main group of 120 patients, at month 3 after the TKE 21 patients scored 46.5 points, which is interpreted as “moderate rehabilitation effectiveness”. These patients presented the following complaints: flexion contracture with limited movement and pain in the operated joint, the need to use a cane when moving, significant difficulties in household self-care, and emotionally labile psychological condition. In 42 patients, more than 53 points were registered, and their result was assessed as "good rehabilitation effectiveness". These patients complained of the following: minor pain syndrome and flexor contracture < 20o of the normal value. 57 patients had no complaints about the operated joint, they scored an average of 66.8 points and their result was assessed as "high efficiency of rehabilitation”.After the repeated course of rehabilitation at month 6 after the surgery, one patient had complaints related to the operated joint. He had flexor contracture, pain syndrome in the operated joint, as well as difficulties in self-care. On average, he scored 45.3 points, and this result was rated as "moderate rehabilitation effectiveness". The following indicators were obtained in 18 other patients: flexor contracture was below normal to 10° that gave 55.8 points on the point scale, which was assessed as "good rehabilitation effectiveness". The remaining 101 patients did not present any complaints related to the operated joint. The result of their TKE was estimated at 68 points, i.e. "high efficiency of rehabilitation".In the control group of 115 patients, at month 3 following TKE, 29 patients scored 46.5 points on a point scale; this result was assessed as "moderate rehabilitation effectiveness". These patients presented the following problems: flexion contracture with limited movement and pain in the operated joint, the need to use a cane when moving, significant difficulty in household self-care, emotionally labile psychological condition. "Good rehabilitation efficiency" was noted in 62 patients (53 points). These patients presented the following complaints: minor pain syndrome and flexor contracture less than normal up to 20°. Twenty-four patients had no complaints related to the operated joint. They scored an average of 66.8 points, and their result was rated as "highly effective rehabilitation".After the second course of rehabilitation 6 months after the operation, 5 patients had complaints related to the operated joint, they had flexion contracture, pain syndrome in the operated joint, difficulties in household self-care. The condition of these patients was defined as "moderate rehabilitation efficiency" (average 45.3 points). The following outcomes were obtained in 39 patients after the repeated course of rehabilitation: flexion contracture is below normal to 10° that gives 55.8 points on the point scale, which was assessed as "good rehabilitation effectiveness". The remaining 71 patients did not have any complaints related to the operated joint, they scored 68 points on the point scale, and their result was assessed as "highly effective of rehabilitation".After the early, comprehensive, individual rehabilitation covering medical, social and vocational aspects of rehabilitation, the main group patients demonstrated the following proportion of efficiency of rehabilitation: high efficiency was registered in 91.7% of cases, good efficiency - in 8.2% of cases, and in 0.4% of cases, the effectiveness of rehabilitation was moderate.In the control group, the patients who did not use early, individual and comprehensive rehabilitation technologies, the following results were obtained: in 79.7% of cases, the effectiveness of rehabilitation was high, in 17.9% of cases, it was good, and in 2.3% of cases, the effectiveness of rehabilitation was moderate.Thus, the proposed method of early, comprehensive, individual, continuous medical, social and vocational rehabilitation has enlarged the number of patients with high rehabilitation efficiency by 12% and has made the proportion of patients with moderate efficiency 1.9% lower than in the control group. The criteria developed by us to determine TKE patient's ability to work include: the general condition of the patient, taking into account concomitant pathologies and involvement of other parts of the ODS in the pathology; the degree of SDF disorder, the supportive ability of the operated leg, and the degree of their compensation; vocational activity, taking into account educational status, harmful factors that affect the outcome of the surgery, as well as the patient’s social status; the need for outside help as well as ability of using public transport.Function Control - I: in case of a slight disorder of the SDF and the supportive ability of the operated leg, the job capacity prognosis is favourable. With such disorders, all types of jobs may be offered (except for those with excessive physical exertion) and light types of sports exercises, e.g., walking, swimming, cycling, non-intensive running. With such indicators, the patients do not meet the criteria for disability. FC – II: moderate impairment of the SDF and the supportive ability of the operated leg, minor restrictions in work and sports, which do not prevent working under conditions that require walking and standing for a long time. Working conditions should provide the opportunity to change body posture and avoid prolonged stress with alteration to sedentary work. Patients of this category are allowed to walk and swim, since these sports do not affect the functions of the operated joint.FC –III: marked disorder of the SDF and the operated leg supportability; these patients, in addition to the operated joints, usually have pathologies of other parts of the musculoskeletal system (the adjacent joint, spine and small joints of the hand). Due to the general pathology, despite the performed TKE, the patients have pronounced disorders in SDF and the supportive function of the operated leg. They need additional help and an auxiliary means of transportation. Taking into account these limitations, they can work under the conditions of easy moving, and under specially created conditions. The listed above factors affect the complete recovery of patients after endoprosthetic surgery; ignoring these factors clearly reduces the TKE effectiveness. When studying the level of daily activity at home and social activities of the patients of the main group, a high percentage of a favourable outcome was noted after TKE. In this patient group, the quality of life of patients was higher than in the control group. In the main group of patients, the indicators of the rehabilitation success are much higher than in the control group. Moreover, it is true concerning not only the medical indicators, but also the social ones, that makes the susceptibility of the environment and routine activity more optimistic for these patients.
5. Conclusions
1. Early, comprehensive, individual and continuous rehabilitation of patients after TKE that takes into account the pathology of other parts of the musculoskeletal system improves the share of high rehabilitation efficiency, and reduces the number of patients with moderate efficiency compared with the control group.2. The developed system for assessing the disability of patients after TKE is based on: a) the disorder of the SDF and supportive ability of the operated leg; b) the pathology of adjacent joints and other parts of the musculoskeletal system increases the number of patients continuing their professional activities in the recommended jobs to 88% of cases.Conflict of interest – not declared.
References
| [1] | Sloan M, Premkumar A, Sheth NP. Projected Volume of Primary Total Joint Arthroplasty in the U.S., 2014 to 2030. J Bone Joint Surg Am. 2018; 100(17): 1455-60. doi: 10.2106/JBJS.17. 01617. |
| [2] | Gao J, Xing D, Dong Sh, et al. The primary total knee arthroplasty: a global analysis. Research Square. April 2020; doi:10.21203/rs.3.rs-22046/v1. License CC BY 4.0. |
| [3] | Zagorodny N.V., Kagramanov S.V., Kudinov O.A., et al.. Complex cases of knee arthroplasty. Bulletin of Traumatology and Orthopedics named after N.N. Priorov [.Zagorodny N.V., and co-authors. Bulletin of Traumatology and Orthopedic]. 2014; (1): 52–6. ttps://cyberleninka.ru/article/n/endoprotezirovanie- tazobedrennogo-i-kolennogo-sustavov-pokazaniya-k-operatsii?ysclid=m3kqwovb1u662850877. |
| [4] | Eshnazarov K. E., Hyoung-Sik Kim, Park Jin Oh, et al. Systematic review of the articles devoted to hip and knee arthroplasty and published in Korean, Russian and Ukrainian journals over the 2005–2014 years. Scientific and practical journal of Orthopedics, Traumatology and Prosthetics. Kharkov. 2015; (4): 134-139. doi: https://doi.org/10.15674/0030-598720154134-139. |
| [5] | Goryannaya N. А., Ishekova N. I., Popov V. V., Bondarenko Е. G. Change of Patients’ Quality of Life after Hip Replacement at the First Stage of Rehabilitation. Ekologiya cheloveka [Goryannaya N.A. and co-authors. Human Ecology]. 2017; 2: 41-44]. |
| [6] | Petrova R.V., Nikolaev N.S., Tsykunov M.B. Rehabilitation approaches in knee arthroplasty. Vestnik vosstanovitelnoy mediciny [Petrova R.V. and co-authors. Bulletin of Reconstructive Medicine] 2022; 21(2): 61-69. https://doi.org/10.38025/2078-1962-2022-21-2-61-69. |
| [7] | Demographic situation in the Republic of Uzbekistan. Agency of Statistics under the President of the Republic of Uzbekistan. [in Russian]. https://stat.uz/images/ demografiya-press-reliz-27_04_2023-rus-.pdf. |
| [8] | Madrakhimov S.B., Karimov M. Yu. Patients’ satisfaction after total knee arthroplasty: Tashkent Medical Academy experience. The Orthopaedic Journal of Sports Medicine, DKG International Knee Day conference, Berlin, 18-19 March – 2021. 9(6) (suppl 2): 52. |
| [9] | Choi Y-J, Ra HJ. Patient Satisfaction after Total Knee Arthroplasty. Knee Surg Relat Res. 2016 Mar 28(1): 1-15. doi: 10.5792/ksrr.2016.28.1.1. |
| [10] | George E. What is a Likert scale? Types, and examples. Researcher Life. 2024; https://researcher.life/blog/article/what-is-a-likert-scale-definition-types-and-examples/. |
| [11] | Charlson Comorbidity Index (CCI). https://clincasequest.org/charlson-comorbidity-index/. |
| [12] | Oswestry Disability Index (ODI) https://www.carepatron.com/files/oswestry-disability-index.pdf. |
| [13] | Ayers DC, Yousef M, Zheng H, et al. The Prevalence and Predictors of Patient Dissatisfaction 5-years Following Primary Total Knee Arthroplasty. J Arthroplasty. 2022 Jun; 37(6S): S121-S128. doi: 10.1016/j.arth.2022.02.077. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML