-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3812-3818
doi:10.5923/j.ajmms.20251511.12
Received: Oct. 5, 2025; Accepted: Oct. 23, 2025; Published: Nov. 6, 2025

Trends and Causes of Maternal Mortality in Andijan Region, Uzbekistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMalika Mamatova1, Rustam Ibragimov2, Rano Mamatova3
1Department of Obstetrics and Gynecology No. 1, Andijan State Medical University, Andijan, Uzbekistan
2Department of Surgical Diseases and Life Safety, Andijan State Medical University, Andijan, Uzbekistan
3Kokand University Andijan Branch, Therapeutic Faculty, Uzbekistan
Correspondence to: Malika Mamatova, Department of Obstetrics and Gynecology No. 1, Andijan State Medical University, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Maternal mortality remains a critical indicator of healthcare quality and a major public health concern in Uzbekistan. Understanding its epidemiological and clinical determinants is essential for developing targeted preventive strategies. Methods: A retrospective descriptive study was conducted to analyze all registered maternal deaths (n = 89) in the Andijan region, Uzbekistan, from 2017 to 2024. Data were obtained from official medical and statistical records. The maternal mortality ratio (MMR) per 100,000 live births was calculated. Deaths were classified by direct and indirect causes, maternal age, parity, place of residence, and type of healthcare facility. Results: The MMR ranged from 11.3 to 14.9 per 100,000 live births, with a mean of 13.7. Direct obstetric causes accounted for 69.7% of deaths, primarily preeclampsia and obstetric hemorrhage (24% each). Indirect causes, including pneumonia and COVID-19 complications, represented 13%. Mortality was higher in rural than in urban areas (MMR 14.6 vs. 12.0). Women under 19 and over 35 years had significantly greater risk (RR 5.55 and 22.71, respectively) compared to the 20–29-year age group. Primiparous women comprised 40.4% of cases. Conclusion: Maternal mortality in the Andijan region remains a pressing public health issue, dominated by preventable direct causes. Targeted interventions should focus on rural populations, adolescents, older mothers, and primiparous women. Improving emergency obstetric care, surveillance, and access to skilled delivery services is essential for further reducing maternal mortality.
Keywords: Maternal Mortality, Pregnancy Complications, Preeclampsia, Postpartum Hemorrhage, Risk Factors, Uzbekistan
Cite this paper: Malika Mamatova, Rustam Ibragimov, Rano Mamatova, Trends and Causes of Maternal Mortality in Andijan Region, Uzbekistan, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3812-3818. doi: 10.5923/j.ajmms.20251511.12.
Article Outline
1. Introduction
- Maternal mortality (MM) is a key indicator of the state of the healthcare system and the social well-being of the population. According to the World Health Organization (WHO), approximately 810 women worldwide die daily from complications related to pregnancy or childbirth, with 60% of these MM cases being preventable [1]. The maternal mortality ratio (MMR), defined as the number of maternal deaths per 100,000 live births, is among the principal indicators for achieving the Millennium Development Goals (MDGs) and the United Nations Sustainable Development Goals (SDGs) [2,4]. A high level of MM constitutes a serious challenge that necessitates analysis and the development of strategies to improve the quality of medical care and social support for women during pregnancy.In the Republic of Uzbekistan, comprehensive changes have been implemented in the healthcare sector since gaining independence, including extensive reforms across all medical fields, which have significantly contributed to improving the quality of healthcare services for the population. The protection of maternal and child health remains a priority policy area in the country. As a result of these reforms, over the past 25 years, the MMR in Uzbekistan has decreased more than threefold: from 65.5 per 100,000 live births in 1990 to 18.9 in 2015. Despite this progress, the rate of decline in MM slowed during the period 2000–2017, amounting to 36% [3]. At the 2015 United Nations Summit, a set of SDGs was adopted, including the goal of reducing MM by one-third by 2030 compared to 2015 levels. As a UN member, Uzbekistan endorsed these goals and adopted several key documents to support their implementation: the “National Goals and Objectives for Achieving the United Nations Sustainable Development Goals until 2030” in 2017; Resolution No. 841 “On Measures for the Implementation of National Goals and Objectives in the Field of Sustainable Development until 2030” in 2018; and Resolution No. 83 “On Additional Measures to Accelerate the Implementation of National Goals and Objectives in the Field of Sustainable Development until 2030” in 2022 [4-7].Despite healthcare reforms and policy initiatives, there are few comprehensive regional analyses of ММ in Uzbekistan. The Andijan region, with its large population and predominantly rural demographics, represents an important case for assessing maternal health outcomes and identifying persisting risk factors.Study aim and research question.This study aimed to conduct a retrospective analysis of ММ in the Andijan region of Uzbekistan between 2017 and 2024, focusing on trends in the MMR, underlying causes of death, and associated demographic and obstetric risk factors. The primary research question was: what are the leading causes and determinants of MM in the region during this period?Study type.Given its retrospective and descriptive design, the study is exploratory in nature. It was intended to generate evidence on risk patterns and to inform targeted preventive strategies, rather than to test a predefined hypothesis.
2. Materials and Methods
- This study is a retrospective descriptive analysis based on statistical records and medical documentation provided by local health authorities. All data were anonymized to maintain confidentiality.The total number of live births in the Andijan region during the study period (2017–2024) was collected and used as the denominator to calculate the maternal mortality ratio (MMR), ensuring the accuracy and reliability of the findings.Research methods included: descriptive statistics and epidemiological analysis to assess trends in MMR, correlation analysis to examine associations between MM and various risk factors, data processing using Microsoft Excel. Microsoft Excel was utilized for data processing and statistical analysis due to its accessibility and capability for handling epidemiological datasets. However, to enhance the robustness of the results, additional statistical tests to assess the significance of observed trends and associations were conducted using appropriate software tools.Limitations of this study include potential inaccuracies or incompleteness in medical records, which may affect the comprehensiveness of the data. Ethical Considerations. This study is a retrospective analysis based on anonymised registry data provided by the Andijan Regional Health Authorities. No direct contact with participants occurred, and no identifying information was collected. In accordance with national regulations in Uzbekistan, retrospective analyses of anonymised secondary data do not require formal approval by a research ethics committee or individual informed consent.
3. Results
- During the study period, 89 maternal deaths were registered in the region. The MMR oscillated between 11.3 and 14.9 per 100,000 live births. The lowest value was recorded in 2017 (12.6), the highest in 2019 (14.9). The average ratio over the analyzed years was 13.73 ± 1.15. Despite observed fluctuations, no definitive upward or downward trend was identified; instead, the data reflect seasonal or random variations. The notable decline in 2024 may indicate positive developments in maternal healthcare or the effectiveness of preventive interventions (figure 1).
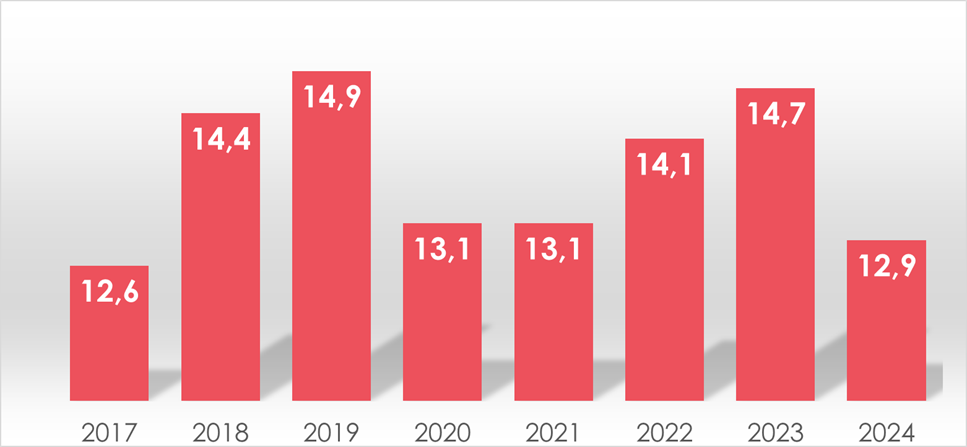 | Figure 1. Trends in the maternal mortality ratio (MMR) per 100,000 live births in the Andijan region, Uzbekistan, 2017–2024. Data were obtained from the official records of the Andijan Regional Health Authorities. MMR = maternal mortality ratio (number of maternal deaths per 100,000 live births) |
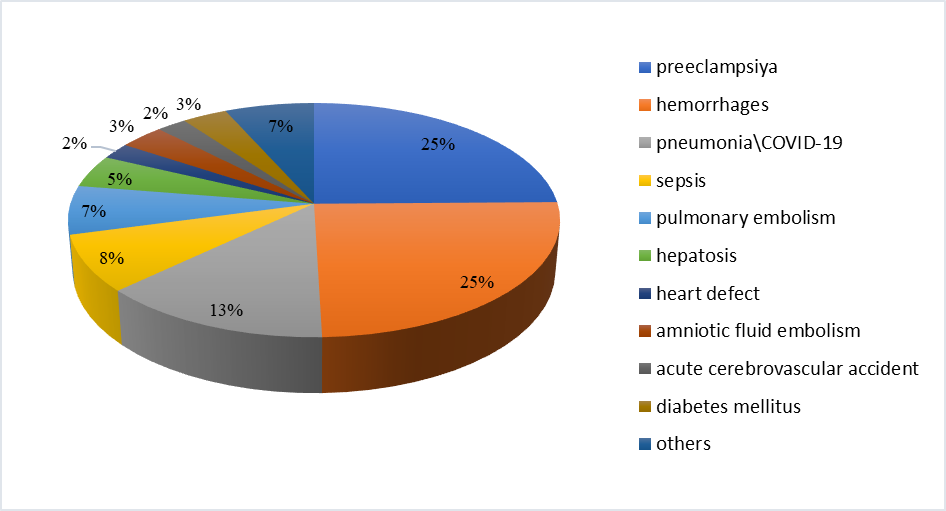 | Figure 2. Distribution of maternal deaths by direct obstetric causes, Andijan region, 2017–2024. Causes include postpartum haemorrhage, hypertensive disorders, sepsis, and other obstetric complications |
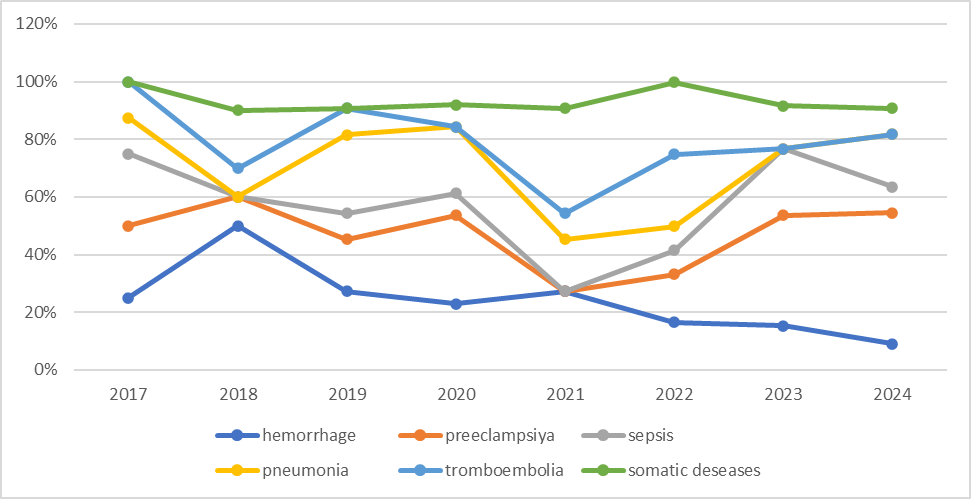 | Figure 3. Dynamics of maternal mortality causes in the Andijan region, 2017–2024. Trends are shown for major direct and indirect causes of maternal death, including haemorrhage, preeclampsia, sepsis, pneumonia, thromboembolism, and somatic diseases. Source: Andijan Regional Health Authorities |
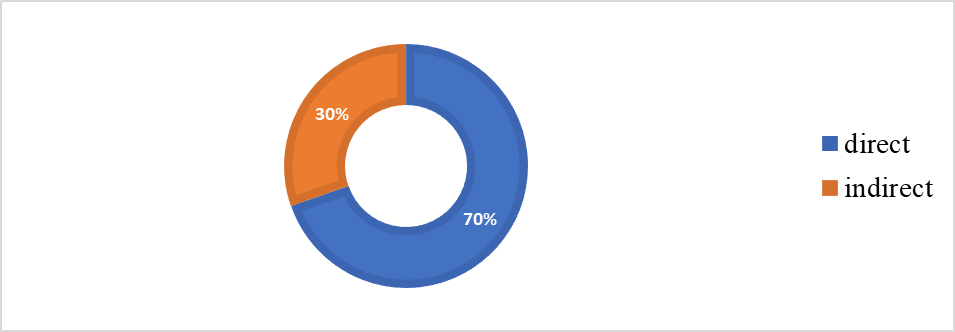 | Figure 4. Structure of direct and indirect causes of maternal mortality in the Andijan region, 2017–2024. Source: Andijan Regional Health Authorities |
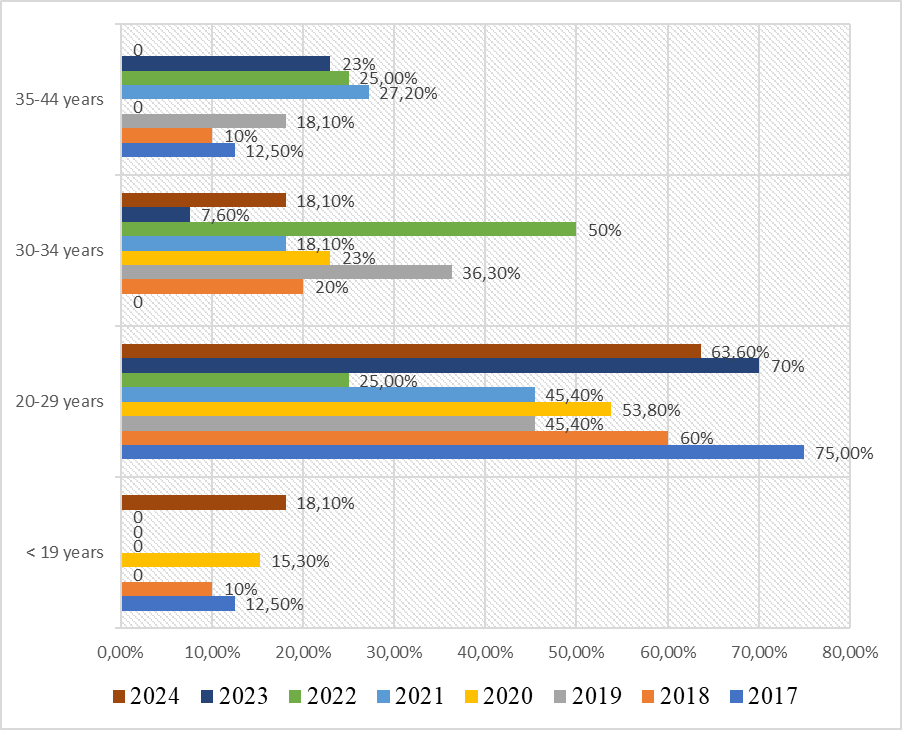 | Figure 5. Maternal mortality by age group in the Andijan region, 2017–2024. Data presented as percentages of total maternal deaths |
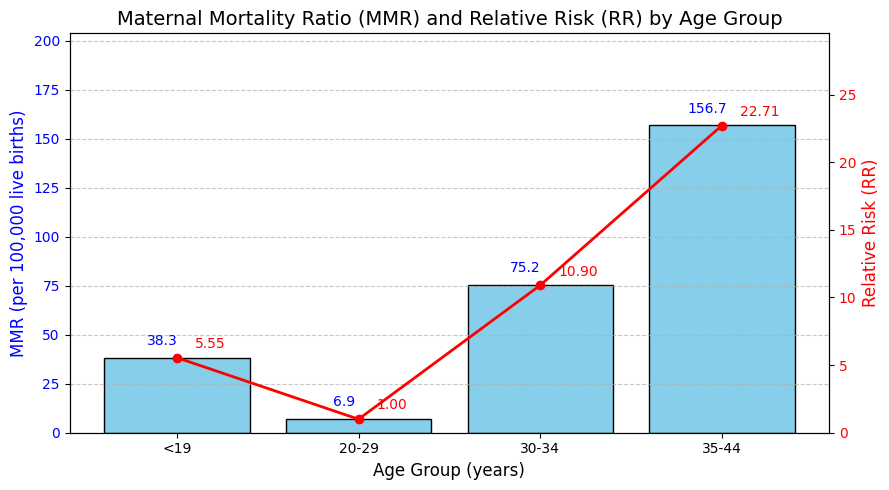 | Figure 6. MM ratio and relative risk (RR) by age groups. Data normalized per 100 000 live births; RR calculated relative to 25–29 age group |
|
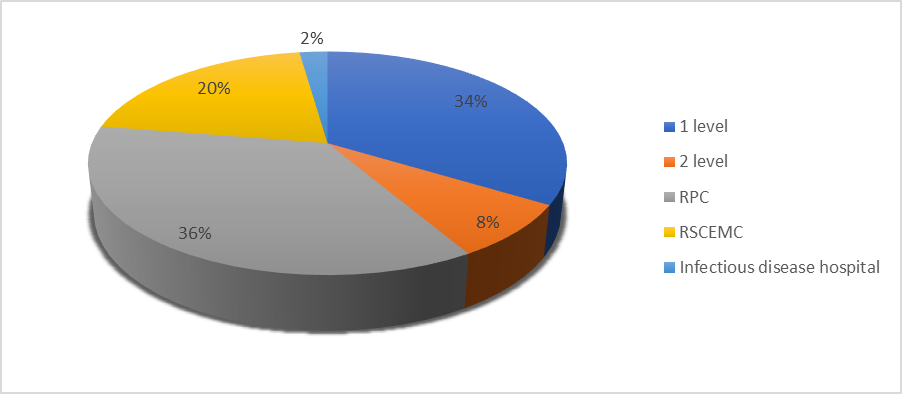 | Figure 7. Location of maternal mortality cases in the Andijan region, 2017–2024. Distribution of maternal deaths by type of medical organization, expressed as percentages of total cases. Statistically significant differences were observed across groups (χ² test, p < 0.05). Source: Andijan Regional Health Authorities |
4. Discussion
- Summary of main findingsThis study provides the first comprehensive retrospective analysis of MM in the Andijan region from 2017 to 2024. The MMR remained relatively stable during this period, fluctuating between 11.3 and 14.9 per 100,000 live births, with no clear downward trend. Direct obstetric causes, particularly preeclampsia and obstetric hemorrhage, predominated, while infectious diseases, including pneumonia and COVID-19 complications, also contributed substantially to maternal deaths. Mortality was significantly higher among rural residents, adolescents, women over 35 years, and primiparous mothers.Preventive strategies should prioritize:1. Early identification and management of hypertensive disorders.2. Strengthening blood transfusion and hemorrhage control systems.3. Expanding continuous professional training for obstetric staff.4. Implementing digital surveillance and telemedicine tools to monitor high-risk pregnancies.Interpretation and comparison with other studiesThe predominance of preventable obstetric causes aligns with findings from other middle-income countries, where hemorrhage and hypertensive disorders remain leading contributors to maternal deaths. These causes are largely avoidable with timely diagnosis, effective referral, and adequate emergency obstetric care. The emergence of infectious causes, particularly during the COVID-19 pandemic, underscores the vulnerability of maternal health services to emerging public health threats. Our results on elevated risk among younger (<19 years) and older (>35 years) mothers are consistent with international evidence demonstrating age-related vulnerability. Similarly, the high proportion of deaths among primiparous women highlights the need for intensified monitoring during first pregnancies.Public health implicationsThe higher MMR observed in rural areas reflects persistent inequalities in access to quality healthcare. Strengthening healthcare infrastructure, improving referral systems, and training obstetric personnel in rural districts should be prioritized. Preventive interventions targeting preeclampsia and obstetric hemorrhage, as well as integrated surveillance for infectious diseases, are essential for further reducing MM. Tailored community-based programs addressing adolescents, older mothers, and primiparous women are also warranted.Strengths and limitationsAs noted earlier, this study analysed all maternal deaths in the Andijan region over an eight-year period, ensuring complete population coverage and reliable epidemiological data. However, the retrospective design and reliance on medical records limited control over data quality, and missing clinical details restricted analysis of confounding factors.Future researchFurther prospective studies incorporating individual-level clinical data are needed to explore the underlying determinants of MM. Research should also assess the effectiveness of targeted interventions in reducing preventable obstetric deaths and in addressing inequalities between rural and urban populations.
5. Conclusions
- MM in the Andijan region remains a persistent public health challenge. Preventable direct obstetric causes, particularly preeclampsia and obstetric haemorrhage, accounted for the majority of deaths, with higher risks observed among rural residents, adolescents, women over 35 years, and primiparous mothers.Targeted interventions focusing on early detection and management of hypertensive disorders and haemorrhage, strengthening healthcare capacity in rural districts, and integrating infectious disease surveillance into maternal health services are essential. Tailored community-based programmes for high-risk groups should be prioritised to achieve further reductions in maternal mortality and to guide regional health policy.
ACKNOWLEDGEMENTS
- The author thanks the Andijan Regional Health Authorities for providing access to anonymized statistical data, and colleagues from the Department of Obstetrics and Gynecology, Andijan State Medical University, for their valuable comments during the preparation of this work.