Qurbonov D. D., Azizov M. K., Axmedov Yu. M., Axmedov I. Yu.
Samarkand Regional Children's Multidisciplinary Medical Center, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Qurbonov D. D., Samarkand Regional Children's Multidisciplinary Medical Center, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
This article research confirms that the widespread adoption of laparoscopic technologies in pediatric surgery is safe and effective. In the context of a changing economic situation, the issue of a complete transition of medical institutions to minimally invasive methods for treating surgical diseases in children is becoming particularly relevant. Traditional surgical approaches, used in pediatric practice for decades, are associated with several significant drawbacks, such as pronounced postoperative pain syndrome, prolonged hospitalization, a high risk of postoperative scar formation, and related cosmetic defects, which are especially significant in childhood.
Keywords:
Childhood, Domestic clinical practice, Pediatric surgery, Appendicitis, Systematic studies
Cite this paper: Qurbonov D. D., Azizov M. K., Axmedov Yu. M., Axmedov I. Yu., Assessment of Laparoscopic Treatment Methods in Pediatric Purulent-Inflammatory Abdominal Conditions, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3796-3802. doi: 10.5923/j.ajmms.20251511.09.
1. Introduction
The implementation of endoscopic minimally invasive technologies in emergency surgical care for children, actively studied abroad, remains insufficiently investigated in domestic clinical practice. Despite individual publications, systematic studies analyzing the role of such techniques in emergency conditions in pediatric surgery are rare. For example, endoscopic appendectomy has become firmly established in clinical protocols [44, 110, 247]; however, its appropriateness in complicated forms of appendicitis (perforation, peritonitis) continues to be a subject of debate among specialists [262]. The main points of discussion concern the adequacy of abdominal cavity lavage/debridement with the laparoscopic approach, the specific technical aspects of performing surgical stages in the presence of an inflammatory process, and the possibilities for monitoring the effectiveness of intraoperative manipulations. Opinions are divided regarding the advantages of minimally invasive techniques in cases of complex anatomical variations of the inflammatory focus location.The economic component of this issue is also of fundamental importance, considering the anticipated reduction in the hospitalization period, a decrease in the frequency of postoperative complications, and a reduced need for analgesic therapy when using minimally invasive techniques. At the same time, it is necessary to objectively assess the initial costs for the acquisition and maintenance of specialized endoscopic equipment, as well as the training of surgical teams in new technologies.Currently, there is no systematic analysis of algorithms for clinics transitioning to laparoscopic methods in pediatric emergency abdominal surgery. This underscores the need for further research and the development of universal solutions. The development of clear criteria for selecting the surgical approach for various nosological forms of purulent-inflammatory diseases of the abdominal cavity in children, considering the stage of the inflammatory process, patient's age, concomitant pathologies, and the technical capabilities of the medical institution, appears particularly relevant. Stratification of patients by risk groups for conversion to open surgery would allow for optimizing the planning of surgical interventions and minimizing intraoperative complications.Aim of the study: To improve the treatment outcomes for patients with purulent-inflammatory diseases of the abdominal cavity using minimally invasive surgeries, by substantiating the effectiveness of their use in pediatric surgery.
2. Materials and Methods
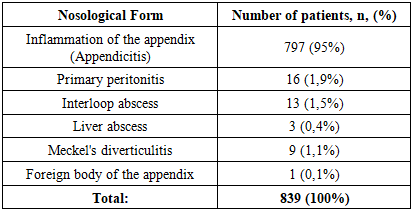
The study analyzed the results of surgical treatment of children with purulent-inflammatory diseases of the abdominal cavity: a total of 839 patients. Among them, 797 (52.6%) children had acute appendicitis and appendicular peritonitis; 16 patients had primary peritonitis; 16 patients had an abdominal and liver abscess; 9 patients had Meckel's diverticulitis; and in one case, a foreign body in the appendix was observed, which caused secondary appendicitis.Data on the distribution of patients within the group are presented in Table 1.Table 1. Structure of the patient group with purulent-inflammatory diseases of the abdominal cavity
 |
| |
|
All patients in the study underwent a complex of various research methods, including clinical, laboratory, and instrumental approaches. Among the instrumental techniques used were ultrasound diagnostics of the abdominal cavity and pelvic organs, and radiological studies (plain radiography, contrast-enhanced X-ray study). Furthermore, laparoscopy was included in the diagnostic process.
3. Results of the Study
An analysis of the effectiveness of laparoscopic technologies in a group of 839 patients with purulent-inflammatory diseases of the abdominal cavity demonstrated a dependence of the results on the quantitative and qualitative composition of the syndromic group, as reflected in Figure 1 and Table 2.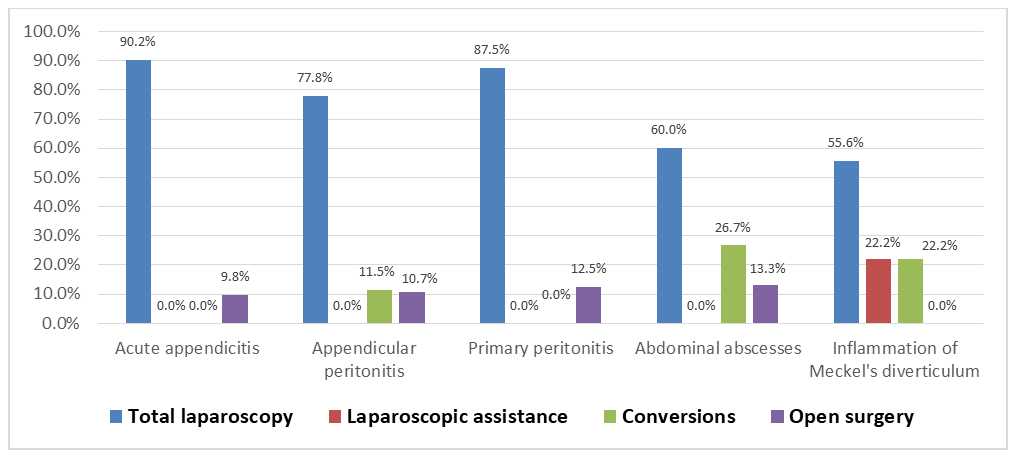 | Figure 1. Types of surgical interventions in the group of patients with purulent-inflammatory diseases of the abdominal cavity |
 | Table 2. Types and scope of surgical interventions in the group of patients with purulent-inflammatory diseases of the abdominal cavity |
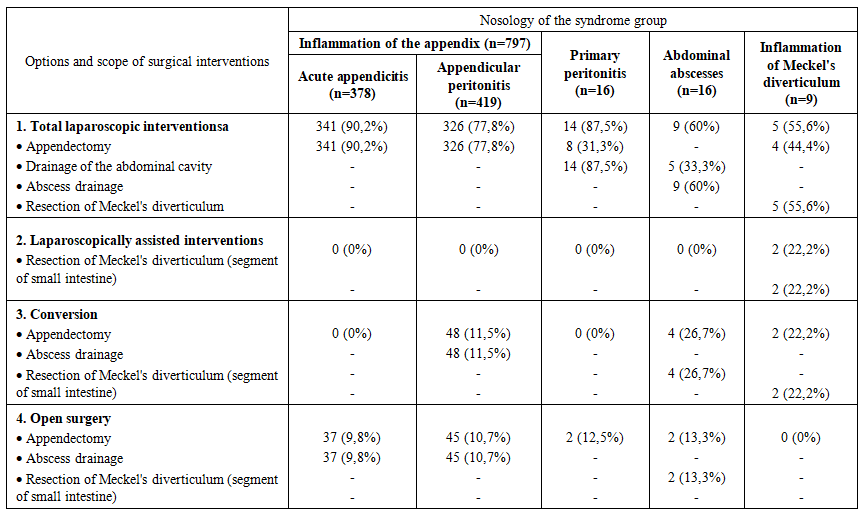
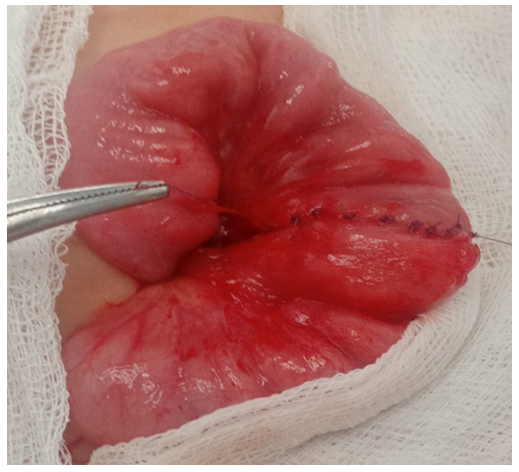
Total laparoscopic interventions demonstrated a statistically significant advantage in children with specific pathologies: for acute appendicitis, this method was applied in 90.2% of cases; for appendicular peritonitis – in 77.8%; and for primary peritonitis – in 87.5% of observations. It is important to note that the success rate of total laparoscopic interventions correlated with the experience of the surgical team and the stage of implementation of the technique into clinical practice. Thus, an analysis of the dynamics of indicators over the entire study period showed a statistically significant increase in the proportion of successfully completed laparoscopic operations and a decrease in the frequency of conversions with the accumulation of experience in using the technique.The feasibility of performing total laparoscopy was determined by several key factors: clarity of visualization and localization of the inflammatory focus during laparoscopic examination, the absence of combined gastrointestinal tract lesions, and the standardization of individual stages of the surgical intervention. It should be emphasized that intraoperative assessment of the extent of the inflammatory process during laparoscopy allowed for a more precise determination of the nature of the pathological effusion, the degree of involvement of adjacent anatomical structures, and the presence of concomitant pathological changes, which in turn determined the surgical treatment tactics in each specific case.Laparoscopically-assisted interventions were used in children with Meckel's diverticulitis in 2 observations (22.2%), predominantly in cases of localization of the inflammatory process or damage in the middle sections of the intestine. This type of surgical intervention represented a rational compromise between the advantages of minimally invasive access at the diagnostic stage and the necessity of performing technically complex manipulations under direct visual control. The laparoscopically-assisted method allowed for minimizing surgical trauma and simultaneously ensuring the reliability of intestinal anastomosis formation if resection of the intestinal segment with the altered diverticulum was necessary.Conversion was performed in cases of intraoperative detection of a complicated course of certain nosological forms within this syndromic group. The highest frequency of conversions was noted in 4 patients (26.7%) with abdominal abscesses, which was due to technical difficulties in the laparoscopic dissection of dense fibrinous adhesions and the risk of damage to the walls of hollow organs during manipulations in conditions of pronounced perivisceritis. In the groups with appendicular peritonitis and Meckel's diverticulitis, conversion was required in 48 (11.5%) and 2 (22.2%) cases, respectively. Analysis of the reasons for conversion allowed for the identification of several prognostically unfavorable factors, such as duration of the disease for more than 72 hours before hospitalization, the presence of a clinical picture of intestinal obstruction, recurrent episodes of purulent-inflammatory abdominal diseases in the medical history, and certain anatomical variations in the location of the inflammatory focus (retrocecal and retroperitoneal position of the appendix). These data can be used in the development of prognostic scales to determine the risk of conversion and the optimal choice of the primary surgical approach.Open surgeries were performed in the early stages of the study, when there was insufficient experience in performing laparoscopic operations. Thus, in children with acute appendicitis, open operations were performed in 37 (9.8%) patients; with appendicular peritonitis – in 45 (10.7%); with primary peritonitis – in 2 (12.5%); and in 2 patients with abdominal abscesses, which constituted 13.3%. A clear trend towards a decrease in the proportion of open operations was noted with the accumulation of experience and the improvement of the technical equipment of the surgical service.In the group of 378 patients with acute appendicitis, laparoscopic interventions demonstrated effectiveness in 341 (90.2%) observations. When extracting large appendices, a specimen retrieval bag (endobag) was used to prevent infection of the abdominal cavity. The use of a specimen retrieval bag allowed for minimizing the risk of contamination of the wound surface and abdominal cavity with pathological contents during the extraction of gross specimens through miniature laparoscopic ports. Abdominal cavity lavage and drainage were not performed, as pathological effusion was not detected in any case. This circumstance confirms the advantages of the laparoscopic approach in terms of visual assessment of the abdominal cavity condition and rational determination of the scope of surgery without unnecessary manipulations.In the group of 242 patients with stage I appendicular peritonitis, total laparoscopic interventions were effective in 90.9% of cases; in the remaining cases, conversion was required in 3.7% of cases, and open surgeries were performed in 5.4% of cases. When extracting large appendices, a specimen retrieval bag was also used. Abdominal cavity sanitation by aspiration of pathological effusion was performed in 184 patients (76%). It is important to note that the laparoscopic approach allowed for selective aspiration of effusion from anatomical areas most prone to the accumulation of pathological exudate (right paracolic gutter, pelvic cavity) without additional traumatization of intact areas of the abdominal cavity.In the group of 141 patients with stage II appendicular peritonitis, laparoscopic interventions were performed in 106 cases (75.2%). When extracting large appendices and resected omental fragments, a specimen retrieval bag was used twice as often, due to the pronounced destruction of the appendices and their partial rupture during mobilization. This tactic helped prevent the dissemination of infection and the formation of secondary abscesses in the postoperative period. In cases of extensive peritonitis, abdominal cavity sanitation was carried out by aspiration of pathological effusion and lavage in 96 patients (68.1%). A characteristic feature of laparoscopic sanitation was the significantly smaller volume of solutions used (1-2 liters) due to targeted lavage of anatomical areas under visual control. Unlike open surgeries, where the volume of irrigation solutions could reach 4-6 liters, the laparoscopic sanitation technique made it possible to avoid excessive exposure to serous membranes and reduce the risk of developing adhesive disease in the long-term period. All surgical interventions were completed with active drainage of the abdominal cavity with placement of drainage systems in the right lateral canal and the pelvic cavity.Conversions were performed in 14 children (9.9%) who had an anterosuperiorly located appendiceal inflammatory mass with marked destruction, where the source of inflammation was difficult to access due to complete adhesions. In such cases, the decision to convert was made based on an objective assessment of the technical difficulties of laparoscopic mobilization of the appendix and the risk of damage to adjacent structures, which indicates a balanced approach to determining the limits of applicability of laparoscopic technologies. In the first years of observation, 14.9% of patients underwent open operations, reflecting the natural learning curve of the surgical team with new minimally invasive techniques.In the group of 36 patients with stage III appendicular peritonitis, laparoscopic technologies were successfully applied in 10 observations (27.8%). Despite the relatively low success rate of total laparoscopic interventions in this subgroup, the very fact that the operation could be performed via a laparoscopic approach even in such a severe condition as diffuse peritonitis is indicative. During laparoscopic interventions, adhesiolysis of loose intestinal adhesions was performed, which allowed for the resolution of preoperative mechanical intestinal obstruction in two patients. This aspect demonstrates the expanded capabilities of laparoscopy not only in diagnosis but also in the treatment of concomitant complications of purulent-inflammatory abdominal diseases. Abdominal cavity sanitation was achieved by thorough aspiration of pathological effusion from the right lateral canal and the pelvic cavity. Surgical interventions were completed with drainage of the abdominal cavity using single-lumen prophylactic drains. Conversion was required in 25 patients (68.4%); of these, appendectomy was successful in 22 (61.1%), while in the remaining 3 patients (8.3%), the operation was limited to drainage of the abdominal cavity due to a suppurative appendiceal mass. Open surgery was performed in 1 (2.8%) patient. The high frequency of conversions in this subgroup was explained by significant technical difficulties in performing laparoscopic manipulations in conditions of diffuse peritonitis with fibrinous deposits and pronounced intestinal paresis.In the group of patients with stage I primary peritonitis (n=6), a positive clinical outcome was achieved in all cases (100%) after laparoscopic surgery. The standard protocol included appendectomy followed by abdominal cavity sanitation through aspiration of pathological exudate with an electric suction device. It is important to note that in cases of primary peritonitis, the laparoscopic approach had a particular advantage, allowing visual confirmation of the absence of organic causes of peritonitis and ruling out other diseases with a similar clinical picture. Total laparoscopy was successful in 7 patients (87.5%) with stage II disease. In 5 of these patients (71.4%), secondary changes in the appendix were identified, requiring its removal. These data demonstrate the difficulty of differential diagnosis between primary and secondary peritonitis at the preoperative stage and underscore the diagnostic value of laparoscopy. A feature of sanitation was the use of targeted irrigation under visual control with a limited volume of irrigation solutions (1-2 L). In all cases, the procedure was completed by placing active drainage systems, which allowed for the effective removal of residual exudate in the postoperative period. The frequency of open operations in the group of patients with stage II disease was 12.5% (1/8).In stage III disease (n=2), technical success of laparoscopic intervention was recorded in 50% of observations (1 patient). In this patient, an appendectomy was performed with thorough aspiration of purulent content from the right lateral canal and pelvic cavity. Open surgery was performed in 1 patient (50%). The limited number of observations in this subgroup makes it difficult to formulate statistically significant conclusions but demonstrates the potential applicability of laparoscopic techniques even in severe forms of primary peritonitis.In the group of patients with interloop abscess (n=13), laparoscopic interventions demonstrated effectiveness in 7 (53.8%) patients. This indicator reflects the objective technical difficulties of laparoscopic access to interloop abscesses, due to their anatomical location and the presence of pronounced adhesive changes around the abscess. In 4 (30.8%) cases, sanitation and drainage of the abscess were carried out after conversion of access. In 2 patients (15.4%), open surgery was performed. Analysis of the postoperative period showed comparable treatment outcomes with different surgical access options, which indicates the priority of the principle of adequate sanitation of the purulent focus over the technical specifics of its performance.Among patients with liver abscess (n=3), laparoscopic interventions were successfully performed in 2 (66.7%) observations. In 1 (33.3%) patient, conversion was required due to difficult visualization of the inflammation source amidst a pronounced adhesive process. All surgical interventions were completed with drainage of the abscess cavity and the abdominal cavity using single-lumen prophylactic drains. Although the number of patients in this subgroup was small, the results obtained indicate the principal feasibility of laparoscopic access to liver abscesses and their effective drainage under endovideosurgery conditions.Here is a clinical case presentation:A 3-year-old patient was hospitalized with a 16-hour history of abdominal pain, with a primary diagnosis of acute appendicitis. Upon admission, the patient's condition was assessed as moderately severe, with a body temperature of 38.3°C, and reported weakness, malaise, and abdominal pain, predominantly localized in the periumbilical region. Palpation of the abdomen revealed tenderness, most pronounced in the right iliac fossa, significant passive muscular guarding, and peritoneal signs were questionable. The liver and spleen showed no pathological changes. Stool was spontaneous, without pathological impurities. Urination was free and painless.An ultrasound examination of the abdominal cavity revealed a volumetric, aperistaltic mass in the right iliac fossa, with a diameter of up to 30 mm, containing a tubular structure and surrounded by anechoic omental tissues – presumably a periappendiceal abscess.After preoperative preparation, indications for surgical intervention (laparoscopy) were determined. The preoperative diagnosis was: acute appendicitis, localized peritonitis.The operation performed was: laparoscopy, laparoscopically-assisted resection of a segment of the ileum with Meckel's diverticulum, anastomosis formation. Abdominal palpation was performed under anesthesia. In the mesogastric region, predominantly on the right, a moderately mobile mass with a diameter of up to 5 cm was identified, having a firm-elastic consistency and clear boundaries. A pneumoperitoneum was established, and 5-mm instruments were inserted.Upon revision of the abdominal cavity, a small amount of purulent exudate was found in the lesser pelvis, and material was collected for bacteriological examination. The vermiform appendix was intact and located in its typical position. During the revision of the ileum, a Meckel's diverticulum with a wide base, covered by inflammatory fibrinous adhesions, was visualized at a distance of 60 cm from the ileocecal angle. Laparoscopic lysis of fibrinous adhesions was performed. The Meckel's diverticulum was spherical, up to 3 cm in length, with a wide base (up to 2 cm), and markedly infiltrated (Figure 2).Given the necessity of resecting the Meckel's diverticulum, the periumbilical access was extended. The segment of the ileum with the Meckel's diverticulum was extraperitonealized (Figure 3), and a resection of the ileal segment with the Meckel's diverticulum and entero-enteroanastomosis were performed (Figure 4). | Figure 2. Laparoscopy. Meckel's diverticulum |
 | Figure 3. Meckel's diverticulum with a segment of the ileum (extraperitonized) |
 | Figure 4. Entero-enteroanastomosis (after resection of part of the small intestine together with the diverticulum) |
 | Figure 5. Macroscopic specimen. Resected part of the intestine with Meckel's diverticulum |
The postoperative diagnosis was: Meckel's diverticulitis.The postoperative period was uneventful, with parenteral nutrition administered for up to 4 days. The patient was discharged home on the 8th day with full recovery.The presented clinical observation demonstrates the possibility of successfully completing an operative intervention using an endosurgical approach by performing a laparoscopically-assisted resection of an ileal segment with destructive Meckel's diverticulitis, the macroscopic changes of which limited the possibility of performing laparoscopic diverticulectomy.In patients (n=5) with stage II Meckel's diverticulitis, laparoscopic techniques proved effective in all cases, confirming the high potential of minimally invasive technologies in treating this pathology. The methods of Meckel's diverticulum resection were determined by its anatomical location, the degree of inflammatory changes, and structural features. Total laparoscopic diverticulectomy was performed in 3 patients (66.7%) with the phlegmonous form of Meckel's diverticulitis. Technically, this operation included mobilization of the diverticulum, transection of its base using a linear endoscopic stapler, and extraction of the resected diverticulum in an endocontainer. Laparoscopically-assisted resections of Meckel's diverticulum were applied in 2 children (33.3%), primarily in cases of significant destruction at the base of the diverticulum. After extraperitonealization of the ileal segment, Meckel's diverticulum resections were performed using a "closed method" (n=1) and resection of the ileal segment with entero-enteroanastomosis formation (n=1). The choice of method was determined by the nature and extent of inflammatory changes, allowing for individualized surgical tactics in each specific case.
4. Conclusions
Analysis of the results of surgical treatment of 839 children with purulent-inflammatory diseases of the abdominal organs demonstrated significant advantages and high effectiveness of total laparoscopic interventions. Specifically, their success rate was 90.2% for acute appendicitis, 77.8% for appendicular peritonitis, and 100% and 87.5% for primary peritonitis stages I and II, respectively. Efficacy was also high in the treatment of stage II Meckel's diverticulitis (100%) and liver abscesses (66.7%).The key determinants of success for laparoscopic access were clear intraoperative visualization, precise localization of the inflammatory focus, the absence of concomitant gastrointestinal lesions, and standardization of operative stages. Laparoscopy allowed for targeted debridement of the abdominal cavity, for example, in stage II appendicular peritonitis, using significantly smaller volumes of irrigation solutions (1-2 liters) under visual control, and effective drainage of pathological foci.Despite high overall effectiveness, in some cases, especially with complicated forms of purulent-inflammatory diseases of the abdominal organs (e.g., stage III appendicular peritonitis, where laparoscopy was successful in 27.8%, or interintestinal abscesses – 53.8%), and also during the initial stages of mastering the techniques, conversion of access was necessary (e.g., 26.7% for abdominal abscesses) or initially open operations were performed. The main reasons for conversion were pronounced adhesive processes, technical difficulties with destructive changes, and intraoperative detection of a complicated course.Thus, the study confirms the advisability of widespread implementation of laparoscopic technologies to improve treatment outcomes in children with purulent-inflammatory diseases of the abdominal organs. The justified application of minimally invasive surgeries, considering the stage of the process and accumulated experience, is a promising direction in pediatric abdominal surgery, requiring further development of algorithms and improvement of techniques.
References
| [1] | Akilov Kh.A., Urmanov N.T., Primov F.Sh., Juraev Zh.A., Khadjayarov N.R. Experience in treating acute appendicitis in Tashkent // Pediatric Surgery. – 2019. Vol. 23, No. 3. pp. 157–160. |
| [2] | Vrublevsky S.G., Poddubny I.V., Trunov V.O. et al. Emergency abdominal pathology in infants // Pediatric Surgery. – 2015. No. 3. pp. 32–33. |
| [3] | Gallyamov E.A., Biktimirov R.G., Agapov M.A. Technical development of laparoscopic pelvic surgery // Almanac of Clinical Medicine. – 2018. Vol. 46, No. 6, pp. 631–639. |
| [4] | Dronov A.F., Kotlobovsky V.I., Poddubny I.V. Laparoscopic operations in children: real ways to improve treatment outcomes // Endoscopic Surgery in Children: Symposium Proceedings. – Ufa, 2002. pp. 41–45. |
| [5] | D'yakonova E.V. Laparoscopic surgery in emergency pediatric abdominal surgery: Abstract of Doctoral Dissertation. – 2018. 78 p. |
| [6] | Clinical Guidelines of the Ministry of Health of the Russian Federation. Acute Appendicitis. – 2016. 88 p. |
| [7] | Poddubny I.V., D'yakonova E.Yu., Ismailov M.U. et al. Laparoscopic surgery for Meckel’s diverticulum pathology // Pediatric Surgery. – 2015. No. 5. pp. 4–6. |
| [8] | Sokolov Yu.Yu., Korovin S.A. Classification variant of acute appendicitis and peritonitis in children // Russian Bulletin of Pediatric Surgery, Anesthesiology and Intensive Care. – 2013. Vol. 3, No. 1. pp. 28–31. |
| [9] | Biondi A., Di Stefano C., Ferrara F., Bellia A., Vacante M., Piazza L. Laparoscopic versus open appendectomy: a retrospective cohort study assessing outcomes and cost-effectiveness // World Journal of Emergency Surgery. – 2016 Aug 30; 11(1): 44. doi: 10.1186/s13017-016-0102-5. |
| [10] | Brian Ezekian, Harold J. Leraas, Brian R. Englum, Brian F. Gilmore, Christopher Reed, Tamara N. Fitzgerald, Henry E. Rice, Elisabeth T. Tracy. Outcomes of laparoscopic resection of Meckel's diverticulum are equivalent to open laparotomy // Journal of Pediatric Surgery. – 2018. https://doi.org/10.1016/j.jpedsurg.2018.03.010. |
| [11] | Hope T. Jackson, Sohail R. Shah, Emily Hathaway, Evan P. Nadler, Richard L. Amdur, Shannon McGue. Evaluating the impact of a minimally invasive pediatric surgeon on hospital practice: comparison of two children’s hospitals // Surgical Endoscopy. – 2016. 30: 2281–2287. |
| [12] | O. Muensterer, M. Bronstein. Factors associated with passing the European Board of Pediatric Surgery exam // Pediatric Surgery International. – 2015. pp. 18–24. |
| [13] | Rebecca M. Rentea, Shawn D. St. Peter, Charles L. Snyder. Pediatric appendicitis: state-of-the-art review // Pediatric Surgery International. – 2017. No. 33. pp. 269–283. doi: 10.1007/s00383-016-399. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML