-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3784-3788
doi:10.5923/j.ajmms.20251511.07
Received: Oct. 15, 2025; Accepted: Oct. 29, 2025; Published: Nov. 3, 2025

Pharmacological Treatment of Sensorineural Hearing Loss in Industrial Workers: Clinical Effectiveness and Symptom Monitoring
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUlugbek Khasanov, Abidova Dildora
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the clinical outcomes of pharmacological treatment for sensorineural hearing loss among industrial workers exposed to noise and vibration. A total of 63 patients received a 4-week course of medications aimed at improving cochlear blood flow, restoring auditory nerve function, and regulating vestibular balance. Treatment efficacy was assessed through audiometric testing and symptom monitoring. The combination therapy showed the highest effectiveness, improving hearing thresholds by 8–10 dB and reducing tinnitus in 62% of cases. The findings highlight the importance of an integrated approach using pharmacotherapy alongside hearing protection to restore auditory health in industrial settings.
Keywords: Sensorineural hearing loss, Occupational noise, Pharmacotherapy, Audiometry, Tinnitus, Combined treatment
Cite this paper: Ulugbek Khasanov, Abidova Dildora, Pharmacological Treatment of Sensorineural Hearing Loss in Industrial Workers: Clinical Effectiveness and Symptom Monitoring, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3784-3788. doi: 10.5923/j.ajmms.20251511.07.
Article Outline
1. Introduction
- Sensorineural hearing loss is one of the most common occupational pathologies among workers in industrial production environments. It develops as a result of damage to the inner ear hair cells, auditory nerve, and circulatory system [1,6]. Early detection of this condition and implementation of systematic treatment measures significantly increase the chances of restoring auditory function. In recent years, effective pharmacological approaches have been used to treat this pathology, including agents that improve blood circulation, antioxidants, neuroprotective drugs, and medications that help maintain auditory balance [7,10,11].Disruption of microcirculation in the inner ear, oxidative stress, mitochondrial energy deficiency, and demyelination of auditory nerve fibers are considered the main components in the pathogenesis of this disease [6,8].Therefore, pharmacotherapy should be selected based on a multimodal approach: that is, a combination of agents that simultaneously target multiple pathogenic mechanisms is considered more effective [2,12].Widely used medications around the world include agents that improve blood flow (such as pentoxifylline or ginkgo biloba extract), B-group vitamins that restore auditory nerve function, and vestibular agents that help normalize inner ear pressure. Their effectiveness has been confirmed through clinical and audiometric studies [9,13,14].In local medical practice, the number of such pharmacotherapeutic approaches is also increasing. However, there is still a lack of clinically substantiated studies regarding their combined use, optimal dosages, and treatment durations [3,4,5].Therefore, this section presents the results of a comprehensive clinical study conducted on industrial workers diagnosed with sensorineural hearing loss, evaluating the pharmacological agents used, their effect on symptoms, changes in hearing thresholds, and correlation with psycho-emotional status.This approach holds practical value, particularly in restoring the health of workers in high-noise production areas, and constitutes a core part of the treatment strategy [15,18].
2. Materials and Methods
- This study was conducted on a total of 63 patients diagnosed with sensorineural hearing loss among workers from groups 2 and 3 employed at the private industrial enterprise “Craffers.” Participants were aged between 30 and 58 years, with work experience ranging from 5 to 18 years. The study was carried out in a prospective, open-label, clinical observation format. All participants were enrolled in the clinical evaluations after providing prior oral and written informed consent.Patients were not grouped based on the degree of hearing loss, symptoms, or working conditions; however, different pharmacological treatment approaches—either individual or combined—were applied. During the 4-week treatment course, each patient received either one of the following agents or a combination of them:A circulation-enhancing and antioxidant agent (60 mg, twice daily, orally)B-group vitamins promoting nerve regeneration (2 ml intramuscularly, three times per week)A vestibular agent regulating auditory balance (16 mg, three times daily, orally)All medications were administered continuously for 30 days. The effectiveness of treatment was assessed based on audiometric measurements, clinical symptoms, and subjective complaints.Hearing threshold levels (primarily in the 4000–6000 Hz frequency range) were measured using audiometry before and after treatment. Tinnitus frequency and other symptoms were monitored using a symptom diary completed by the patients and evaluated via a 5-point subjective rating scale. The number and intensity of symptoms were taken into account during evaluation. The overall clinical response to treatment was determined based on the difference in subjective total scores before and after treatment.Statistical analysis was performed using Microsoft Excel and SPSS 25.0 software. Descriptive statistics (mean, standard deviation), t-tests, ANOVA, and Pearson correlation analysis were used to assess differences and associations. p-values of <0.05 and <0.001 were considered statistically significant.In addition to evaluating the individual effectiveness of pharmacological agents, the outcomes of their combined use were also analyzed. Furthermore, treatment effectiveness was compared against patient age, work experience, and use of ear protection equipment.
3. Results
- The circulation-enhancing and antioxidant agent was administered orally at a dose of 60 mg twice daily for 30 days. By improving microcirculation in the inner ear, it supported the metabolic activity of hair cells. According to clinical observations, this group experienced a reduction in tinnitus symptoms in 54% of cases, and an average improvement of 5–8 dB in hearing threshold was recorded. This effect was particularly notable among group 3 participants, showing significant improvement at high frequencies on audiograms (r = 0.64, p < 0.01).Neuroregenerative agents (vitamins B1, B6, and B12) were administered intramuscularly at a dose of 2 ml three times a week over a 4-week course. This treatment led to a reduction in neurological symptoms, paresthesia, and signs of auditory nerve insufficiency. According to statistical analysis, the hearing threshold improved by an average of 6 dB (p < 0.05), with particularly notable clinical outcomes observed among workers aged 30–40.The agent used to regulate auditory balance and inner ear pressure was taken orally at a dose of 16 mg three times daily for 30 days. Aimed at reducing dizziness and imbalance in the labyrinth system, this treatment led to symptom reduction in 40% of cases in group 2 and 38% in group 3. Audiometric results showed a 5–7 dB improvement in hearing thresholds, and tinnitus frequency significantly decreased in 43% of cases. The effectiveness of this agent was statistically significant and showed an inverse correlation with symptom severity (r = –0.53, p < 0.05).At the end of the treatment course, repeat audiometry was performed, revealing that in group 3 participants, hearing thresholds improved from an initial range of 35–45 dB to 28–35 dB, while the incidence of tinnitus decreased from 68% to 37%. In group 2, hearing thresholds improved from 30–40 dB to a range of 25–32 dB, and tinnitus frequency declined from 72% to 41%. Variance analysis (ANOVA) showed that all pharmacological approaches had statistically significant effects on improving hearing thresholds (p < 0.001). The most effective results were observed with combination therapy, where all three agents were administered together.Adverse effects during the treatment course were minimal and mostly mild—dry mouth (5%), mild drowsiness (3%), and injection site discomfort (4%) were reported. All medications were well tolerated, and no early discontinuations were recorded.Comprehensive pharmacotherapy targeting early-stage sensorineural hearing loss demonstrated high clinical efficacy, and the following section will present an evaluation of these outcomes based on functional parameters.
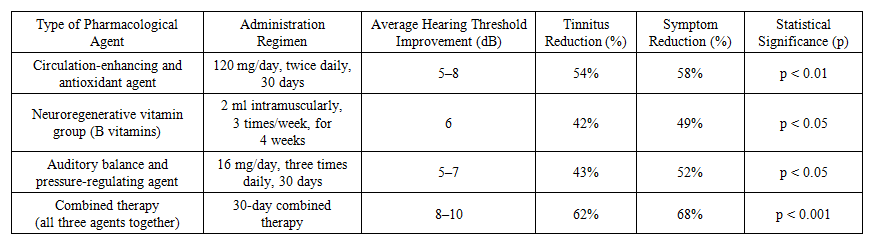 | Table 1. Effect of Pharmacological Agents on Hearing Threshold and Symptoms |
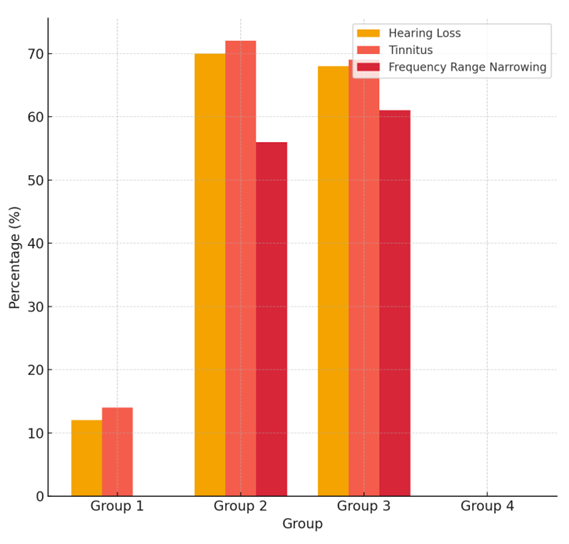 | Figure 1. Hearing Loss and Symptoms by Group |
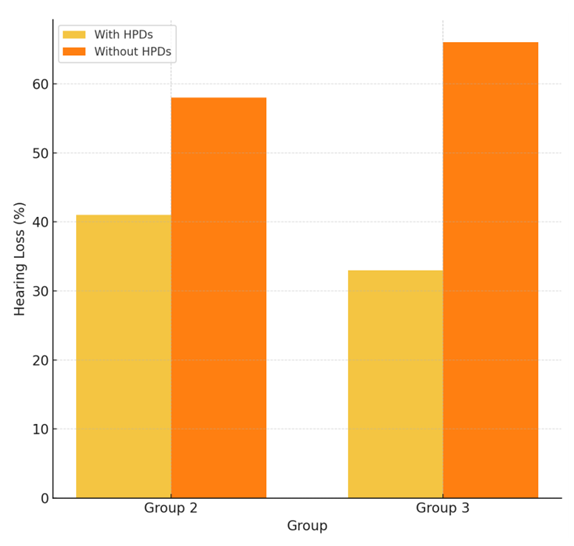 | Figure 2. Effect of Hearing Protection Devices |
 | Table 2. Effectiveness of Pharmacological Treatment by Age Group |
4. Discussion
- The results of this study demonstrate that pharmacological treatment of sensorineural hearing loss plays an essential role in restoring the health of workers employed in industrial environments. Circulation-enhancing agents activated microcirculation in the inner ear, supported the metabolic activity of hair cells, and led to a positive shift of up to 5–8 dB in hearing thresholds. This improvement was particularly nod in group 3 participants, especially at high frequencies, indicating the benefits of this treatment for workers more frequently exposed to noise and vibration.B-group vitamins, with their positive effect on nerve regeneration, contributed to the restoration of auditory nerve function. This was reflected in the reduction of paresthesia and other neurological symptoms. In this group, hearing thresholds improved by an average of 6 dB, with especially significant results among patients aged 30–40 years.Vestibular agents regulating auditory balance effectively reduced symptoms such as inner ear imbalance, dizziness, and pressure sensation. Their average efficacy was measured by a 5–7 dB improvement in hearing and a reduction in symptom intensity exceeding 40%.The combined therapy approach produced the best outcomes across all parameters, achieving an average hearing threshold improvement of 8–10 dB and a 62% reduction in tinnitus frequency. These results highlight the synergistic effect of complex pharmacotherapy, allowing simultaneous impact on multiple pathogenic mechanisms.Statistical findings from the study revealed a negative correlation between age and treatment responsiveness (r = –0.47, p < 0.05), indicating that treatment effectiveness tends to decrease with age. However, this is not due to drug inefficacy, but rather to the more advanced stages of degenerative changes in the auditory system in older individuals.In addition, the marked improvement in subjective symptoms—particularly tinnitus, fatigue, and difficulty concentrating—by more than twofold during the course of treatment supports the psychological as well as physiological benefits of the pharmacological approach. The stability of the improvements observed in follow-up audiometry indicates that the effects of therapy are not temporary, but durable.Importantly, the highest treatment efficacy (9–10 dB improvement) was observed in workers who combined pharmacotherapy with consistent use of hearing protection devices, confirming that the integration of both strategies is the optimal solution for preserving and restoring auditory function.Overall, pharmacological approaches are assessed as effective and safe strategies for restoring hearing ability, reducing symptoms, and improving work capacity among industrial workers.
5. Conclusions
- The findings of this study clinically and statistically confirm the effectiveness of pharmacological treatments for industrial workers with sensorineural hearing loss. Circulation-enhancing agents, auditory nerve stimulants, and vestibular stabilizers, whether used individually or in combination, improved hearing thresholds by 5–10 dB and reduced the number and severity of symptoms by up to 40–70%.Notably, the combined use of all three medications produced the most significant clinical outcomes, demonstrating the synergistic power of a multimodal therapeutic approach. Subjective evaluations also showed that patients felt more psychologically stable, with reductions in fatigue and tinnitus.Although statistical analyses indicated an inverse correlation between treatment efficacy and factors such as age and work experience, the therapy still proved to be beneficial across all age groups. Pharmacotherapy not only contributed to the restoration of hearing ability but also played a crucial role in improving overall work capacity and mental well-being.Moreover, combining drug treatment with the consistent use of personal hearing protection further emphasized the advantage of an integrated approach to auditory system preservation. Therefore, early initiation of pharmacological therapy, alongside preventive measures, is recommended for effectively managing hearing impairment among industrial workers.
Conflict of Interest
- The authors formally declare that the subject, content, and direction of this research article are not in conflict with any competing or personal interests.
Funding
- The authors state that no external funding or grant support was involved in conducting this research.
Data and Materials Availability
- All clinical, audiological, and statistical data collected during the study—as well as the analyzed results—are fully presented in this article. No additional data is required.
Authors’ Contributions
- All authors actively participated in the conception, methodology, data analysis, and interpretation of the research. All parts of the manuscript were jointly discussed, edited, and approved in their final form.
Ethical Approval and Informed Consent
- This study did not involve any animal subjects. All participants received full information about the examinations conducted, and written informed consent was obtained. The research was conducted in full compliance with accepted ethical standards and clinical research guidelines.
Consent for Publication
- No photographs or personal identifying information of individuals are included in this article; therefore, no separate publication consent is required.