-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3779-3783
doi:10.5923/j.ajmms.20251511.06
Received: Oct. 13, 2025; Accepted: Oct. 30, 2025; Published: Nov. 3, 2025

Strengthening Rehabilitation for Children with Moderate Sensorineural Hearing Impairment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNargiza Fattakhova
Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Nargiza Fattakhova, Tashkent Medical Academy, Tashkent, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article examines modern approaches to strengthening auditory-verbal rehabilitation in children with moderate sensorineural hearing impairment. A clinical study conducted at the Tashkent Medical Academy demonstrated the high effectiveness of an individualized program that included digital hearing aids, regular speech therapy sessions, auditory training, and psychosocial support. Children who received comprehensive rehabilitation showed significantly better outcomes in auditory perception, speech development, and social adaptation compared to the control group.
Keywords: Sensorineural hearing impairment, Auditory-verbal rehabilitation, Children, Hearing aids, Speech therapy, Auditory training, Social adaptation
Cite this paper: Nargiza Fattakhova, Strengthening Rehabilitation for Children with Moderate Sensorineural Hearing Impairment, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3779-3783. doi: 10.5923/j.ajmms.20251511.06.
Article Outline
1. Introduction
- Sensorineural hearing impairment (SNHI) represents a persistent deficit of auditory function caused by damage to the inner ear structures, the auditory nerve, or central auditory pathways. In children, this pathology has particular significance, as hearing plays a decisive role in the development of speech, cognitive processes, and successful social adaptation [1]. According to the World Health Organization, more than 34 million children worldwide live with hearing loss, and over 60% of these cases could be prevented or effectively managed through timely interventions [2].A growing concern is the rising number of cases of SNHI identified in early childhood, often linked to adverse environmental conditions, perinatal complications, intrauterine infections, hereditary factors, and insufficient prenatal diagnostics in certain regions [3]. Among all types of hearing loss, moderate sensorineural impairment (41–55 dB) is especially insidious, as it may remain unnoticed for a long time, particularly in children who have not yet developed active speech. The absence of timely detection and correction leads to secondary delays in speech and intellectual development, reduced learning ability, and, later in life, social and professional limitations [4].In this context, strengthening rehabilitation strategies has become one of the most urgent tasks in pediatric otorhinolaryngology, speech therapy, and special education. While approved clinical protocols exist, their effectiveness often remains limited due to late diagnosis and a lack of systematic approaches that consider age-related, neurological, and psycho-emotional characteristics of children [5] [6].Contemporary research highlights that the most successful outcomes can be achieved through multidisciplinary collaboration between otorhinolaryngologists, audiologists, speech therapists, neurologists, and child psychologists. Such integrated rehabilitation not only restores sound perception but also ensures the acquisition of speech, socialization, and quality of life [7]. Strengthening and expanding these approaches today represents an essential direction in both clinical practice and scientific research.
2. Materials and Methods
- The study was conducted at the Department of Otorhinolaryngology of the Tashkent Medical Academy between 2022 and 2024. A total of 80 children aged 3–7 years with a confirmed diagnosis of moderate sensorineural hearing impairment (Grade II, 41–55 dB) were enrolled. The participants were divided into two equal groups of 40 children each: the main group (Group I) and the control group (Group II). Allocation was performed taking into account age, sex, severity of impairment, and the presence of comorbid somatic conditions.The main group received a strengthened rehabilitation program, which included:individualized fitting and adjustment of modern digital hearing aids;regular speech therapy sessions with a speech-language pathologist (at least three times per week);auditory training based on specialized acoustic stimulation protocols;psycho-emotional support, involving both a child psychologist and parental counseling;continuous medical supervision (pediatrician, neurologist, otorhinolaryngologist).The control group underwent standard therapy consisting only of hearing aid fitting and occasional speech therapy sessions (no more than once per week).To assess the effectiveness of rehabilitation, the following methods were applied:Audiological diagnostics: pure-tone threshold audiometry and measurement of auditory thresholds before and after intervention;Speech assessment: evaluation of phonemic hearing, active and passive vocabulary, and connected speech;Cognitive and social adaptation: assessment of memory, attention, and group adaptation using the Social Behavior Scale (SocD);Parental perception: structured questionnaire assessing satisfaction with rehabilitation outcomes;Dynamic monitoring: three checkpoints—baseline (T0), after 6 months (T1), and after 12 months (T2).All data were recorded in individual observation charts. Results were analyzed using descriptive statistics, and intergroup comparisons were carried out with Student’s t-test. Statistical significance was set at p < 0.05.Thus, the study design allowed for evaluation not only of objective measures of hearing and speech, but also of social integration dynamics and parental feedback, providing a comprehensive picture of rehabilitation effectiveness.
3. Results
- Children in the main group demonstrated significant progress. The mean auditory threshold improved from 50.2 dB to 37.1 dB (p < 0.01), the active vocabulary increased 1.5-fold, and notable improvements were observed in pronunciation and grammatical structure of speech. In the control group, changes were less pronounced and statistically insignificant. Social adaptation improved in 87% of children in the main group compared to 58% in the control group. Parental satisfaction with rehabilitation outcomes was also higher in the main group (91% vs. 63%).After 12 months of observation, children with moderate SNHI (Grade II) in the two comparative groups showed distinct differences. The main group, which received the strengthened and individualized rehabilitation program, demonstrated marked positive dynamics across all key parameters—auditory perception, speech development, and social adaptation—while the control group showed only limited improvements.The Basic Hearing Scale (BHS), which reflects perception of speech and background sounds, confirmed these findings. In the main group (Group I), the mean score increased from 15.9 at baseline (T0) to 17.5 after 6 months (T1) and 19.0 after 12 months (T2), corresponding to a gain of +3.1 points. In contrast, the control group (Group II) demonstrated only a modest improvement, from 14.9 at baseline to 15.7 at 6 months and 16.8 at 12 months, yielding an overall gain of just +1.9 points. The difference between the groups at the final stage was statistically significant (p < 0.05).
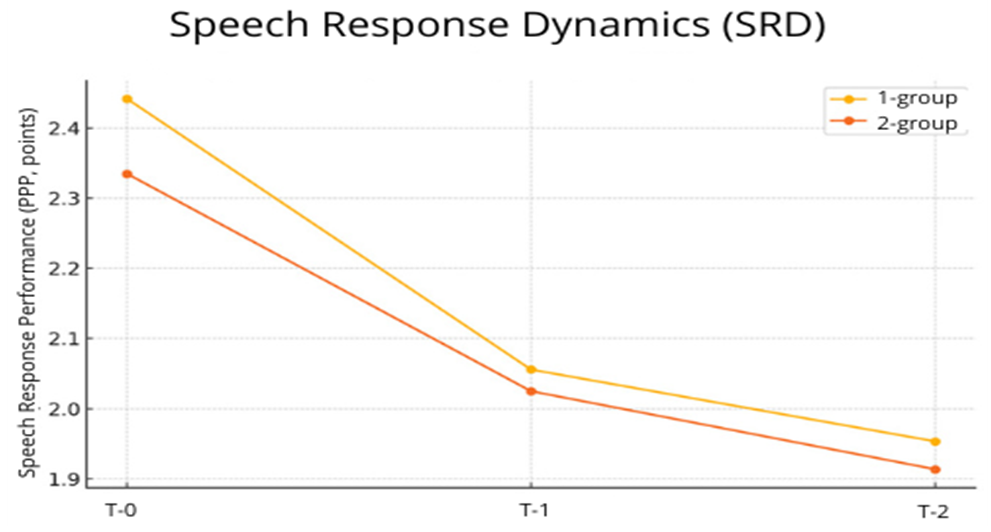 | Figure 1. Dynamics of auditory perception (BHS) across three observation stages: baseline, after 6 months (T1), and after 12 months (T2) |
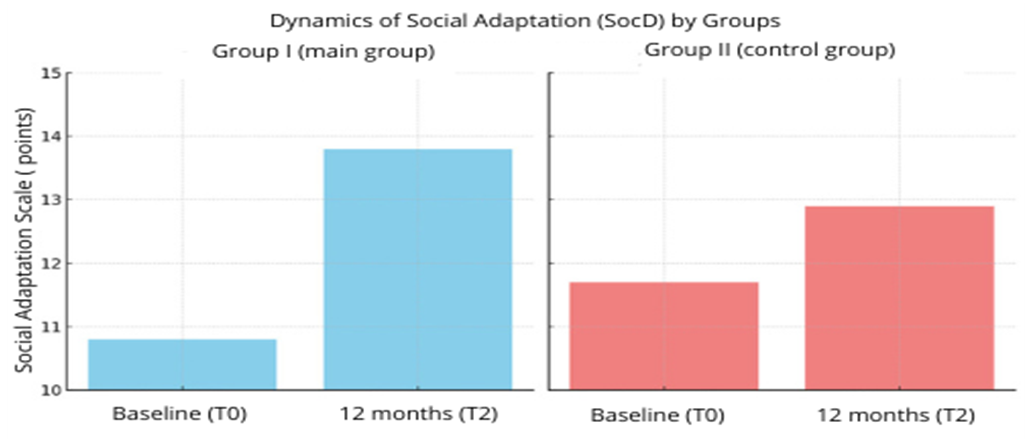 | Figure 2. Dynamics of social adaptation (SocD) in children of the main and control groups over 12 months |
|

|

4. Discussion
- The results of this study confirm the high effectiveness of a strengthened comprehensive auditory-verbal rehabilitation program for children with moderate sensorineural hearing impairment. Children in the main group demonstrated significant improvements in auditory, speech, and social skills compared to those in the control group who received standard therapy. These findings are consistent with reports from other studies emphasizing the advantages of a multidisciplinary approach [1,4,5].The most notable difference was observed in auditory perception: over the 12-month period, the Basic Hearing Scale (BHS) increased by an average of +3.1 points in the main group, compared to only +1.9 points in the control group. This highlights the importance of individualized hearing aid fitting and regular auditory training aimed at enhancing auditory perception and phonemic awareness [2,6].Speech development also showed statistically significant improvement in the main group. The 0.5-point reduction in SRR over one year reflects more stable speech skills, expansion of vocabulary, and the ability to produce connected speech. In contrast, the changes in the control group were minimal, likely due to the limited intensity of speech therapy sessions.Particular attention should be paid to social adaptation (SocD), which improved by +3.0 points in the main group, as confirmed by graphical analysis. These gains can be attributed to the involvement of a child psychologist in the rehabilitation process, as well as systematic training of parents in communication strategies with hearing-impaired children. Social inclusion, emotional intelligence, and communication skills proved to be highly responsive to psycho-emotional support, a trend also supported by other research in this field [3,7].Overall, the findings not only confirm the relevance of implementing a strengthened, multimodal rehabilitation model, but also emphasize the need for its adaptation to the individual characteristics of each child. Such an approach enables not only compensation for auditory deficits but also the prevention of secondary complications related to emotional development, learning potential, and social integration.
5. Conclusions
- Based on the clinical study conducted, the following conclusions can be drawn:Strengthened auditory-verbal rehabilitation with an individualized approach—including modern digital hearing aids, regular speech therapy, auditory training, and psychosocial support—proved to be more effective than the standard scheme of care for children with moderate sensorineural hearing impairment.Children in the main group demonstrated significant improvement in auditory perception (+3.1 points), speech development (SRR reduction by –0.5 points), and social adaptation (+3.0 points), whereas progress in the control group was significantly lower.The introduction of multimodal methods into pediatric otorhinolaryngology and speech therapy practice substantially improves the quality of life of children with hearing loss, supports successful social integration, and contributes to the formation of a well-rounded personality.The findings underscore the importance of early initiation of rehabilitation (preferably before the age of 4), interdisciplinary collaboration among specialists, and active parental involvement in restoring auditory-verbal functions.The strengthened rehabilitation program presented in this study may be recommended for broad implementation in audiology and speech therapy centers, as well as for adaptation within public healthcare institutions engaged in the rehabilitation of children with hearing impairments.
Conflict of Interest
- The authors declare that the subject, content, and direction of the research presented in this article do not conflict with any competing or personal interests.
Funding
- The authors confirm that no external funding sources or grant support were involved in conducting this research.
Data and Material Transparency
- All clinical, audiological, and statistical data collected and analyzed within the framework of this study are fully presented in the article. No supplementary materials are required.
Authors’ Contribution
- All authors actively contributed to the development of the research concept, formulation of methodology, analysis of results, and preparation of conclusions. Each section of the article was jointly discussed, revised, and approved by all co-authors.
Ethical Standards and Informed Consent
- This study did not involve experiments on animals. All participants were fully informed about the procedures, and written informed consent was obtained. The research was conducted in strict accordance with established ethical standards and clinical research norms.
Consent for Publication
- The article does not contain photographs or personal data that could identify study participants; therefore, separate consent for publication was not required.
Publisher’s Note
- Eurasian Journal of Otorhinolaryngology – Head and Neck Surgery (https://ejohns.scinnovations.uz) remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.