-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(11): 3769-3774
doi:10.5923/j.ajmms.20251511.04
Received: Oct. 6, 2025; Accepted: Oct. 28, 2025; Published: Nov. 3, 2025

The Early and Long-Term Postoperative Outcomes in Children with Ileostomy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkilov Kh. A.1, 2, Primov F. Sh.1, 2, Urmanov N. T.2, Yuldashev T. A.2, Fayziev A. M.1, 2
1Center for the Development of Professional Qualification of Medical Workers, Tashkent, Uzbekistan
2Republican Research Centre of Emergency Medicine, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

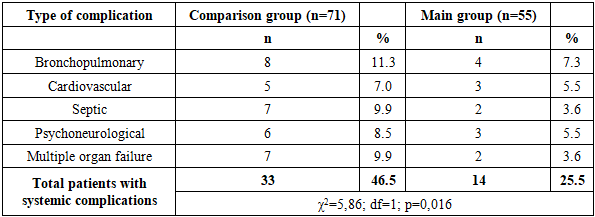
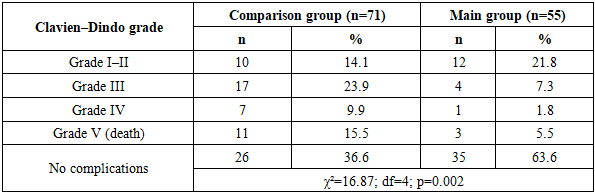
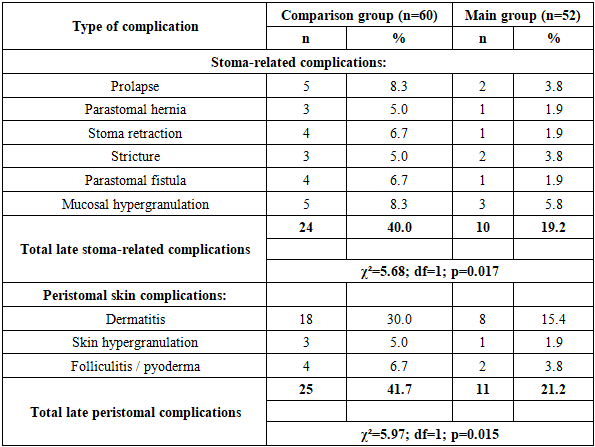
Objective. To evaluate and compare management strategies for pediatric patients with ileostomies, with a focus on the effectiveness of a comprehensive rehabilitation program in reducing postoperative complications and improving recovery. Methods. A total of 126 children with ileostomies treated from 2014 to 2024 were analyzed. The comparison group (n=71) included patients managed between 2014–2019 with conventional approaches, while the main group (n=55) received an optimized protocol from 2020 onwards. This program included structured parent and patient education, individualized stoma care, combined antiseptics, protective films, absorbent dressings, low-intensity laser therapy, and rational nutritional support. Outcomes assessed were early and late stoma complications, systemic morbidity, hospital stay, and frequency of reconstructive operations. Statistical significance was set at p<0.05. Results. Early stoma-related complications occurred in 53.5% of the comparison group versus 27.3% of the main group (p=0.003). Systemic complications decreased from 46.5% to 25.5% (p=0.016). Severe (Clavien–Dindo grade III–V) complications were more frequent in the comparison group (49.3% vs. 14.6%, p=0.002). Late stoma complications decreased from 40.0% to 19.2% (p=0.017), and peristomal skin problems from 41.7% to 21.2% (p=0.015). The mean postoperative hospital stay was shorter in the main group (11.5 ± 0.35 vs. 13.2 ± 0.5 days, p<0.001). A greater proportion of patients in the main group underwent timely reconstructive surgery, while persistent functioning stomas were more frequent in the comparison group (16.7% vs. 3.8%). Conclusion. A comprehensive rehabilitation strategy integrating advanced local and systemic measures significantly reduced complication rates, improved intestinal recovery, shortened hospitalization, and enhanced long-term outcomes in children with ileostomies.
Keywords: Children, Ileostomy, Stoma complications, Surgical outcomes, Rehabilitation, Postoperative care, Reconstructive surgery
Cite this paper: Akilov Kh. A., Primov F. Sh., Urmanov N. T., Yuldashev T. A., Fayziev A. M., The Early and Long-Term Postoperative Outcomes in Children with Ileostomy, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3769-3774. doi: 10.5923/j.ajmms.20251511.04.
1. Introduction
- Ileostomies in children are an essential tool in the pediatric surgeon’s armamentarium, allowing life-saving intervention in severe congenital and acquired intestinal pathologies. Accurate epidemiological data remain limited; however, estimates suggest that the overall morbidity associated with stoma creation and closure ranges from 20% to 38% of pediatric patients [1,2,3,4].In pediatric practice, intestinal stomas are formed for a number of common conditions. In neonates, the most frequent indications include necrotizing enterocolitis, intestinal atresia, anorectal malformations, and Hirschsprung’s disease. In older children, severe forms of inflammatory bowel disease may also necessitate ileostomy formation [2,5].The creation of a diverting intestinal stoma allows temporary decompression or bypass of the affected bowel segment, promotes anastomotic healing, and improves the child’s condition prior to restorative surgery. In most cases, pediatric ileostomies are temporary and are scheduled for closure once the patient is stabilized and the primary pathology has been addressed [1,5,6].Despite their undeniable benefits, the presence of an intestinal stoma significantly complicates the management of pediatric patients. Even temporary ileostomies, functioning for only several weeks or months, carry a high risk of complications and demand meticulous care. According to various studies, the overall incidence of postoperative problems may reach 70% or more [4,6,7,8].Common complications include peristomal skin irritation, electrolyte imbalances due to high-output stomas, stoma prolapse or retraction, strictures, as well as infections and nutritional deficiencies in children. Such complications increase the length of hospital stay, the frequency of readmissions, and the overall burden on families [4,7,8]. All of this highlights the importance of optimizing strategies for the management of children with intestinal stomas.In recent years, active discussion has focused on the optimal timing of ileostomy closure, preventive measures against complications, and rehabilitation strategies; however, no unified approach has yet been established. In this context, the present comparative study was conducted to evaluate tactical approaches aimed at improving treatment outcomes in children with ileostomies.
2. Materials and Methods
- The study was based on the results of examination and treatment of 126 children with ileostomy who were managed in the Department of Pediatric Surgery at the Republican Scientific Center of Emergency Medical Care (Tashkent, Uzbekistan) during the period from 2014 to 2024.Inclusion criteria were: the presence of intestinal pathology leading to dynamic obstruction; sequelae of abdominal trauma with intestinal disruption; purulent-inflammatory diseases of the abdominal cavity; adhesive processes; and other conditions requiring the formation of an intestinal stoma.Exclusion criteria were: malignant processes of the abdominal organs, as well as malignant transformation of ulcerative intestinal lesions.The age of patients ranged from newborn to 18 years. The overall cohort included 91 boys (72.2%) and 35 girls (27.8%). All patients were divided into two clinical groups. The comparison group included 71 children (56.4%) treated between 2014 and 2019 (retrospective part of the study). The main group consisted of 55 children (43.6%) who received treatment using an optimized comprehensive rehabilitation program.By sex distribution, in the comparison group boys accounted for 67.6% (n=48) and girls for 32.4% (n=23); in the main group these proportions were 78.2% (n=43) and 21.8% (n=12), respectively. In both groups, the majority of patients were school-age children (8–12 years).The most frequent indication for intestinal stoma formation was ulcerative colitis, observed in 36 patients (27.8%): 22 (31.0%) in the comparison group and 14 (25.5%) in the main group. The second most common cause was Crohn’s disease (21 cases, 16.7%). The third most frequent was small bowel intussusception (18 cases, 14.3%). Less common indications included small bowel atresia (7.9%), Hirschsprung’s disease (7.1%), and anorectal malformations (7.1%). A rare indication was adhesive small bowel obstruction (3.2%).The distribution of patients according to the urgency of surgery was approximately equal: emergency procedures accounted for 48.4% (n=61), while elective surgeries comprised 51.6% (n=65). No significant differences between the groups were identified for this parameter.The most common complication preceding stoma formation was intestinal obstruction, diagnosed in 75 children (59.5% of the total cohort). Less frequent were intestinal strictures (29.4%), recurrent bleeding episodes (27.8%), perforation (13.5%), and bowel necrosis (4.0%).Comorbid conditions were recorded in 51 children (40.5%). Among them, the most frequent were alimentary and nutritional disorders (13.5%), congenital malformations and central nervous system diseases (8.7% each), as well as urinary tract and bronchopulmonary pathologies.With respect to localization of the pathological process, multiple lesions of the colon were noted in 60 children (47.6%). Isolated involvement of the sigmoid colon was observed in 21 patients (16.7%), the descending colon in 17 (13.5%), and the rectum in 12 (9.5%). Less frequently, changes were registered in the cecum (5.6%) and ascending colon (4.0%).In the overall cohort, a single-barrel stoma was created in 56 patients (44.4%), while a double-barrel stoma was formed in 70 patients (55.6%). No significant differences between the groups were identified for this parameter: the proportion of double-barrel stomas was 54.9% in the comparison group and 56.4% in the main group.Thus, both groups of patients were comparable in terms of age, sex, structure of primary and comorbid pathology, localization of lesions, and type of intestinal stoma formed, which allows for a valid comparison of the effectiveness of the applied therapeutic and rehabilitative approaches.An analysis was conducted of surgical protocols, the type of intestinal stoma created, and the frequency and structure of repeat and restorative procedures. Complications in children with ileostomies were classified as early (within 30 days after surgery) and late (after 30 days), as well as local (stoma-related) and systemic.To evaluate outcomes and complications, the Clavien–Dindo classification (2004) was applied, which allowed for the standardization of postoperative complication severity and facilitated comparison of results between the study groups [9].Optimized management of children with ileostomies was carried out within the framework of a specially developed comprehensive surgical rehabilitation program. This approach included both local and general care measures.Local care involved educating parents and patients in hygiene practices, individual selection of ostomy appliances, antiseptic treatment of the peristomal area, the use of protective pastes, films, and creams, as well as the application of low-intensity laser therapy to stimulate tissue regeneration and prevent inflammatory complications. In cases of peristomal dermatitis, pyoderma, or erosive-ulcerative lesions, combined antiseptics, dressing applications, and specialized wound care materials were used.In the event of surgical complications (bleeding, necrosis, evisceration, abscess, phlegmon, bowel retraction, prolapse, parastomal hernia, or stricture), specialized inpatient management was undertaken with the possibility of operative correction.General care was aimed at nutritional correction with the inclusion of agents for restoring intestinal microbiota, monitoring and consultations with specialized physicians, dynamic control of the intestinal microbiocenosis with the use of probiotics (bifidobacteria and lactobacilli), as well as timely management of comorbid conditions. In complicated cases, children were hospitalized in specialized inpatient units, where they received multicomponent therapy, including intensive supportive care and preparation for the reconstructive stage.Thus, the management program for the main group combined modern methods of preventing and treating stoma-related complications, the use of innovative laser therapy technologies, and a multidisciplinary approach with an emphasis on early rehabilitation and improved outcomes.Statistical analysis included descriptive methods (mean values, standard errors, relative measures), as well as comparative analysis using the χ² test and Student’s t-test. Differences were considered statistically significant at p< 0.05.
3. Results
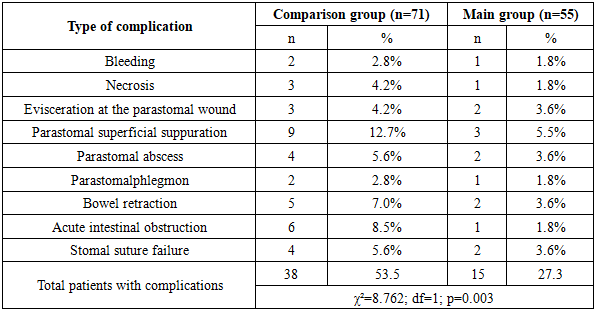
- In the comparison group, complications were recorded in 53.5% of patients (38 cases), whereas in the main group they occurred in only 27.3% (15 cases) (χ²=8.762; df=1; p=0.003). The most common complications were parastomal superficial suppuration (12.7% vs. 5.5%), acute intestinal obstruction (8.5% vs. 1.8%), and bowel retraction (7.0% vs. 3.6%) (Table 1).
|
|
|
|
|
4. Discussion
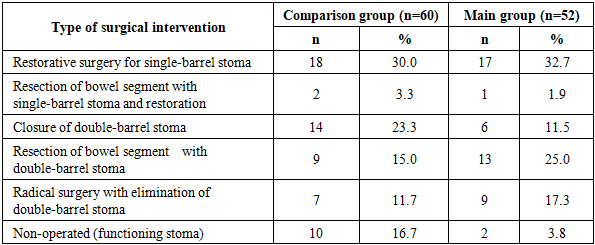
- The findings demonstrate that the introduction of a comprehensive rehabilitation program in the pediatric population significantly shortens the time to restorative operations in patients with both single- and double-barrel stomas. This improvement is associated with enhanced preoperative preparation, a reduction in complication rates, and accelerated healing processes. These results highlight the importance of rehabilitation programs in improving surgical outcomes and enhancing the quality of life of children with intestinal stomas.The overall incidence of any complications (including mild ones) in children with intestinal stomas can exceed 70%, as noted in several studies [10–13]. A considerable proportion of children with ileostomies experience complications both during the functioning period of the stoma and at the stage of its closure. According to a retrospective analysis of 336 cases, severe stoma-related complications (Clavien–Dindo grade III and higher) occurred in 39% of children under 3 years of age [14]. Moreover, even after planned stoma closure, serious problems such as anastomotic leakage, hernias, and adhesive obstruction were reported in 23% of patients [14].It is important to emphasize that ileostomies themselves carry a higher risk of complications compared to colostomies. It has been shown that the presence of an ileostomy is an independent factor increasing the likelihood of severe complications in children, with the relative risk of complications rising approximately 2.5-fold [2,4]. This is attributed to the more liquid and aggressive composition of intestinal effluent from the ileum, which leads to dehydration, electrolyte imbalance, and skin damage.Excessive stoma output represents one of the most serious complications in young children, potentially leading to malabsorption and intestinal failure. However, to date, there are no standardized protocols for the prevention and management of this condition in pediatric patients. A 2024 systematic review confirmed the complete lack of high-quality studies addressing the management of high-output enterostomies in children [15]. The authors emphasize the need for the development of multistage conservative strategies—including rational restriction of nutrition and fluid intake, the use of oral rehydration solutions, chyme reinfusion, and pharmacological therapy—to reduce stoma output and prevent both acute and chronic complications.In the absence of an evidence base, current treatment relies on specialist experience. Practical measures include strict monitoring of fluid balance, the administration of stool-thickening agents and medications that reduce intestinal motility, as well as the initiation of the earliest possible enteral feeding to stimulate small bowel adaptation.One of the key goals of tactical decision-making is to minimize the length of hospitalization for the child. Different approaches may affect this parameter. A particular issue under discussion is how the timing of ileostomy closure influences hospital stay and overall recovery. Our study demonstrated that earlier stoma closure allows for a reduction in the total duration of treatment without increasing patient risk. This is consistent with international data.In a retrospective review of necrotizing enterocolitis cases, groups were compared according to the interval before ileostomy closure: less than 8 weeks, 8–12 weeks, and more than 12 weeks [16]. It was noted that early closure (within 2 months) resulted in a somewhat longer postoperative hospitalization (explained by the lower weight and immaturity of these infants); however, the overall duration of treatment from stoma formation to final discharge did not differ significantly between groups [16]. At the same time, the rate of postoperative complications was not affected by the timing of closure—neither early nor delayed restoration of intestinal continuity increased the risk of anastomotic leakage or infections [16].Moreover, several studies indicate that unjustifiably prolonged maintenance of a temporary ileostomy may be associated with the accumulation of stoma-related problems, such as impaired growth and electrolyte disturbances. For example, when comparing traditional closure times (8–12 weeks) with earlier closure (around 4 weeks) in children, the latter group demonstrated an even lower overall incidence of stoma-related complications, although wound-related infectious complications were somewhat more frequent [17].Our results are consistent with these findings: provided that strict selection criteria are observed—stable general condition of the child, adequate body weight, absence of active infection, and no ongoing need for decompression of the distal bowel—early restoration of intestinal continuity does not worsen outcomes. On the contrary, stoma closure facilitates child care, improves nutrient absorption, and contributes to more rapid weight gain in the postoperative period.Criteria for stoma closure in pediatrics are primarily based on the child’s readiness for repeat surgery and sufficient recovery after the initial intervention. There are no absolute rigid timelines in international practice, and management varies depending on the clinical situation. According to surveys of pediatric surgeons in the United Kingdom, the most common target for stoma closure is approximately six weeks after its creation [18,19]. However, in reality, the timing may differ, with decisions influenced by factors such as the child’s nutritional status and weight gain, the presence or absence of stoma-related complications (e.g., skin problems or prolapse), as well as the activity of the underlying disease [18,19].A systematic review of the literature has shown that delaying definitive surgery and stoma closure in such patients does not provide clear advantages [18–20]. Prolongation of stoma function is justified only in the presence of strict medical indications, whereas restoration of intestinal continuity as early as feasible is increasingly regarded as the standard of care.The accumulated experience and the results of our study confirm that tactical details—from patient preparation and timing of surgery to the choice of closure technique—significantly influence treatment outcomes. In light of the obtained data, our findings can be interpreted as consistent with current international trends in the management of children with ileostomies.Over the past decade, international research has demonstrated that strategies focusing on early stoma closure, comprehensive rehabilitation, and prevention of complications yield better outcomes. Our study, comparable to systematic reviews and clinical trials, provides further evidence in favor of refining treatment strategies: an individualized approach to ileostomy closure in children, combined with multidisciplinary support, can reduce the incidence of complications, accelerate recovery, and improve quality of life in the pediatric population.This study has several limitations. First, the sample size was limited, which reduced the ability to perform detailed stratification by nosological forms, age categories, and severity of patient condition. Second, part of the data obtained in the comparison group was retrospective, which does not exclude the possibility of systematic errors related to incomplete documentation and limited availability of information on certain clinical parameters. Third, the study was single-center in nature, which necessitates confirmation of the findings in multicenter studies involving larger patient cohorts.
5. Conclusions
- The implementation of a comprehensive rehabilitation strategy, incorporating advanced methods of local and systemic treatment, significantly reduces the incidence of complications, improves intestinal recovery, shortens the duration of hospitalization, and enhances the outcomes of surgical rehabilitation in children with ileostomies.