Shomurodov Xurshid Shokirovich, Narzullaev Nuriddin Umarovich
Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan
Correspondence to: Shomurodov Xurshid Shokirovich, Bukhara State Medical Institute named after Abu Ali Ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The traditional symptoms of strokes are the sudden, apoplectiform development of the disease, fainting, and the simultaneous occurrence of neurological signs (usually paralysis). Characteristic of cerebral infarction are the signs that come before, such as an increasing impairment of functions, fainting at the beginning of the disease. However, the disease rarely occurs in this form.
Keywords:
Ischemic stroke, Immunocorrection, Serum, Cytokine content, Dynamic changes
Cite this paper: Shomurodov Xurshid Shokirovich, Narzullaev Nuriddin Umarovich, Dynamic Changes in Serum Cytokine Levels from Immunocorrection in Patients with Ischemic Stroke, American Journal of Medicine and Medical Sciences, Vol. 15 No. 11, 2025, pp. 3764-3768. doi: 10.5923/j.ajmms.20251511.03.
1. Introduction
In the acute period of strokes, the mortality rate has been rising to a high level. This is due to the severity of strokes, clinical course, as well as the presence of side diseases at the stage of concomitant decompensation. Low quality of care is also a contributing factor in this category of patients. Concomitant complications also affect mortality rates. Ischemic stroke complications in patients over the age of 70 are 62%, in turn 40% in ischemic stroke. Cranial vascular disease is currently one of the most serious medical and social problems in the world. According to WHO data in 2019, about 6.5 million people in the world die every year from brain strokes or other forms of cerebrovascular disease (10.8% of the total number of deaths). Death is the second most common in tserebrovascular diseases, after heart disease, and it is 8% in men and 16% in women. In western Europe, an average of 33,000 euros per year is spent on the treatment, rehabilitation and Prevention of a patient with a brain stroke [1,3,5,7,9,11,13,15].The purpose of the study. assessment of dynamic changes in serum cytokine levels from immunocorrection in patients with ischemic stroke. As an object of research, RSHTYOIM was carried out in the Department of neuroreanimation of the Bukhara branch in 2022-2025 in 137 patients who were treated with the diagnosis of ischemic stroke.
2. Results and Analyzes
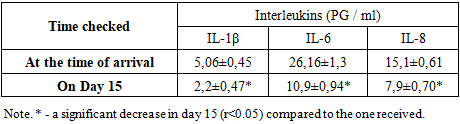
In order to assess the indicators of the systemic immune response of the body, the amount of serum cytokines (il-1β, il-6, and il-8) from 25 patients from each group was studied by the method of solid-phase immunoferment analysis (IFA) using a set of reagents ("vector-Best," Russia). Patients with deep disorders of esophageal sopor-coma I and psychomotor arousal were treated according to standard protocols using anti-cranial, membranastabilizing, antioxidant, sedative, anticoagulant, and antiagregant group drugs. When studied on the 15th day of treatment in the main group of patients with II who used immunocorrectional therapy (Acridopheron) in addition to standard therapy, the incidence of serum anti-inflammatory cytokines was lower compared to the rates studied when hospitalized. At the same time, significant reductions in the following cytokines were noted: il-1β 2.3 times (2.2±0.47 PG/ml versus 5.06±0.45 PG/ml); il-6 2.4 times (26.16±1.3 PG/ml versus 10.9±0.94 PG/ml); il-8 1.9 times (15.1±0.61 PG/ml versus 7.9±0.70 PG / ml. At the same time, clinical indicators have also improved: clarity of consciousness, patient access to communication, orientation in space and time, stabilization of hemodynamics, swallowing recovery, improved independent adequate breathing, improved plegian position in the limbs up to paresis. In addition to standard therapy, immunocorrectional therapy has been used in the main group of patients with ischemic stroke, dynamic changes in the content of serum cytokines (PG/ml) (Table 1).Table 1. In patients with II in the main group of patients indications of serum interleukins after immunocorrigiratory therapy
 |
| |
|
In addition to standard therapy, dynamic changes in the content of serum cytokines in ischemic stroke in patients of the main group, in which immunocorrectional therapy is used, are described in Figure 1.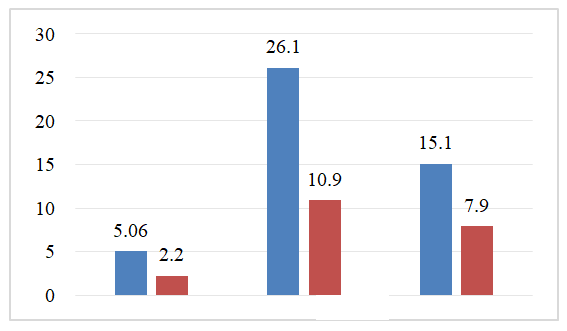 | Figure 1. Dynamic changes in the content of serum cytokines in ischemic stroke in patients of the main group, in which immunocorrectional therapy is used |
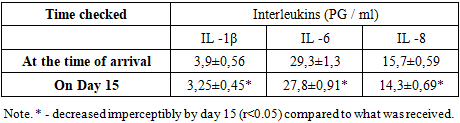
In the comparison group (traditionally treated but not receiving immunocorrigiratory therapy), patients with II on the 15th showed a gradual caesarean section decrease with the data at the time of taking serum inflammatory cytokine levels: in this il-1β 1.2 times (3.25±0.45 PG/ml versus 3.9±0.56 PG/ml); il-8 1.1 times (15.7±0.59 PG/ml versus 14.3±0.69 pg/ml); meanwhile, a 1.1-fold decrease in IL-6 levels has been recorded (27.8±0.91 pg/ml versus 29.3±1.3 pg/ml) (R<0.05). Dynamic changes in the content of blood serum cytokines (PG/ml) (Table 2) of patients with ischemic stroke in the comparison group, in which standard therapy is used without the use of immunocorrectional therapy.Table 2. Dynamic indicators of serum interleukins (not taking immunocorrigiratory therapy) in patients with ischemic stroke in patients of the comparison group
 |
| |
|
Dynamic changes in serum cytokine content of patients with ischemic stroke in the comparison group, in which traditional standard therapy is used without taking immunocorrectional therapy, are graphically illustrated in Figure 2.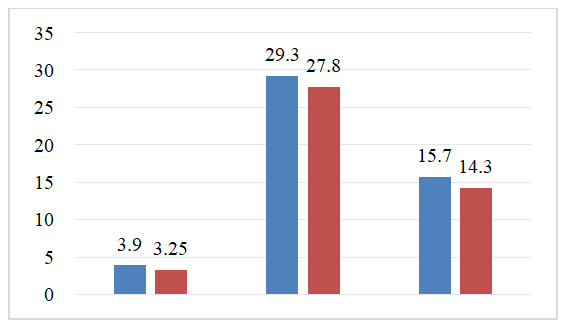 | Figure 2. Dynamic changes in the content of tsitokins in the blood serum of patients with ischemic stroke in the comparison group in which standard therapy is used |
Thus, in the group of patients with ischemic stroke, with standard therapy, the main inflammation was obtained, and there was no significant decrease in the level of anti-inflammatory cytokines il-1β, il-6 and il-8. In the main group, where immunocorrectional therapy was used, these indicators were significantly lower. Comparison of the content of serum il-6 cytokine in the main (immunocorrigiratory therapy received) and comparison (standard traditionally treated) group of patients with ischemic stroke clearly shows the dynamics of decline, which once again confirms the effectiveness of immunocorrectional therapy in comparison with standard therapy (Figure 3).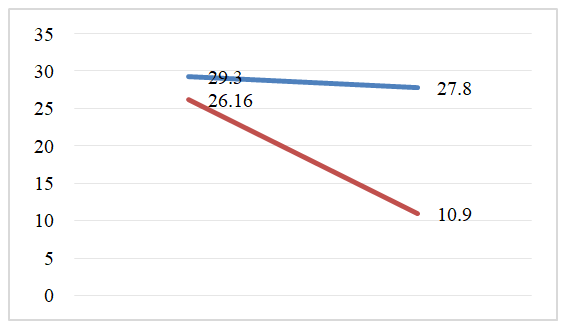 | Figure 3. Dynamic indicators of the content of il-6 in the blood on the 1st and 15th days of treatment in the main group receiving immunocorrectional therapy with II and in the comparison group receiving standard conventional therapy |
The main and comparison group shows a difference in favor of the dynamic decrease in serum IL-8 cytokine, as well as the effectiveness of immunocorrectional therapy compared to the use of standard therapy (Figure 4).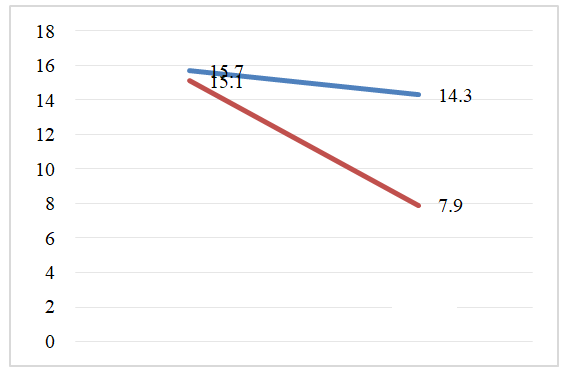 | Figure 4. Dynamic indicators of the content of il-8 in the blood on the 1st and 15th days of treatment in the main group receiving immunocorrectional therapy with ischemic stroke and in the comparison group receiving standard conventional therapy |
In the main group, by the 15th day after immunocorrectional therapy, there was a significant decrease in the level of cytokines such as il-1β, il-6, il-8 in the central peripheral blood, compared with the indicators on the first day taken. In particular, serum il-1β levels decreased 2.3 times and on the 15th day of treatment were 2.2±0.47 PG/ml compared to 5.06±0.45 PG/ml; il-6 decreased 2.4 times and was 10.9±0.94 PG/ml compared to 26.16±1.3 PG/ml. Il-8 decreased 1.9 times and was 7.9±0.70 PG/ml compared to 15.1 ±0.61 PG/ml. Monitoring serum il-6 levels of patients with ischemic stroke and comparing them with the clinical features of stroke makes it possible to note a number of features of cytokine dysbalance in the acute period of the disease. Regardless of the option of withdrawal of II, on the 1st day of the disease, the amount of IL-6 in the blood serum is higher than that of healthy people and reaches its peak on the 5th-10th days of the disease. At the same time, it has been noted that il 6 levels are directly related to the volume of cerebral infarction – ischemia [2,4,6,8,10,12,14]. The jump in the content of this cytokine is determined by the pathogenetic role of a participant in local and systemic inflammation, accompanied by a tumor around his cerebral ischemia. At the same time, the negative prognostic significance of il-6 as a dangerous marker of the immune system is associated with the activating effect on the severity of the inflammatory process in the brain. Thus, the results of the study of the features of the cytokine profile at the systemic and local level showed that ischemic stroke received inflammation and is accompanied by hypersecretion of anti-inflammatory cytokines, the production of which has significant features in the dynamics of the development of the inflammatory process caused by ischemia (blood thinning) in brain tissues. On the 1st day after ischemia, there was a significant increase in the concentration of cytokines using serum inflammation (il-1β, il-6, il-8). Such production of inflammatory mediators and an increase in the amount of cytokines in the blood serum can be assessed as an adequate initial reaction of the immune system to neuroimaging and the development of brain tumors to brain ischemia.In the 1st day after ischemic stroke, in addition to il-6 and il-8 in dynamics, a slight increase in the amount of cytokines studied in the blood serum was observed, the concentration of which increased by 4-5 times, respectively. In the dynamics of the development of the inflammatory process in the brain, an increase in the production of il-6 and il-8 contributes to a further increase in the permeability of the hematoencephalic barrier, the outflow of neutrophils and, as a result, the development of complications. The direct correlation relationship between detected cytokine levels (il-1β, il-6, il-8), cellular immune system indicators T-lymphocytes (CD3+,CD4+,CD8+) suggests that they play an important role in neural inflammatory developmental pathogenesis in ischemic stroke as a secondary factor, and justifies the feasibility of their study to predict progression and consequences in ischemic stroke. The number of days spent in the intensive care unit depends primarily on the state of the vital systems of the body, and for patients with II, this largely determines the level of cerebral dysfunction. As a result of immunocorrectional therapy, MNT has a decrease in the size of the penumbra zone around ischemia and a decrease in neurodevelopment, which leads to a decrease in brain edema, as a result of which there is an early correction of cerebral dysfunction, which is recorded on the Glasgow scale and MSKT, there is a decrease in the volume of Therefore, the duration of stay in the intensive care unit of the main group of patients was 13.8±3.7 days, and in the comparison group-19.4±3.1 days. In ischemic stroke, when an immunocorrectional treatment method is used using an immunomodulatory drug (Acridopheron), neuronal apaptosis is restricted and intra-cerebral pressure normalization occurs, which leads to a faster recovery of central nervous system functions (Glasgow scale). Reducing the duration of stay in the disability and resuscitation department compared to standard therapy. This makes it possible to draw conclusions about improving the results of treatment against the background of the proposed method of using immunocorrectional therapy, which allows you to influence the pathogenetic joint and the molecular mechanisms of the development of brain tumors and neurodevelopment.An analysis of the MSKT data obtained in patients with ischemic stroke in the study showed that all patients in both groups have cerebral hemispheres and cerebral spinal (column) ischemia in primary Mskt. In addition, the flattening of the owners of the cerebral cortex, the narrowing of the basal cistern were signs of a brain tumor with impaired consciousness. Against the background of immunocorrectional therapy in patients of the main group, MSKT data, for example, the shrinkage of the ischemia zone, the appearance of signs of improvement in cerebral cortex architectonics, basal cisternae and the restoration of normal dimensions of the cerebral ventricles, provided information about the regression of brain tumor. The cellular and humoral immune indicators of these dynamic manifestations, blood cytokines, corresponded to the indicators of positive neurological changes on the Glasgow Scale (Figure 5).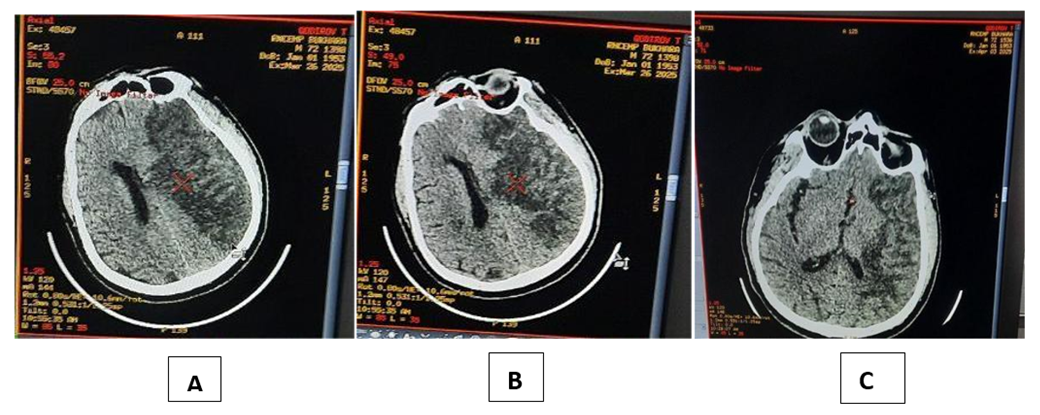 | Figure 5. MSKT examination of a patient with ischemic stroke in the main group (during A - Intake, V - 7-day, after S - 15-day). In patients in the comparison group, however, the above changes in cranial MSKT s showed significantly slower than in the main group |
Thus, the results of the study of changes in systemic (serum) and cellular and humoral immune indicators of the cytokine profile showed that in ischemic stroke, inflammation was acquired and is accompanied by hypersecretion of anti-inflammatory cytokines, the production of which has significant properties in the dynamics of the development of the inflammatory process that occurs in ischemic stroke. The first day after cerebral ischemia (acute period) received serum inflammation (il-1β, il-6, il-8) with a significant increase in cytokine concentration. Such hyperproduction of inflammatory mediators was assessed as an adequate initial reaction of the immune system to injury and was explained by the predominance of the local level cytokine concentration - the characteristics of their secretion at MNS. Received inflammation in cerebral ischemia (il-1β, il-6, il-8) a significant decrease in the concentration of cytokines on the 15th day of the disease in the blood serum reflects the severity of the inflammatory process in the brain, an increase in the permeability of the hematocephalic barrier, which is characteristic of severe forms of II, which can serve as a reliable prognostic criterion for.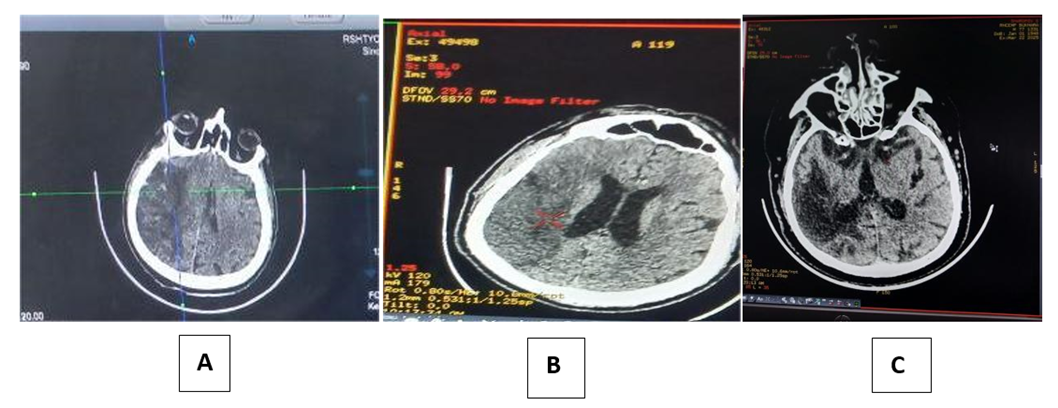 | Figure 6. MSKT examination of a patient with ischemic stroke in the comparison group (A - during admission, V - after day 7, s-after day 15) |
3. Conclusions
It should be noted that the high production of inflammatory cytokines, in particular il-6 and il-8, is important in the pathogenesis of the neurodevelopmental process, since the decrease in geb function as a result leads to the involvement of hematogenous neutrophils in the brain and the development of complications.
References
| [1] | Belozerov E. S. Immunodeficiencies and prenosological forms of immunosuppression / E. S. Belozerov, N. K. Shagshardanov, E. I. Zmushko. - Semipalatinsk, 2008. - P. 141-163. |
| [2] | Boshyan R. E. Infection caused by the Epstein-Barr virus: epidemiological manifestations and laboratory diagnostics: Author's abstract. dis Cand. honey. sciences. - M., 2018. - 42 p. |
| [3] | Burmagina I. A., Pozdeeva M. A., Agafonov V. M. Infectious mononucleosis in the Northern region // Modern medicine: topical issues. - 2014. - No. 33. - P. 26-31. |
| [4] | Valishin D. A., Khunafina D. Kh., Murzabaeva R. T., Mamon A. P. et al. Differential diagnosis in infectious mononucleosis // Bulletin of the Bashkir State Medical University. - 2013. - No. 4. - P. 135-140. |
| [5] | Volokha A.P. Epstein-Barr viral infection in children // Modern Pediatrics. - 2015. - No. 4 (68). - P. 103. |
| [6] | Vygovskaya OV, Kramarev SA, Taradiy NN et al. Immunopathogenesis in Epstein-Barr viral infection in children // Modern Pediatrics. - 2013. - No. 8 (56). - P. 44. |
| [7] | Zhivitsa L.V., Ponomarenko G.F., Predeina V.A.Features of the course of infectious mononucleosis in children and adults // Clinical medicine. - 2018 - No. 10. - P. 121-123. |
| [8] | Galaktionova O. I. Defeat of children with the Epstein-Barr virus in the foci of infectious mononucleosis / O. I. Galaktionova, A. P. Pomogaeva, L. N. Urazova // Mater. I Congress of Pediatric Infectious Diseases of Russia “Act. Questions of infectious pathology in children. - M., 2002. - 32 p. |
| [9] | Gileva R.A., Khokhlova Z.A., Chechet Yu.S. Clinical and laboratory characteristics of infectious mononucleosis caused by the Epstein-Barr virus // Kazan Medical Journal. - 2014. - No. 5. - T. 95. - P. 722-725. |
| [10] | Goreyko T.V., Kalinina N.M., Drygina LB Modern concepts of immunopathogenesis of infection caused by the Epstein-Barr virus // Infection and immunity. - 2017. - No. 2. - T. 1. - P. 121-130. |
| [11] | Narzullaev N.U. Cytokine profile of children with acute inflammation of the palatine tonsil in acute infectious mononucleosis during treatment. Tibbiyotda yangi kun. No. 2 (30). Tashkent 2020, p. 459-461. |
| [12] | Narzullaev N.U., Gaziev K. U. The clinic-epidemiological characteristic of the sharp average otitis at a HIV-infected of children. Central Asian Journal of Medical аnd Natural Sciences. Vol. 3. № 2. 2022. pp. 239-242. |
| [13] | Narzullaev N.U., Xolov X.N., Nurov U.I. Immunopathogenesis оf Clinical Manifestations сhronic Rhinosinusitis. Neuroquantology. Vol. 20. № 6. 2022. pp. 1-8. |
| [14] | Narzullaev N.U., Keldiyorova Z.D., Mirzoeva M.R. Immunological disordersin infectious mononucleosis in children. Neuroquantology. Vol. 20. № 6. 2022. pp. 9600-9602. |
| [15] | Narzullaev N.U., Irismetov M.E., Toshev F.N. Use of thrombocytic autoplasma in treatment of gonarthrosis and coxarthrosis. Journal of Тianjin university science аnd Тechnology. Vol. 65. № 4. 2022. pp. 40-47. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML