-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3742-3746
doi:10.5923/j.ajmms.20251510.99
Received: Sep. 20, 2025; Accepted: Oct. 16, 2025; Published: Oct. 31, 2025

Using Bioimpedance Analysis to Guide Antihypertensive Therapy Adjustment in Patients with High Peripheral Resistance
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOlimjonov Dilshod Dilmurod o’g’li, Alyavi Anis Lutfullayevich
Republican Specialized Scientific Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan
Correspondence to: Olimjonov Dilshod Dilmurod o’g’li, Republican Specialized Scientific Practical Medical Center of Therapy and Medical Rehabilitation, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Effective treatment of hypertension remains a leading global health issue with special concern for patients with excessive peripheral resistance which is a low hanging fruit in health optimization. The use of bioimpedancemetry offers a new way to individualize antihypertensive treatment by optimizing fluid volum and vascular fluid distribution. The objective of this study was to asses the effectiveness of bioimpedancemetry in tailoring antihypertensive therapy in patients with excessive peripheral resistance. In this study, the NICaS bioimpedance cardiograph from NI Medical was employed, a highly accurate, non-invasive device for monitoring hemodynamic parameters. The NICaS device uses a tetrapolar electrode configuration placed on the wrist and opposite ankle of the patient, measuring electrical resistance changes in response to arterial pulsation, allowing for precise assessment of vascular resistance and fluid distribution in the body.
Keywords: Bioimpedancemetry, Hypertension, Peripheral resistance, Antihypertensive therapy, Personalized medicine
Cite this paper: Olimjonov Dilshod Dilmurod o’g’li, Alyavi Anis Lutfullayevich, Using Bioimpedance Analysis to Guide Antihypertensive Therapy Adjustment in Patients with High Peripheral Resistance, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3742-3746. doi: 10.5923/j.ajmms.20251510.99.
Article Outline
1. Introduction
- According to the latest reports from the World Health Organization, hypertension is a significant issue in the world with over 1.28 billion people suffering from it, causing significant morbidity and mortality. Hypertension not only increases the chances of acquiring cardiovascular diseases, such as strokes, heart attacks, and heart failures, which all ultimately contribute to the worldwide burden on the economy and the healthcare system. Therapeutically hypertension is a very divided and complex issue. Patients with high peripheral resistance with comorbid high blood pressure pose a unique challenge because of the systemic and vascular factors like endothelial insufficiency and increased vascular rigidity [3]. In spite of the progress made in the field of medicine and the introduction of several antihypertensive medications, it continues to remain one of the most difficult condition to treat in the healthcare field. Patients suffering from hypertension with peripheral vascular resistance, the standard treatment offers does not take fluid retention and vascular resistance which are the key factors in treatment response. There is a highly robust demand in the market in for efficient diagnostic treatments that are able to identify the major contributors to tailored treatment [4]. Bioimpedancemetry has emerged as a promising technology in this context.
2. The Purpose of the Study
- This method measures electrical impedance using certain body tissues to achieve insights about vascular resistance, fluid balance, and body composition. This information is critical to patients having high peripheral resistance, for it enables clinicians to customize antihypertensive strategies to specific physiological configurations. Primary research indicates that treatment approaches based on bioimpedance measurement can lead to controlled blood pressure levels, thus minimizing cardiovascular risk.This paper seeks to assess the impact of bioimpedancemetry on antihypertensive treatment optimization in patients with excessive peripheral resistance. With the intent of improving therapeutic results, the investigator seeks to integrate bioimpedancemetry into routine clinical practice in a manner that nuance the treatment approach to balance blood pressure and minimize cardiovascular risk.
3. Materials and Methods
- This research was planned as a prospective observational study for a duration of 6 months. The ethics committee of the designated medical center, in keeping with the declaration of Helsinki, granted ethical approval for the study. Participants were enrolled only after completing the informed consent form. 62 patients with hypertension, aged between 29 and 60 years (mean age 48.75 ± 1.6 years), of whom 30 were female, were included. The following inclusion criteria were used: a diagnosis of essential hypertension and signs of increased peripheral resistance on clinical examination and bioimpedance measurements. Exclusion criteria were secondary hypertension, pregnancy, severe renal or hepatic dysfunction, and history of cardiovascular events within the past six months. Bioimpedance measurements were conducted using the NICaS bioimpedance cardiograph. This device uses a 1.4 mA alternating current at a frequency of 32 kHz, which is capable of measuring body electrical resistance changes. These changes are related to vascular pulsations, allowing for the assessment of total body water (TBW), extracellular water (ECW), intracellular water (ICW), and total peripheral resistance (TPR). These metrics are crucial in understanding fluid balance and vascular health in hypertensive patients, providing a foundation for personalized treatment adjustments.Antihypertensive therapy was provided in line with current clinical practice recommendations, including angiotensin-converting enzyme inhibitors, calcium channel blockers, diuretics, and beta-blockers. Therapeutic approaches were tailored based on bioimpedancemetry results, with the goal of lowering blood pressure to the greatest extent possible and avoiding adverse effects. Bioimpedance measurement was done using a standardized protocol at baseline, three months, and six months. Vascular resistance, total body water, extracellular water, and intracellular water were some of the primary parameters assessed. The readings were done under standard conditions using fasting patients and a minimum of 30 minutes post-exercise to ensure uniformity. The measurements were taken at baseline, three months, and six months. Blood pressure systolic and diastolic, vascular resistance as assessed by bioimpedance, the level of hydration, and clinical end points were recorded. Patient compliance and side effects were also recorded. Statistical analysis was performed using SPSS software version 27.0. Continuous data were expressed as mean ± standard deviation, whereas categorical data were expressed as frequencies and percentages. Changes in parameters pairwise over time were analyzed using paired t-tests or repeated-measures NICaS. Multivariate regression models were employed to identify the correlation between bioimpedance parameters and clinical outcomes. A p-value of <0.05 was considered statistically significant.
4. Results
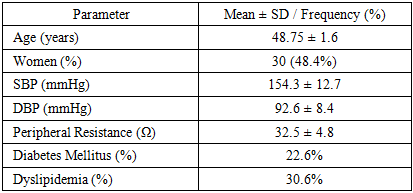
- A total of 62 patients composed the study population with a mean age of 48.75 ± 1.6 years. Thirty were females (48.4%). Baseline SBP was 154.3 ± 12.7 mmHg and DBP was 92.6 ± 8.4 mmHg. Vascular resistance values gathered via bioimpedancemetry had an average of 32.5 ± 4.8 ohms. The group also comprised patients with comorbid illnesses such as diabetes mellitus (22.6%) and dyslipidemia (30.6%) (Table 1). Over the course of the study, measurements of TBW, ECW, ICW, and TPR at baseline, 3 months, and 6 months showed significant changes that were critical for adjusting antihypertensive therapy. These data indicated improvements in fluid balance and a reduction in vascular resistance, both of which were associated with enhanced blood pressure control.
|
|

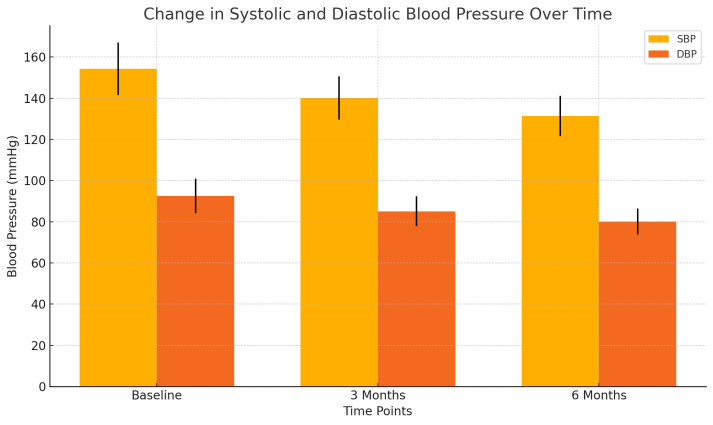 | Figure 1. Change in Systolic and Diastolic Blood Pressure Over Time |
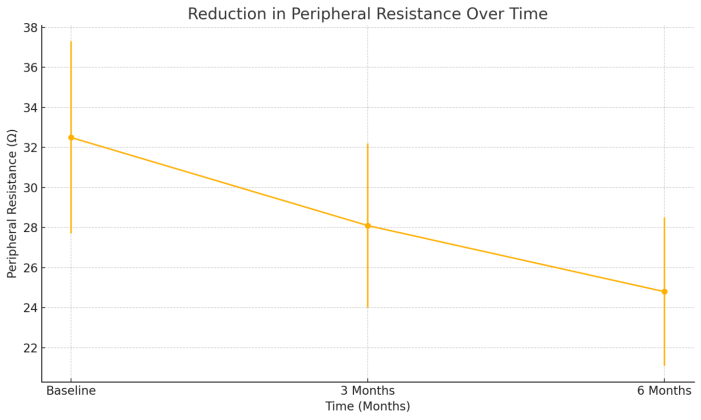 | Figure 2. Reduction in Peripheral Resistance Over Time |
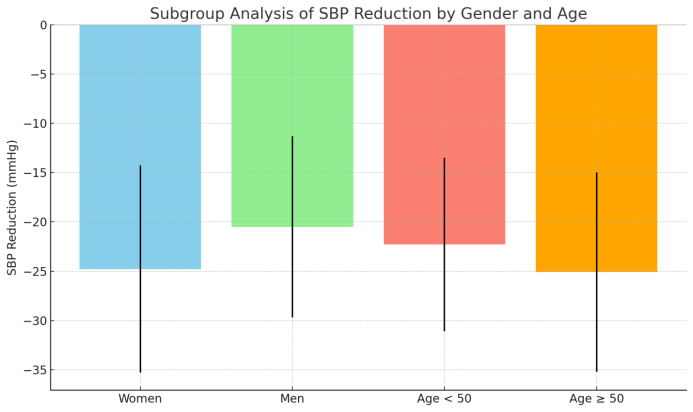 | Figure 3. Subgroup Analysis of SBP Reduction by Gender and Age |
5. Discussion
- This study illustrates how using bioimpedancemetry therapy can aid in controlling blood pressure and in reduction of peripheral resistance in hypertensive patients with a tendency of peripheral resistance. The results were prominent in peripheral resistance and blood pressure, both diastolic and systolic, after a 6 month period. Bio determacemetry can personalize hypertensive therapy and provide clinical resistance arguments proven effective. While this study confirms the usefulness of bioimpedance in personalizing hypertensive treatment, further research is necessary to establish broader clinical applications. Future studies should explore the integration of bioimpedance measurement with other advanced diagnostic tools, such as wearable sensors and artificial intelligence, to provide more comprehensive insights into cardiovascular health. Additionally, expanding the use of bioimpedance analysis across diverse patient populations and clinical settings will help confirm its long-term benefits and establish its place in routine clinical practice.Recent studies on bioimpedancemetry in hypertension therapy provide a clear diagnosis of the condition. For example, Taylor et al describe the parameters more accurately, stating that they are able to predict the responsive therapy bioimpedance used in resistant patients. [4] However, the comprehensive bioimpedance proven extensive clinical value over the 6 month period, particularly in patients with significant peripheral resistance. Different from the previous studies, this one offers subgroup studies providing therapeutic differences in the age and gender.Utilizing bioimpedancemetry within unheard limits concerning the management of hypertension brings in value additions on several fronts. A clinically driven individualized approach to overcoming hypertension which balances therapy against vascular resistance and fluid status is better position to achieve optimal blood pressure and lower the risk of cardiovascular events. Uniointed bcheck-directed therapy enhances compliance by limiting side effects and promoting individualized therapy. In addition, bioimpedance measurements are non-invasive, inexpensive, and can be integrated into workflow measurements which undoubtedly increases their utility as standards of practice. The strengths of this study include its prospective design bioimpedance metrics and robust statistical evaluation. On the other hand, concerns over generalizability rest on the small single center sample size. Also, findings do not establish causality of therapy outcomes concerning the associations made with bioimpedance parameters. These findings, and particularly the long-term outcomes, require confirmation by future studies that are multicenter and include larger cohorts.Future research should focus on expanding the use of bioimpedancemetry in diverse patient populations and settings. Investigating its role in predicting cardiovascular events and exploring its integration with other advanced diagnostic tools, such as wearable sensors and artificial intelligence, could further enhance its clinical utility. Long-term studies are also necessary to assess the sustainability of the observed benefits and their impact on morbidity and mortality. By advancing the understanding of bioimpedancemetry’s role in hypertension management, this study provides a foundation for its broader application in personalized medicine.
6. Conclusions
- This study underscores the pivotal role of bioimpedancemetry in optimizing antihypertensive therapy for patients with high peripheral resistance. By enabling precise measurement of vascular resistance and fluid balance, bioimpedancemetry-guided therapy significantly improved blood pressure control, reduced peripheral resistance, and enhanced clinical outcomes over a six-month period.Incorporating advanced diagnostic tools like bioimpedancemetry into routine clinical practice holds great promise for the personalized management of hypertension. This approach not only addresses the individual variability in physiological responses but also enhances the overall efficacy and safety of antihypertensive therapies. Future research should aim to further validate and expand the application of bioimpedancemetry in diverse patient populations, ultimately contributing to better cardiovascular health outcomes.Conflict of Interest Statement. None.