-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3718-3720
doi:10.5923/j.ajmms.20251510.94
Received: Sep. 27, 2025; Accepted: Oct. 21, 2025; Published: Oct. 31, 2025

Load Tolerance and Quality of Life in Patients with Chronic Heart Failure and Obesity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLN. F. Tashkenbayeva
Republican Scientific and Practical Center of Cardiology, Tashkent, Uzbekistan
Correspondence to: N. F. Tashkenbayeva, Republican Scientific and Practical Center of Cardiology, Tashkent, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective. To assess exercise tolerance and quality of life in patients with chronic heart failure (CHF) and obesity depending on the presence of metabolic syndrome (MS). Materials and methods. The study included patients with obesity and CHF (main group) and obese individuals without CHF (control group), stratified by the presence/absence of MS. Treadmill test parameters were evaluated (duration, maximal workload, VO₂, chronotropic index, heart rate increase, peak systolic blood pressure [SBP] and its increment), along with quality of life using the Minnesota Living with Heart Failure Questionnaire (MLHFQ) and the SF-36 survey. Results. Patients with MS demonstrated significantly lower exercise tolerance: reduced treadmill duration, VO₂, chronotropic index, and heart rate increase, accompanied by a greater increment of SBP. According to MLHFQ, patients with MS reported worse physical and emotional functioning and a higher total score (indicating poorer quality of life). On SF-36, MS was associated with reduced physical functioning and general health. Conclusion. The presence of MS in patients with CHF and obesity is associated with reduced exercise tolerance and impaired quality of life, underscoring the need for comprehensive cardiometabolic rehabilitation aimed at correcting metabolic disturbances and improving functional reserve.
Keywords: Chronic heart failure, Obesity, Metabolic syndrome, Exercise tolerance, Quality of life, SF-36, MLHFQ
Cite this paper: N. F. Tashkenbayeva, Load Tolerance and Quality of Life in Patients with Chronic Heart Failure and Obesity, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3718-3720. doi: 10.5923/j.ajmms.20251510.94.
1. Introduction
- Chronic heart failure (CHF) is one of the leading causes of disability and reduced quality of life in the population. In recent years, researchers have been focusing on the combination of CHF with obesity and metabolic syndrome (MS). This phenotype is characterized not only by hemodynamic and metabolic disorders but also by decreased exercise tolerance, which directly affects the prognosis and daily activity level of patients [1,3].Limited exercise tolerance in such patients is associated with the activation of neurohumoral systems, endothelial dysfunction, insulin resistance, inflammation, and myocardial remodeling. Additionally, the presence of MS contributes to a further decrease in functional reserve, deterioration of quality of life, and an increased risk of repeated hospitalizations [2,5].Important tools for assessing patients' condition include exercise tests (treadmill, VO2), the Minnesota Living with Heart Failure Questionnaire (MLHFQ) scale, and the SF-36 questionnaire, which allow for a quantitative assessment of the disease's impact on physical activity and overall well-being [4,6].Research Objective — to assess indicators of exercise tolerance and quality of life in patients with chronic heart failure and obesity, depending on the presence of metabolic syndrome.
2. Material and Methods
- A cross-sectional comparative study was conducted, including patients with obesity and chronic heart failure (CHF) (main group) and individuals with obesity without CHF (control group), divided based on the presence/absence of metabolic syndrome (MS).• The observation groups included:• MG (main group) without MS - patients with CHF and obesity, without signs of metabolic syndrome.• MG with MS - patients with CHF and obesity in the presence of metabolic syndrome.• CG (comparison group) without MS - control group (obesity without CHF and without MS).• CG with MS - control group (obesity without CHF, with MS).Exercise stress tests (treadmill): duration, maximum achieved workload, oxygen consumption (VO2), heart rate (HR % of predicted), chronotropic index (CI), HR increase, peak systolic blood pressure, systolic blood pressure increase.Quality of Life Questionnaires:- Minnesota Living with Heart Failure Questionnaire (MLHFQ): assessment of physical activity limitation (PAL), emotional distress (ED), and total score (TS).- SF-36: physical functioning (PF), role-physical (RP), vitality (VT), emotional well-being (EW), general health (GH).Statistical analysis: data are presented as M±SD, Student's t-test was used for comparison. Differences were considered statistically significant at p<0.05.
3. Results
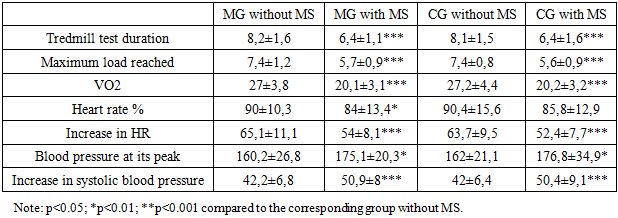
- Analysis of the treadmill test results showed a significant decrease in functional reserve in patients with chronic heart failure and obesity in the presence of metabolic syndrome (Table 1).
|
4. Discussion
- This study demonstrated that the presence of metabolic syndrome (MS) in patients with chronic heart failure (CHF) and obesity is associated with a pronounced decrease in exercise tolerance and deterioration in quality of life.A significant reduction in treadmill test duration, VO2, and maximum achieved workload in patients with MS reflects a decrease in aerobic capacity and functional reserve. A less pronounced increase in heart rate and a decrease in the chronotropic index (CI) in this cohort indicate chronotropic incompetence - a typical manifestation of neurohumoral dysregulation and autonomic dysfunction in the combination of CHF, obesity, and insulin resistance. Clinically, this leads to premature fatigue, reduced tolerance for daily activities, and limited participation in rehabilitation programs.In patients with MS, against a background of lower heart rate increase, higher systolic blood pressure (SBP) was observed at peak exercise and greater SBP increase. Such dissociation (enhanced pressor response with relative chronotropic "rigidity") aligns with the understanding of the role of sympatho-adrenal hyperactivation, vascular stiffness, and endothelial dysfunction in forming an abnormal response to exertion. In practice, this is associated with a higher risk of events and a worse prognosis in CHF.According to MLHFQ, MS patients have higher scores for physical functional limitations and emotional distress, as well as higher overall scores (worse quality of life). According to SF-36, a decrease in physical functioning (PF) and general health (GH) was revealed, and in several comparisons, a decrease in vitality (VT). These data highlight that MS negatively impacts not only physiological but also subjective aspects of health, exacerbating the "symptom burden" of CHF.Thus, patients with CHF+obesity+MS are indicated for structured cardiometabolic rehabilitation programs: gradual aerobic training with heart rate/blood pressure monitoring, addition of low-to-moderate intensity interval protocols, breathing exercises; correction of body weight and visceral component is mandatory.Considering the enhanced pressor response and low chronotropic response, optimization of beta-blockers (taking into account chronotropic competence), ACE inhibitors/ARBs/ARNI, possible prescription of SGLT-2 inhibitors (as cardiorenometabolic therapy), and statin therapy for atherogenic profile is justified.Diet therapy (calorie content, protein, restriction of simple sugars and salt), gradual physical activity, behavioral interventions; if necessary, pharmacotherapy for obesity according to indications.Targeting of autonomic dysfunction. Heart rate control, heart rate variability training, and stress management can improve chronotropic reserve and exercise tolerance.Strengths: simultaneous assessment of objective exercise parameters (treadmill, VO2, CI) and validated quality of life questionnaires (MLHFQ, SF-36) with clear stratification according to MS.
5. Conclusions
- The presence of metabolic syndrome in patients with chronic heart failure and obesity is associated with a significant decrease in exercise tolerance (shorter duration of treadmill test, lower VO2, lower maximum workload); chronotropic incompetence (smaller increase in heart rate, lower chronotropic index); enhanced pressor response to exercise (higher systolic blood pressure at peak and greater systolic blood pressure increase); deterioration of quality of life according to MLHFQ and decreases in SF-36 domains (especially physical functioning and general health perceptions).The obtained data substantiate the need for a comprehensive cardiometabolic approach: combining evidence-based pharmacotherapy for chronic heart failure and metabolic syndrome with personalized rehabilitation, body weight control, and correction of autonomic dysfunction, which should improve exercise tolerance and quality of life indicators.