-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3702-3705
doi:10.5923/j.ajmms.20251510.90
Received: Sep. 26, 2025; Accepted: Oct. 22, 2025; Published: Oct. 31, 2025

Comparative Analysis of Pregnancy Course, Delivery Outcomes and Neonatal Condition in Women from Namangan and Tashkent Depending on Vitamin D Status
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFeruza Rаhmatjonovna Turdieva1, Dilrabo Talmasovna Kayumova2
1Phd Student, Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health, Uzbekistan
2D.M.Sc. Professor, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Feruza Rаhmatjonovna Turdieva, Phd Student, Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Over the past decade, numerous studies have accumulated in the literature linking vitamin D deficiency and insufficiency during pregnancy with a wide range of adverse outcomes for maternal, fetal, and neonatal health. The aim of this study was to evaluate the impact of vitamin D status on the course of pregnancy, delivery outcomes, and perinatal indicators among women in Namangan region and Tashkent city. Materials and Methods. Patients were divided into three groups: with deficiency, insufficiency, and adequate vitamin D levels. Results. Comparative analysis revealed no statistically significant differences between the regions in terms of delivery outcomes, anthropometric data, and Apgar scores (p>0.05). Conclusion. Adequate vitamin D levels in pregnant women contribute to a reduced risk of complications and improved perinatal outcomes, regardless of the region of residence.
Keywords: Vitamin D, Pregnancy, Complications, Newborn, Apgar scale
Cite this paper: Feruza Rаhmatjonovna Turdieva, Dilrabo Talmasovna Kayumova, Comparative Analysis of Pregnancy Course, Delivery Outcomes and Neonatal Condition in Women from Namangan and Tashkent Depending on Vitamin D Status, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3702-3705. doi: 10.5923/j.ajmms.20251510.90.
1. Introduction
- In recent years, the role of vitamin D in ensuring a normal course of pregnancy and fetal development has attracted increasing attention from researchers. According to modern data, more than 40–80% of women of reproductive age have insufficient serum 25(OH)D levels, which makes hypovitaminosis one of the most pressing problems in obstetrics [1,6]. Vitamin D insufficiency during pregnancy is associated with a higher incidence of complications such as preeclampsia, gestational diabetes, preterm birth, anemia, and infectious diseases [2,5]. For newborns, maternal vitamin D deficiency often leads to low birth weight, intrauterine growth restriction, increased risk of infections, and low Apgar scores [5].One of the important factors influencing vitamin D sufficiency is the geographical location and place of residence. Studies show that vitamin D levels are directly related to latitude and solar radiation intensity: deficiency occurs significantly more often in northern than in southern regions [9]. In addition, ethnic and cultural factors, including dietary habits and clothing that limits ultraviolet exposure, also play a role [8]. Some studies have demonstrated differences between residents of urban and rural areas. Women in rural areas usually have higher vitamin D levels, which is associated with longer sun exposure and greater outdoor physical activity. In contrast, urban women more often present with deficiency due to a sedentary lifestyle, prolonged stay indoors, and sunscreen use [3,4]. Even under identical climatic conditions, vitamin D sufficiency can vary significantly within a single country. For example, Wang et al. (2016) demonstrated that serum 25(OH)D levels and bone mineral density depended not only on the season but also on the specific region of residence [7]. These findings emphasize the necessity of considering geographical factors when assessing vitamin D status.For Uzbekistan, this problem is of particular importance. Despite high levels of insolation, vitamin D deficiency and insufficiency remain widespread among pregnant women. This is associated with cultural characteristics (wearing closed clothing), limited sun exposure, as well as dietary patterns.Aim of the study. To assess the features of pregnancy course, delivery outcomes, and perinatal indicators in pregnant women from Namangan region and Tashkent city depending on vitamin D status.
2. Materials and Methods
- A total of 166 pregnant women and their newborns were examined from January 2024 to September 2025. Among them, 100 were observed at the Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health (Tashkent), and 66 at the Namangan branch of the same institution.All pregnant women underwent a general clinical examination, which included complaints collection, medical history, general and special obstetric examination. Serum 25-hydroxycholecalciferol (25-OH-D) levels were determined in maternal venous blood using immunochemiluminescent assay (ELISA).For the classification of vitamin D status in newborns, the reference ranges of the Russian Association of Endocrinologists were applied:• Deficiency: <20 ng/mL• Insufficiency: ≥20 and <30 ng/mL• Optimal/adequate: ≥30 ng/mLStatistical analysis was performed as absolute values and their percentage ratios using applied software packages.
3. Results and Discussion
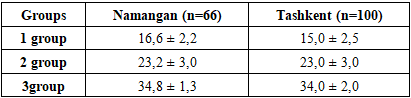
- Out of 100 patients included in the study in Tashkent, Group 1 (n=41; 41%) consisted of pregnant women with vitamin D deficiency, Group 2 (n=29; 29%) – with vitamin D insufficiency, and Group 3 (n=30; 30%) – with optimal vitamin D levels (control group). Thus, vitamin D deficiency among pregnant women in Tashkent occurred 1.4 times more frequently compared to insufficiency and normal levels.In Namangan, 66 pregnant women were examined. Among them, vitamin D deficiency was identified in 36.4% (n=24), insufficiency – in 45.5% (n=30), and optimal levels – only in 18.1% (n=12). Unlike Tashkent, vitamin D insufficiency predominated in Namangan, while the proportion of women with adequate vitamin D status was almost twice as low (18.1% vs. 30%).
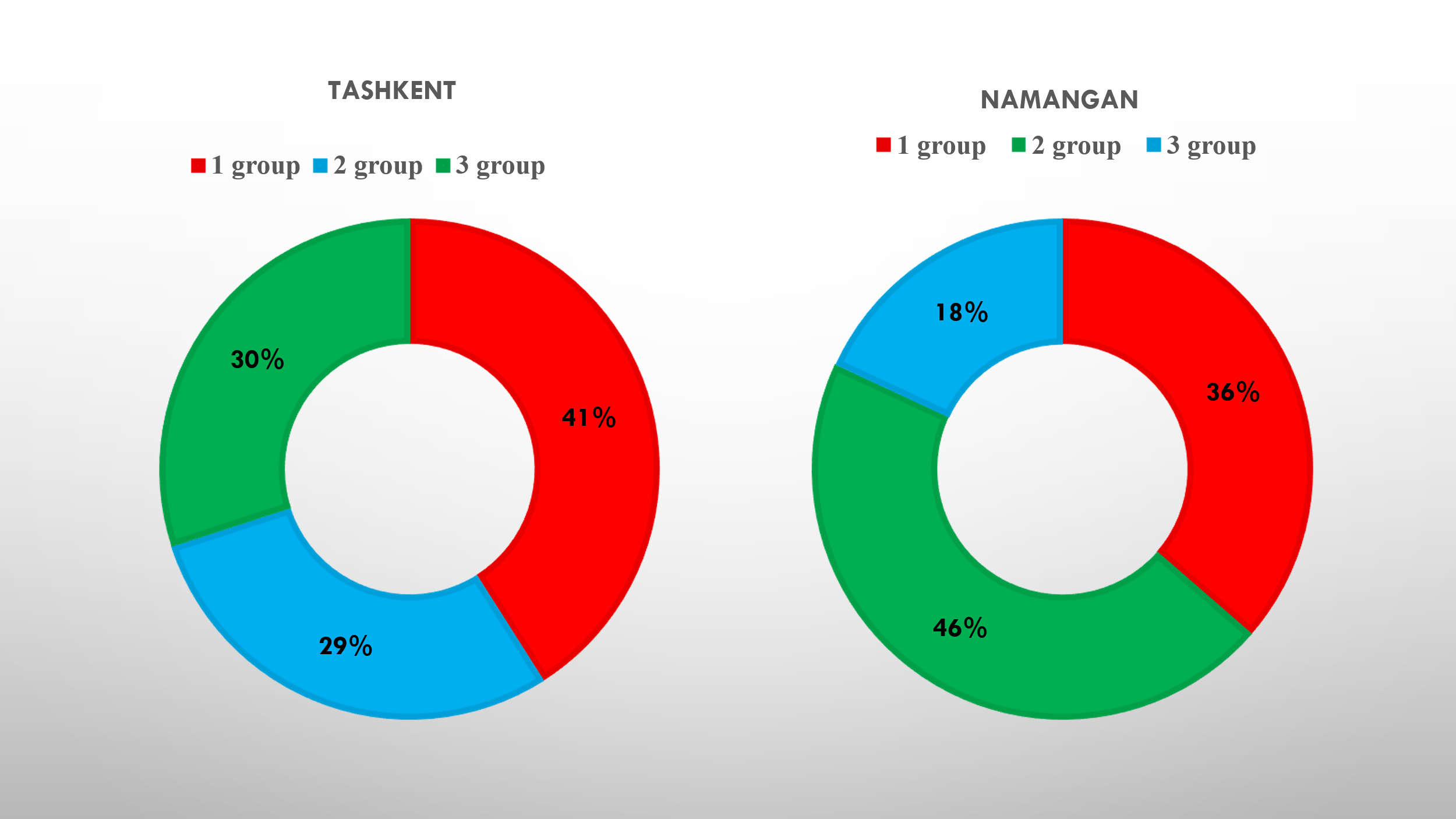 | Figure 1. Structure of pregnant women, (%) |
|
|
|
|

|

4. Conclusions
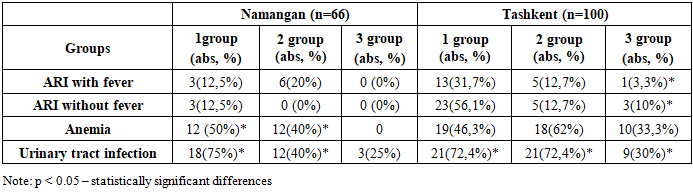
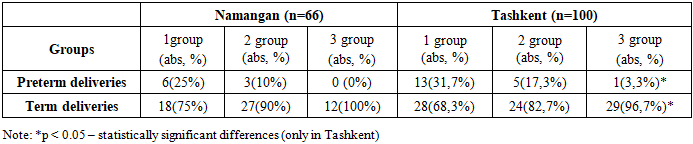
- The present study revealed that vitamin D deficiency and insufficiency are widespread both in Namangan region and in Tashkent city, with differences in distribution: vitamin D deficiency was more frequently observed in Tashkent, whereas insufficiency predominated in Namangan. Pregnant women with vitamin D deficiency more often experienced pregnancy complications such as urinary tract infections, anemia, and respiratory infections. In Namangan, the association with urinary tract infections and anemia was more pronounced, while in Tashkent deficiency was accompanied by a higher frequency of respiratory diseases. Comparative analysis of the course of labor showed no statistically significant differences between the regions in the rates of preterm and term deliveries. Birth weight and length, as well as Apgar scores, were higher in newborns of mothers with adequate vitamin D levels; however, interregional differences were not statistically significant (p > 0.05).Thus, the findings confirm the importance of maintaining optimal vitamin D sufficiency during pregnancy for favorable gestational course and neonatal outcomes. Regardless of the region of residence, adequate maternal vitamin D levels are associated with improved newborn health indicators.