-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3698-3701
doi:10.5923/j.ajmms.20251510.89
Received: Sep. 29, 2025; Accepted: Oct. 25, 2025; Published: Oct. 31, 2025

The Significance of Hemodynamic Markers for the Early Detection of Preeclampsia in Pregnant Women with Chronic Arterial Hypertension
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNajmetdinova D. F.1, Negmatullaeva M. N.2
1Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health, Uzbekistan
2Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic arterial hypertension (CAH) is a significant risk factor for obstetric complications, including the development of preeclampsia, which markedly increases maternal and perinatal morbidity and mortality rates. Hemodynamic markers play a crucial role in the early diagnosis of this condition, allowing for the assessment of intracardiac and central hemodynamics, detection of left ventricular diastolic dysfunction, and evaluation of volumetric disturbances. The analysis of these parameters contributes to the timely prediction of complications and facilitates the development of individualized management strategies for high-risk pregnant women.
Keywords: Chronic arterial hypertension, Preeclampsia, Pregnancy, Hemodynamic markers, Early diagnosis, Cardiovascular complications, Maternal mortality, Perinatal outcomes
Cite this paper: Najmetdinova D. F., Negmatullaeva M. N., The Significance of Hemodynamic Markers for the Early Detection of Preeclampsia in Pregnant Women with Chronic Arterial Hypertension, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3698-3701. doi: 10.5923/j.ajmms.20251510.89.
1. Introduction
- Arterial hypertension (AH) is among the most prevalent diseases both in the general population and among women of reproductive age. The steady increase in its prevalence and associated cardiovascular complications necessitates the search for new approaches to diagnosis and treatment. In recent years, researchers have shown increasing interest in predicting and diagnosing the early stages of hypertensive syndromes, owing to their significant impact on maternal and perinatal mortality [1,3].Chronic arterial hypertension (CAH) remains one of the leading causes of severe cardiovascular complications and mortality worldwide, including among women of reproductive age. According to the World Health Organization (WHO), CAH causes approximately 10 million deaths annually, with an additional 6.3 million individuals becoming disabled. The overall number of patients exceeds 1 billion globally. The relevance of this issue to obstetrics lies in the fact that CAH is an important predictor of future cardiovascular pathology and ranks second among the causes of maternal mortality [4,8].Hypertensive disorders complicate up to 10% of pregnancies, of which approximately one-third are associated with CAH, while the remaining cases are linked to gestational hypertension. The presence of CAH significantly increases the risk of superimposed preeclampsia, which worsens the course of pregnancy in 25–70% of cases, increasing the frequency of obstetric and perinatal complications. Pregnancy against the background of arterial hypertension is accompanied by profound changes in the cardiovascular system. When preeclampsia develops on top of CAH, it exacerbates left ventricular diastolic dysfunction, disrupts intracardiac and central hemodynamics, contributes to the development of asymptomatic heart failure, and negatively affects fetal intrauterine growth. In this regard, the assessment of hemodynamic markers that reflect cardiac output, minute performance, and volumetric changes in the maternal body is of particular importance [2,6].At present, the relationship between hemodynamic disturbances and endothelial dysfunction, as well as their role in the pathogenesis of preeclampsia in women with CAH, remains insufficiently clarified. The study of these markers allows for the prediction of maternal and fetal risks and supports the development of individualized approaches to the management of high-risk pregnancies [5,7].Aim of the Study: To determine the role of hemodynamic markers in the early diagnosis of preeclampsia developing against the background of chronic arterial hypertension.
2. Materials and Methods
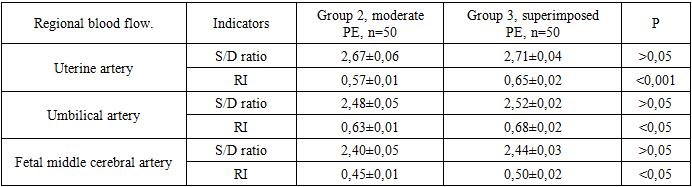
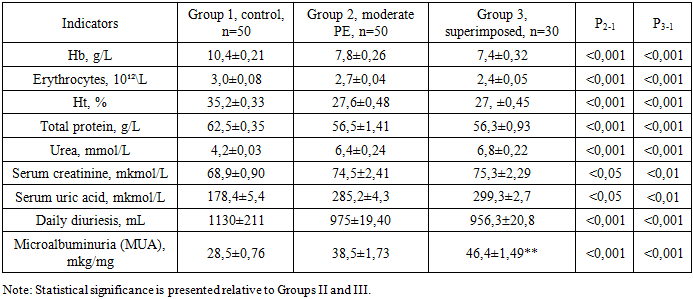
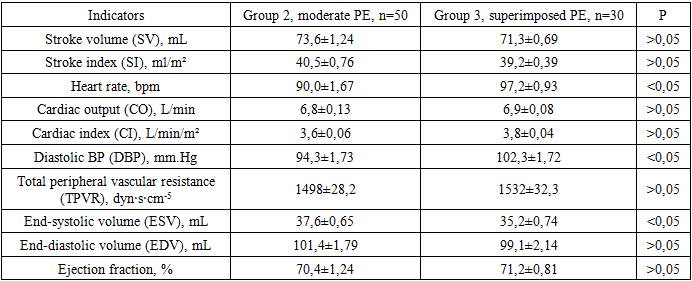
- A screening examination was conducted on 150 pregnant women, divided into three groups:• Group I — pregnant women with chronic arterial hypertension complicated by preeclampsia (n = 50);• Group II — pregnant women with a physiological course of pregnancy who subsequently developed preeclampsia (n = 50);• Group III — pregnant women with an uncomplicated physiological pregnancy (n = 50).The following parameters were evaluated in all patients:• indicators of systemic hemodynamics (blood pressure, systolic arterial pressure, total peripheral vascular resistance);• central and regional hemodynamics (renal and uteroplacental-fetal blood flow) assessed by Doppler ultrasound;• clinical and biochemical parameters (urea, creatinine, total protein, etc.);• blood coagulation indicators (platelets, prothrombin index, activated partial thromboplastin time, clotting time, INR, fibrinogen);• Doppler measurements of uteroplacental and renal blood flow.Statistical analysis of the data was performed using Student’s t-test. Normality of distribution was assessed using the kurtosis test, while equality of variances was checked using Fisher’s F-test. Differences were considered statistically significant at p < 0.05.
3. Results
- Status of homeostatic parameters in women with superimposed preeclampsia. This group included 50 pregnant women with chronic arterial hypertension and proteinuria, in whom superimposed preeclampsia was diagnosed at 20–22 weeks of gestation. The mean age of patients was 36.1 ± 2.4 years. By parity: primiparous — 16 (32%), multiparous — 34 (68%). The diagnosis of superimposed preeclampsia was established when the following criteria were met:• newly detected proteinuria (≥ 0.3 g/day) after 20 weeks of pregnancy, or worsening of pre-existing proteinuria;• progression of arterial hypertension in women whose blood pressure was well controlled before 20 weeks of pregnancy;• onset of multi-organ dysfunction symptoms after 20 weeks of gestation.As control groups, 50 pregnant women with moderate preeclampsia and 50 women with physiological pregnancies were selected. All patients, upon manifestation of clinical signs of preeclampsia, were hospitalized in a specialized maternity facility, where dynamic monitoring of maternal and fetal status was conducted starting from the second trimester.
|
|
|