-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3658-3661
doi:10.5923/j.ajmms.20251510.80
Received: Oct. 8, 2025; Accepted: Oct. 27, 2025; Published: Oct. 31, 2025

Management Tactics for Young Children with CHD and Analysis of Its Effectiveness Before and After Cardiac Surgery
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdurakhmanova Dilnoza Furkatovna1, Akramova Khursanoy Abdumalikovna2
1Department of Hospital Pediatrics No. 1, Traditional Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
2DSc., Department of Hospital Pediatrics No. 1, Traditional Medicine, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Akramova Khursanoy Abdumalikovna, DSc., Department of Hospital Pediatrics No. 1, Traditional Medicine, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Congenital heart defects (CHD) in young children are frequently associated with comorbidities and nutritional deficiencies that negatively influence postoperative recovery. This study aimed to optimize preoperative management and nutritional correction methods for children with CHD to improve surgical outcomes. A prospective analysis was conducted on 144 children aged 3 months to 3 years, divided into two groups: the main group (102 patients) receiving optimized preoperative management and the comparison group (42 patients) treated according to standard protocols. The optimized approach included individualized nutritional support emphasizing breast milk preservation, use of therapeutic protein hydrolysate mixtures, and vitamin supplementation. Results demonstrated a significant improvement in body weight and body mass index (BMI) in the main group compared to the control, with a reduction in malnutrition rates from 19.6% to 11.8% (p<0.05). Postoperative complications, such as dyspnea, cyanosis, and feeding difficulties, decreased more markedly in the main group (p<0.01). Weight recovery to preoperative levels occurred within 3–4 weeks in the main group versus 6–8 weeks in the comparison group. In conclusion, optimized preoperative management with targeted nutritional support significantly enhances physical development, accelerates postoperative recovery, and reduces complications in young children undergoing cardiac surgery for CHD.
Keywords: Congenital heart defects, Children, Nutritional status, Preoperative management, Cardiac surgery, Postoperative recovery, Body mass index
Cite this paper: Abdurakhmanova Dilnoza Furkatovna, Akramova Khursanoy Abdumalikovna, Management Tactics for Young Children with CHD and Analysis of Its Effectiveness Before and After Cardiac Surgery, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3658-3661. doi: 10.5923/j.ajmms.20251510.80.
1. Introduction
- According to the World Health Organization (WHO), " ... 303,000 children die annually from malformations during the first 4 weeks of life. Malformations can lead to long-term disability, which has a significant impact on individuals, their families, health systems, and society... " [1] Comorbid pathology and impaired physical development are considered operational risk factors and are identified in 30% of children with congenital heart defects [2], which are significant risk factors in relation to The presence of comorbid pathology has a significant impact on the course of the postoperative period, the development of complications, and also affects the prognosis. Current standards and approaches in cardiac surgery should include analysis of comorbid diseases when choosing methods of anesthesia, intensive care, and surgical intervention tactics [3,4]. Comorbidity is the presence of another disease or medical condition simultaneously with the present disease. It is known that the presence of comorbid diseases contributes to an increase in hospital bed days, leads to the development of disability, hinders rehabilitation, and increases the number of complications after surgical interventions [5].The purpose of the study. To optimize the method of preoperative management of young children with congenital heart defects based on the assessment of the state of physical development, and to develop methods of nutrition correction.
2. Materials and Methods
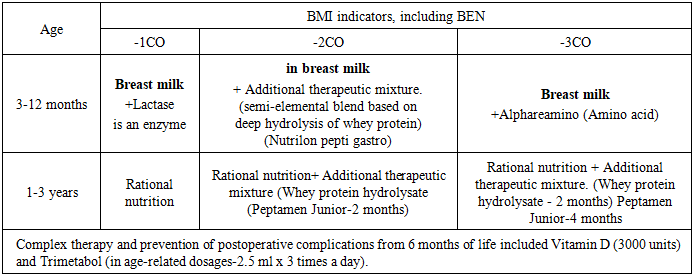
- The paper presents an analysis of a prospective study of 144 children with congenital heart defects (CHD). The age of the examined children with CHD ranged from 3 months to 3 years. The children were divided into 2 groups: the main group-102 children with optimized preoperative management and 44 children – the comparison group with standard preoperative management. We evaluated the effectiveness of preoperative preparation at the hospital stage and during the follow-up period in terms of anthropometric results and somatic status.Management of children with congenital heart defects was aimed at stabilizing the patient's condition, correcting hemodynamic disorders, preventing complications, and preparing for the upcoming surgical intervention. The main tasks included: maintenance of adequate gas exchange and tissue perfusion; correction of hypoxemia and metabolic acidosis; optimization of heart and lung function; prevention of infectious complications; provision of nutritional support and normal water-electrolyte balance.In the main group (102 patients), medical nutrition for patients of the first year of life with malnutrition was carried out with the maximum possible preservation of breast milk in the diet (table. 1).
|
3. Result and Discussion
- When analyzing the physical development of young children with CHD in the dynamics of follow-up, in the preoperative and postoperative periods, the following results were obtained.The dynamics of body weight in 44.1% of children with CHD in the main group after 3 months corresponded to the median, which is 14.7% higher than the baseline values. Thus, initially high body mass indices corresponding to +2CO - +1CO and +3CO - +2CO were found in 4.9% and 2.0%, respectively, in children in the main group; after 3 months, a decrease in the frequency of occurrence of high body mass indices was found by almost 3.5 times, so 2.0% of children with CHD in the main group recorded a decrease in the frequency of occurrence of body weight corresponding to +2CO-+1CO.Taking into account the fact that children with CHD in most cases registered low body weight at the initial examination, in 9.8% and 19.6%, respectively-2CO - - 3CO and-1CO - - 2CO, then after 3 months of follow-up, these percentages significantly decreased to 2.9% and 11.8%, respectively (P < 0.05).In the comparison group, the body weight of children remained almost at the same level as at the initial examination, and a tendency was established to reduce the frequency of occurrence of body weight corresponding to the median from 31.0% to 26.2%, respectively. There is alsoan increase in the observedincrease повышения массы in body weight reaching 4.8%.There is a tendency to increase the frequency of occurrence of children in the comparison group with low body weight, which in 23.8% after 3 months corresponded to-1CO - - 2CO, which is 4.8% higher. In 14.3% of children with CHD from the comparison group, after 3 months of follow-up, low body weight corresponding to - 2CO--3 CO was recorded, which is 3.6% higher than the initial data.When measuring body weight at admission to the hospital for surgical treatment, the body weight of children in the main group in 47.1% corresponded to the median, while in the comparison group this percentage was 26.2%, which is 20.9% higher (P < 0.05). Also, children in the main group were significantly less likely to have a body weight below -1CO - - 2CO and -2CO - -3 CO in relation to the comparison group – 5.9% vs. 23.8% (P < 0.01) and 1.0% vs. 16.7% (P < 0.01), respectively.Weight loss after cardiac surgery in children with CHD is a well-known phenomenon and is explained by a whole complex of factors related to both physiological reactions to surgery and the peculiarities of the course of the postoperative period.In our studies, weight loss was observed in 5.6% of children in the main group, while in the comparison group this percentage increased 2.4 times and amounted to 13.4%. The frequency of weight loss in the range-2CO - - 3CO was 2.9% among children of the main group and 19.0% among children of the comparison group, which is statistically significantly higher (P < 0.01).Thus, weight loss after surgery in children with CHD is a multifactorial process: a combination of catabolism, insufficient energy intake and correction of edematous syndrome. Understanding these mechanisms is important for interpreting the dynamics of physical development and planning nutritional support in the early postoperative period.With the stabilization of heart activity and improvement of appetite in children, both in the main group and in the comparison group, active anabolism was noted. Body weight gain in the first month after surgery averaged +0.8-1.0 kg, which allowed us to return to preoperative values by 3-4 weeks (3.3±0.02 weeks). In the comparison group, the average weight gain was +0.4-0.5 kg (P<0.05), recovery to the preoperative level occurred only by 6-8 weeks (7.4±0.04 weeks).3 months after the operation, children in the main group regained weight to the standard values corresponding to children aged 3-12 months and 1-3 years, the frequency of body mass corresponding to-1CO - - 2CO and -2CO - - 3CO in the main group decreased to 5.9% and 2.0%, respectively, while in the group For comparison, these indicators reached 16.7% and 11.9%, respectively, which was significantly significant (P < 0.01).Children with CHD in both groups showed an increase in the proportion of children with a harmonious BMI in the dynamics of follow-up, but in the main group this dynamic was significantly more pronounced. In children with CHD in the main group, after 3 months of dynamic follow-up, BMI indicators corresponding to moderate nutritional insufficiency (- 1CO- -2CO) decreased by 5.8% (17.6% vs. 11.8%), while in the comparison group, there was an increase in the frequency of occurrence of children with a BMI in the range of-1CO - - 2CO by 2.4% (from 19.0% to 21.4%).Pronounced nutritional insufficiency was not observed in children of the main group after 3 months of dynamic control, whereas in the comparison group it was registered in 14.3%, which is 4.5% higher compared to the initial data. However, in children in the main group, when admitted to a hospital for surgical treatment, low BMI indicators corresponding to moderate nutritional deficiency and severe nutritional insufficiency were found in 4.9% and 1.0%, respectively, while in the comparison group these indicators were almost 6.5 times higher (21.4% vs. 19.0%, respectively). (Figure 1)
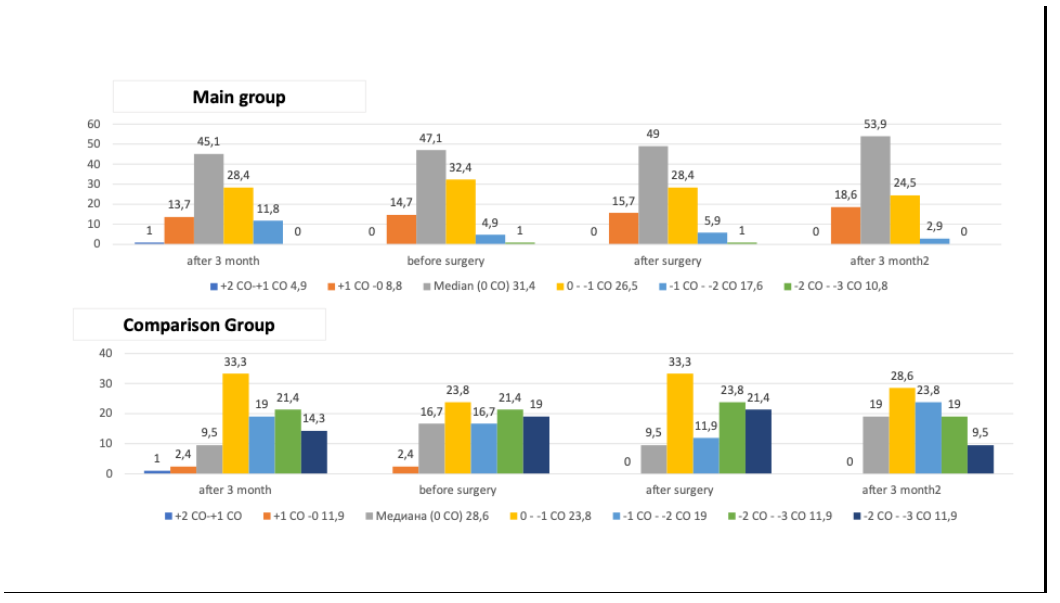 | Figure 1. Dynamics of BMI in young children with CHD depending on the method of preoperative management |
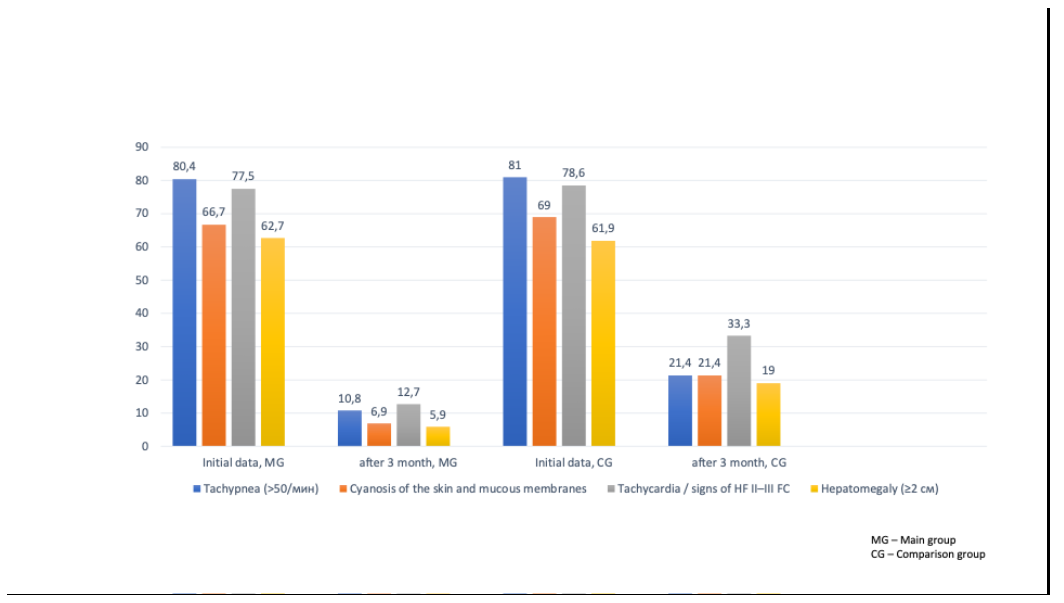 | Figure 2. Frequency of clinical symptoms in children with CHD before and after treatment |
4. Conclusions
- Thus, the study showed that 3 months after the preoperative management of children with early CHD in both groups showed improvement, but in children of the main group, the regression of symptoms was significantly more pronounced and statistically significant. A decrease in the symptoms of heart failure (dyspnea, tachypnea, sweating, hepatomegaly) is an indicator of hemodynamic stabilization, while a decrease in physical development delay reflects an improvement in the metabolic status and adequate nutritional support.