Bekbaulieva Gulistan Niyatbayevna1, Nodira Ibraximova Otabekovna2
1Dsc, Professor, Tashkent State Medical University, Tashkent, Uzbekistan
2PhD Student, Tashkent State Medical University, Obstetrics and Gynaecology Department, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Healthy generation - healthy family reserve, that into account received without to adulthood mature girls every one-sided mature development in the future family to the conditions preparation for is a criterion. According to WHO, the problem of reproductive health is in the focus of attention of scientists around the world and is one of the priorities in the Republic of Uzbekistan, where children and adolescents make up almost 40% of the population. This issue has been raised in our Republic at the state level. As an example, studies conducted in 2009 show that in the Republic of Uzbekistan, a total of 16.5% of adolescent girls aged 13-18 years had clinical signs of delayed sexual development. Special attention is paid to the period of puberty of girls and young women. Maintaining health at this age is seen as a promising contribution to the reproductive, intellectual, economic and social reserve of society. This age group determines the health of subsequent generations, mainly forms the background and structure of various gynecological diseases and possible obstetric pathologies. A pathogenetically based differential approach to the management of adolescent girls with delayed sexual development, taking into account the functional state of the sexual development system in girls. Screening examinations were conducted on 896 teenage girls aged 13-18 in schools in the city of Chirchik based on a special questionnaire. To study the functional state of the pituitary-thyroid system in the examined adolescent girls, the levels of thyroid-stimulating hormone (TSH), thyroxine (T4), and triiodothyronine (T3) in the blood serum were determined.
Keywords:
Adolescent girls, Delayed sexual development, Puberty, Thyroid gland, Menstruation, Ovarian insufficiency, Autonuclear antibodies
Cite this paper: Bekbaulieva Gulistan Niyatbayevna, Nodira Ibraximova Otabekovna, Features of Diagnosis of Delayed Sexual Development in Adolescent Girls, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3615-3619. doi: 10.5923/j.ajmms.20251510.72.
1. Introduction
Diseases that are clearly manifested in this period of life include delayed puberty. According to various authors, delayed sexual development is detected in 2.5-7% of girls, in the structure of gynecological morbidity among adolescents in the Republic of Uzbekistan this disease makes up 10.4%. Its negative consequences for the future life of adolescent girls are significant, and in most cases, even pronounced forms of delayed sexual development are diagnosed very late, and asymptomatic forms of the disease are often not diagnosed at all in the early stages, which makes it difficult to prevent diseases of the reproductive system [1,5]. There is no data on the frequency and prevalence of pathology in the regions of the republic, there is no clear idea of the ratio of various forms of delayed sexual development. The large number of causes of the disease, the clinical and pathogenetic forms, determines the problem of predicting risk factors depending on climatic, social and economic conditions [2,4].Currently, it has been proven that the thyroid gland, together with the hypothalamic-pituitary complex, plays an important role in regulating the reproductive system [3,4]. The thyroid gland is one of the main integral organs that ensure the maintenance of the body's physical and chemical homeostasis [5]. The role of the thyroid gland ensures the most important aspects of the activity of sex hormones: metabolism, brain activity, bone growth, immune system activity, physical and mental development, sexual maturation processes and other reactions [5,6]. However, the role of the thyroid gland in the pathogenesis of disorders of gonadotropic and sex hormone metabolism in adolescence, the question of its molecular function in the metabolism of sex hormones has not yet been sufficiently studied [7,8].Based on the above, taking into account the living conditions and lifestyle, as well as the characteristics of the territorial location, comprehensive study and assessment of the risk factors causing the delay in sexual development, early diagnosis of the disease, and scientific justification of the identification of risk groups, thereby reducing and preventing morbidity during adolescence [8].
2. Materials and Methods
Screening examinations were conducted on 896 teenage girls aged 13-18 in schools in the city of Chirchik based on a special questionnaire. To study the functional state of the pituitary-thyroid system in the examined adolescent girls, the levels of thyroid-stimulating hormone (TSH), thyroxine (T4), and triiodothyronine (T3) in the blood serum were determined.
3. Result and Discussion
Screening examinations were conducted on 896 teenage girls aged 13-18 in schools in the city of Chirchik based on a special questionnaire.Table 1. Age distribution of girls who underwent the examination
 |
| |
|
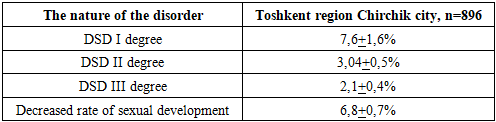
Table 2. Frequency of sexual development disorders in adolescent girls aged 13-18 years
 |
| |
|
The role of hormones in girls with delayed sexual development at the age of 13-18. Currently, there are many works that reveal the nature of the formation of the gonadotropic function of a person and the sexual characteristics of its formation in ontogenesis. The last major achievement in the study of the mechanisms of puberty is that puberty is characterized not only by the maturation of individual links of the complex combined and synchronous functional system of the brain - pituitary gland - peripheral endocrine glands, but also, most importantly, by the establishment. Long and short feedback links between them, negative and positive, provide the physiological direction of puberty and establish the cycle characteristic of the female body. In girls during the "Transition" to adolescence, the hypothalamic centers are very sensitive to the smallest amount of estrogen produced by the mature ovaries. This amount of estrogen is sufficient to inhibit hypothalamic centers that stimulate the production of tropic hormones. The early stages of puberty are characterized by a decrease in the sensitivity of the hypothalamus to sex steroids and inhibition of the secretion of gonadotropic hormones, their level gradually increases.The neuroendogenous influence of the hypothalamus centers plays a decisive role in the acceleration of the puberty process. Release of lysing hormone (luliberin) by the preoptic nuclei located in the hypothalamus ensures periodic production of gonadotropic hormones. The circadian rhythm of GnRH production and its balance is formed in adulthood and is an indicator of the maturity of neurosecretory structures of the hypothalamus. Based on these data, the concept was put forward that puberty is the process of establishing the rhythm of GnRH secretion, with its complete absence in childhood, with a gradual increase in the frequency and amplitude of impulses, until the establishment of an adult-specific rhythm. The morphological and functional maturity of the primary structures of the hypothalamus determines the gradual formation of the gonadotropic function of the pituitary gland. With the development of the rhythm and level of gonadotropins, the function of the ovaries changes, as a result, physical and sexual development is ensured. Several growth factors are involved in the biological effect of gonadotropins: epidermal growth factor, IGF-I (insulin-like growth factor-I), transforming growth factor α and β, fibroblast growth factor. At the initial stage of puberty, the secretion of gonadotropins increases, that is, the dominance of FSG biosynthesis and secretion occurs. The importance of this is that FSH leads to increased sensitivity of gonadal tissues to LH, thereby increasing the secretion of sex steroids. In addition, FSH plays a key role in regulating the maturation of follicles and oocytes. The concentration of LH increases significantly only after the age of 14 and reaches the level characteristic of women of reproductive age. At the age of 16-17 years, it is almost the same as the concentration of gonadotropin hormones characteristic of the menstrual cycle of reproductive age, and the amount of FSH is determined when a clear increase in FSH secretion appears on the 18th day of the menstrual cycle, and the second peak of LH secretion on the 22nd-23rd day of the menstrual cycle. However, the net value of FSH at this age is significantly lower than in women of reproductive age.Prolactin plays an important role in the maturation of the female body. Many authors recognize that a certain level of prolactin is necessary for the physiological process of puberty. It has been found that prolactin concentrations increase during the prepubertal period and reach adult values 1-2 years after menarche.As the concentration of gonadotropins increases, the concentration of estrogen in the blood increases. The effect of estrogens on the hypothalamic-pituitary system ensures the cyclic production of gonadotropins. Estrogens inhibit the secretion of FSH and LH, and also reduce the response of the anterior pituitary gland to the action of GnRH. The first menstruation- menstruation- is associated with the ovulatory peak of the LH against the background of endometrial development. During the menstrual cycle, the amount of estrogen increases several times, and the ratio of the main fractions changes. In the first 1-1.5 years after the onset of menstruation, the level of sex steroids in the blood serum fluctuates in a very wide range, only the dynamics of the hormonal activity of the ovaries is clearly visible. At the same time, at the end of puberty, hormonal cycles have their own characteristics: the peak of estrogen shifts to the second half of the cycle, the luteal phase is shortened, and progesterone production decreases. In women, androgens produced by ovarian stromal cells are an important component of reproductive system formation. Androgens, initially in the form of androstenedione, are converted to testosterone in peripheral tissues. At the same time, testosterone, dihydrotestosterone and dehydroepiandrosterone are also produced in small amounts in the ovaries. In the blood, testosterone and dihydrotestosterone are bound to proteins, mainly globulin. The concentration of this globulin in the blood determines the balance between androgens and estrogens. About 97.8% of testosterone in the blood is bound to globulins, the rest (about 2.2%) is free and has the characteristic of binding to the receptors of the relevant tissues and having a physiological effect. The structure of sex hormone-binding globulin is more closely related to testosterone than to estrogen. During puberty, the concentration of sex hormone-binding globulin is the same in both sexes. At puberty, its amount in blood serum decreases significantly in boys, it is 2 times less than in girls.Biogenic amines play an important role in the processes of intracerebral control of GnRH secretion. They transmit the nerve signal to the nuclei of the hypothalamus, which “translate” it into the language of the endocrine system. The role of monoamines in the regulation of gonadotropins has been proven: it is known that dopamine inhibits the secretion of prolactin, directly affecting the adenohypophysis. Excess dopamine is said to have a depressant effect on GnRH secretion. Norepinephrine, on the contrary, stimulates the release of LH, possibly stimulating the tonic secretion of gonadotropins.To date, about thirty regulatory peptides common to the nervous and endocrine systems have been identified. The control of the role of these compounds, classified as peptide neurotransmitters, is highly complementary to the mechanisms of regulation of the endocrine system, which are related to the central nervous system. The participation of neuropeptides in the regulation of the secretion of prolactin and gonadotropins has been proven. When considering the issues of neurohumoral regulation of puberty, special attention should be paid to the pineal gland. Its inhibitory effect on sexual function and, first of all, on puberty has long been known. The pineal gland produces many biologically active substances that have an antagonistic effect on gonadotropic hormones and convert environmental information into neurosecretory impulses. The main neurotransmitter of this mechanism is melatonin, the synthesis of which is regulated by impulses coming from the retina of the eye. Experiments on animals have shown that the regulation of reproductive function by the pineal gland is carried out not due to the direct effect of the pineal gland on the gonads, but due to the effect of the hypothalamic-pituitary system. In addition, the introduction of melatonin into the third ventricle of the brain reduces the level of FSH and LH and increases the level of prolactin in the blood. However, it is not clear whether the production of these substances is altered by melatonin itself or whether they modulate the activity of monoaminergic neurons and thus participate in the regulation of the production of releasing factors.The role of melatonin in the regulation of gonadotropic function in humans has been poorly studied. There is evidence of a decrease in its level in boys during puberty. However, similar changes were not found in girls. Administration of melatonin to prepubertal and pubertal children does not affect the concentration of LH and FSH. In prepubertal children, an inhibitory effect on the secretion of prolactin and growth hormone has been found. This effect disappears in adulthood. It is currently believed that melatonin plays the only role in the regulation of gonadotropic function in humans under physiological conditions.A high frequency of autoimmune thyroid diseases has been identified in patients with primary ovarian insufficiency, which may indicate the autoimmune role of autonuclear antibodies in the pathogenetic mechanisms of these pathological processes.To study the functional state of the pituitary-thyroid system in the examined adolescent girls, the levels of thyroid-stimulating hormone (TSH), thyroxine (T4), and triiodothyronine (T3) in the blood serum were determined. The summarized data of the studied parameters are presented in the table below.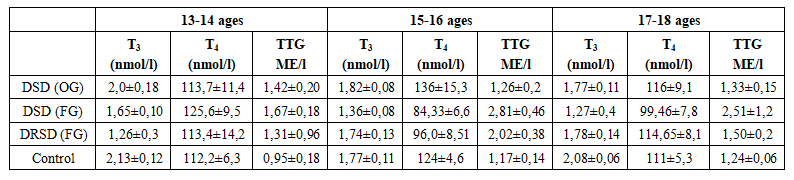 | Table 3. Central with genesis JRK sick teenager in girls pituitary-thyroid system functional status |
The degree of thyroid enlargement is determined by examination and palpation according to WHO recommendations:Grade 0 - no signs of thyroid enlargementGrade I - the size of the lumps is larger than the distal phalanx of the thumb, the lump is palpable but not visible.Grade II - the bulla is palpable and visible to the eye.Based on the table above, the average levels of thyrotropin hormone and thyroid hormones in the blood of girls with delayed sexual development did not differ from similar data in the control group, regardless of the age group. In all individuals of the specified clinical group, the individual values of the studied parameters varied within the normal range.Analysis of data from girls with a functional form of delayed sexual development revealed some features of the activity of the pituitary-thyroid system. In the sample of patients with sexual development defects due to primary amenorrhea, compared to the control group, a significant increase in the average sex hormone values in all age subgroups, as well as a significant decrease in the thyroxine level in the group under 14 years of age, was found. The average values of thyroxine concentration in patients aged 15-16 in the study group were 86.33±6.7 nmol/l, in girls with normal sexual development of the same age - 125.0±4.7 nmol/l, (P<0.01).Analysis of individual indicators of the state of the pituitary-thyroid system in this clinical group revealed the following: 9 patients (8.5%) had hormonal indicators typical of hypothyroidism. Five of them had serum TTG levels exceeding 10 mU / l with T4 concentrations below standard values and undefined T3 values, and four showed a moderate increase in TTG levels with normal T3 and T4 levels. Also, when comparing the clinical manifestations of the pathology, in the first case, the condition of the patients is considered to be pronounced, in the second - subclinical hypothyroidism (or minimal thyroid insufficiency).In the subgroups of adolescents aged 13-14 and 17-18 years, the mean values of thyrotropin, thyroxine and triiodothyronine did not reveal a statistically significant difference compared to the control group. It should be noted that, despite the absence of a statistically significant difference in the concentration of thyrotropin, a certain tendency to its increase was detected in girls with STPS, which can be observed in all age subgroups. A significant decrease in the concentration of thyroxine was detected in a sample of people aged 15-16 years - 97.0±8.52 versus 125.0±4.7 nmol/l in the control group (P<0.01).When analyzing individual parameters of the hormones of the pituitary-thyroid system, it was found that in five girls with delayed sexual development, the level of thyrotropin was higher than the norm without significant changes in the concentration of T3 and T4. In all other cases, the individual values of the considered indicators varied within the norm.The highest rate of diffuse goiter of grades I-II was found in girls with functional hypogonadism and was 88.5±2.6%.Thus, a study of the functional state of the pituitary-thyroid system in girls with a delay in sexual development of central genesis showed that there is a general relative deficiency against the background of secondary hypogonadism, not associated with organic diseases of the hypothalamic-pituitary complex. As a result of increased TSH concentration, an increase in the hormone thyroxine occurs, which causes delayed sexual development due to a transient deficiency of sex hormones.
4. Conclusions
In the city of Chirchik, 17,3% teenage girls aged 13-18 have clinical signs of delayed puberty. 4,8% of them are manifest forms, 11,7% are hidden forms of the disease.Clinical signs of retardation of sexual development are accompanied by disturbances in physical development: decrease in body mass index and deviations in the formation of the skeletal system. With the increase in the lack of sexual development, the frequency of normosthenic body type decreases, and the imbalances in the development of the chest and pelvic organs increase. Against the background of symptoms of sexual infantilism, the following secondary disorders of the menstrual function are identified in adolescent with delayed sexual development: secondary amenorrhea - 23%, opsomenorrhea -40%, long-term (more than 2 years) unstable menstruation - 29 %, of which with minor bleeding - 8%.
References
| [1] | Bekbaulieva Gulistan Niyetbaevna, Ibrahimova Nodira Otabekovna. Modern aspects of the etiopatogenesis of sexual delay in girls – adolescents Problems of biology and medicine. page 254-258, 2022, №4 (137) Tashkent Medical Academy, Republic of Uzbekistan, Tashkent. |
| [2] | G.N. Bekbaulieva, N.O. Ibrahimova. Physical development of adolescent girls with delayed sexual development. page-52. International Scientific-Practical Conference “Only English: Advances in Medical Research and Practice Conference” Tashkent May 23, 2023. |
| [3] | Heinrichs C. Normal puberty and delayed puberty. Rev Med Brux. 2011 Sep; 32(4): 256-62. |
| [4] | Ibrakhimova N.O., Bekbaulieva G.N., Jalilov F.S. Somatic background in adolescent girls with delayed sexual development. https://in-academy.uz/index.php/yo/article/view/26736. |
| [5] | On the issue of sexual development deficit in adolescent girls. page 91–92. (2024). |
| [6] | Ibrakhimova N.O., Bekbaulieva G.N. The role of chronic systemic diseases in adolescent girls with delayed sexual development. page-73 SPECIAL EDITION Only English “Advances in medical research and practice conference” Tashkent 2. ТМА 2024. |
| [7] | Jennifer Harrington, and Mark R. Palmert Distinguishing Constitutional Delay of Growth and Puberty from Isolated Hypogonadotropic Hypogonadism: Critical Appraisal of Available Diagnostic Tests Volume 97 Issue 9 | September 1, 2012. |
| [8] | N.O. Ibrahimova, G.N. Bekbaulieva. To the question of deficiency of sexual development in adolescent girls. page-56. International Scientific-Practical Conference “Only English: Advances in Medical Research and Practice Conference” Tashkent May 23, 2023. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML