-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3611-3614
doi:10.5923/j.ajmms.20251510.71
Received: Oct. 2, 2025; Accepted: Oct. 26, 2025; Published: Oct. 29, 2025

Metabolic Heterogeneity of Polycystic Ovary Syndrome Phenotypes: A Comparative Analysis of Hormonal and Biochemical Parameters
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTojieva Iroda Mirsoli kizi, Mannapova Umida Raufovna
Republican Specialized Scientific and Practical Medical Center of Endocrinology named after Y.Kh. Turakulov, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Polycystic ovary syndrome (PCOS) is characterized not only by reproductive dysfunction but also by marked metabolic disturbances. The aim of this study was to conduct a comparative analysis of the hormonal and metabolic profiles in women with different PCOS phenotypes, defined according to the Rotterdam criteria (ESHRE/ASRM, 2003). Materials and Methods: The study included 151 reproductive-aged women, divided into four phenotypes. The analysis included measurements of body mass index (BMI), insulin, HOMA-IR, lipid profile, androgens, and sex hormone-binding globulin (SHBG). Results: The most pronounced metabolic disturbances were observed in patients with phenotype A (HA+A+PCO), including elevated levels of insulin and triglycerides and reduced SHBG. Even phenotype D (A+PCO), traditionally considered metabolically favorable, showed significant signs of insulin resistance. Logistic regression revealed that triglyceride level was the only statistically significant predictor of severe insulin resistance (HOMA-IR > 3.5). Conclusion: These findings underscore the need for metabolic monitoring in all PCOS phenotypes and the importance of using phenotypic classification not only for reproductive assessment but also for metabolic stratification.
Keywords: Polycystic ovary syndrome, Phenotypes, Insulin resistance, Triglycerides, SHBG
Cite this paper: Tojieva Iroda Mirsoli kizi, Mannapova Umida Raufovna, Metabolic Heterogeneity of Polycystic Ovary Syndrome Phenotypes: A Comparative Analysis of Hormonal and Biochemical Parameters, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3611-3614. doi: 10.5923/j.ajmms.20251510.71.
1. Introduction
- Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders affecting women of reproductive age. In addition to classical gynecological manifestations such as chronic anovulation and hyperandrogenism, PCOS is characterized by pronounced metabolic abnormalities. These include insulin resistance, abdominal obesity, dyslipidemia, and an increased risk of developing type 2 diabetes and cardiovascular disease.According to the Rotterdam criteria (ESHRE/ASRM, 2003), PCOS can be classified into four phenotypes, based on the combination of three key features: hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology. Each phenotype is associated with varying degrees of hormonal and metabolic disturbance. However, it remains unclear how clinically meaningful these differences are—and whether there are distinct interaction patterns between the hormonal background and metabolic status for each phenotype. One of the most intriguing questions is the relationship between hyperandrogenism and insulin resistance within the different PCOS variants.Based on this, the aim of our study was to conduct a comparative analysis of hormonal and metabolic parameters in women with different PCOS phenotypes and to identify potential patterns in their interrelationships. Particular attention was paid to identifying statistically significant correlations between androgen levels, lipid metabolism parameters, and insulin resistance markers. Additionally, factors associated with pronounced insulin resistance (defined as HOMA-IR > 3.5) were analyzed separately.
2. Materials and Methods
- The study included data from 151 women of reproductive age with a confirmed diagnosis of polycystic ovary syndrome (PCOS) according to the Rotterdam criteria [12]. Based on phenotypic classification, the participants were divided into four groups: Phenotype A: a combination of hyperandrogenism (HA), anovulation (A), and polycystic ovarian morphology (PCO); Phenotype B: hyperandrogenism and anovulation (HA + A); Phenotype C: hyperandrogenism and polycystic morphology (HA + PCO); Phenotype D: anovulation and polycystic morphology (A + PCO).The clinical and laboratory parameters included in the analysis were: Body mass index (BMI), insulin levels, glucose, HOMA-IR (calculated as glucose × insulin / 22.4), total testosterone, sex hormone-binding globulin (SHBG), luteinizing hormone (LH), follicle-stimulating hormone (FSH), total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), and triglycerides (TG).Statistical analysis included both descriptive and inferential methods. Data were presented as medians, quartiles, means, and standard deviations. Comparison of indicators between PCOS phenotypes was performed using the non-parametric Kruskal–Wallis test. Spearman's rank correlation coefficient was used to assess relationships between hormonal and metabolic parameters. Severe insulin resistance was defined as HOMA-IR > 3.5. To identify factors associated with severe insulin resistance, a logistic regression model was built, with calculation of corresponding coefficients and p-values.
3. Results
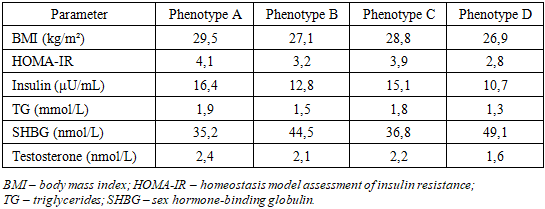
- The study included 151 reproductive-aged women with a confirmed diagnosis of polycystic ovary syndrome (PCOS), who were classified into four phenotypes according to the Rotterdam criteria (ESHRE/ASRM, 2003). The distribution by phenotype was as follows: Phenotype A (hyperandrogenism + anovulation + polycystic ovarian morphology) included 61 participants (40.4%), Phenotype B (hyperandrogenism + anovulation) — 21 participants (13.9%), Phenotype C (hyperandrogenism + polycystic ovarian morphology) — 41 participants (27.2%), Phenotype D (anovulation + polycystic ovarian morphology) — 28 participants (18.5%).Analysis using the Kruskal–Wallis test revealed statistically significant differences among PCOS phenotypes in several hormonal and metabolic parameters (Table 1).
|
|
4. Discussion
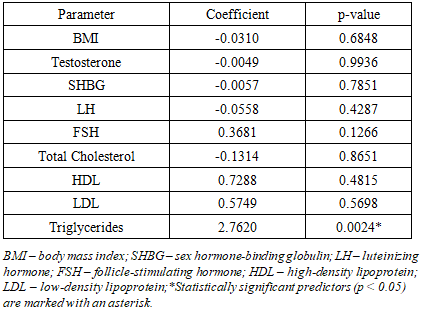
- The results of this study highlight the clinical and metabolic heterogeneity of polycystic ovary syndrome (PCOS). Phenotypic stratification allows for the consideration of not only reproductive features but also the degree of metabolic vulnerability, which is important for prognosis, clinical management, and individualized therapy.Women with the classic full phenotype (A) demonstrated the most pronounced insulin resistance, hyperinsulinemia, and dyslipidemia. HOMA-IR, insulin levels, and triglycerides were significantly elevated, while sex hormone-binding globulin (SHBG) was significantly reduced. The observed positive correlations between BMI, HOMA-IR, and TG, along with inverse correlations with SHBG, confirm the existence of an insulin–SHBG–triglyceride axis characteristic of the high-risk PCOS phenotype [2,4,5].Despite the presence of both hyperandrogenism and anovulation, phenotype B (HA + OA) showed only moderate metabolic disturbances. The inverse correlation between SHBG and BMI, as well as the positive correlation between total cholesterol and LDL, indicate the presence of early signs of dyslipidemia even against a relatively favorable metabolic background. These data support the necessity of metabolic monitoring in all PCOS phenotypes, regardless of clinical severity [6].In patients with phenotype C (HA + PCO), positive associations were found between testosterone, BMI, HOMA-IR, and lipid markers (including LDL and triglycerides), emphasizing the role of hyperandrogenism in shaping an atherogenic profile. An inverse correlation between LH and SHBG was also identified, which may reflect gonadotropin dysregulation. This hormonal–metabolic profile deserves attention not only in the reproductive but also in the cardiometabolic context [8,9].Phenotype D (OA + PCO), which lacks hyperandrogenism, is traditionally considered metabolically favorable. However, in our study, it also showed strong positive correlations between BMI, insulin, HOMA-IR, and triglyceride levels. These results emphasize that the absence of hyperandrogenism does not preclude the presence of insulin resistance, reinforcing the relevance of metabolic screening across all PCOS phenotypes [9,11].In the logistic regression model aimed at identifying predictors of severe insulin resistance (HOMA-IR > 3.5), the only statistically significant predictor was triglyceride level (p = 0.0024). Neither BMI, nor testosterone, SHBG, nor other lipid parameters reached statistical significance. This confirms that triglycerides and derived indices such as the TyG index are more sensitive markers of metabolic disturbances in PCOS than traditional anthropometric measures [12].
5. Conclusions
- The results obtained emphasize the need for metabolic monitoring in all PCOS phenotypes, including those not accompanied by hyperandrogenism. The level of sex hormone-binding globulin (SHBG) may serve as a routine and sensitive marker of insulin resistance. In addition, triglycerides represent a simple and clinically significant indicator of metabolic risk in women with PCOS. These findings support the use of phenotypic classification not only for reproductive assessment, but also for understanding metabolic risks and guiding individualized treatment strategies.