Sardorbek A. Sultanov, Azam Kh. Babadzhanov
National Medical Center, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Orthotopic liver transplantation (OLT), which has become one of the most advanced areas of modern medicine, has radically transformed the approach to treating patients with terminal stages of both diffuse and focal liver pathologies. Due to a shortage of donor organs, waiting times for surgery have significantly increased—often lasting for many months—leading to higher mortality among patients on the waiting list. As an alternative solution, transplantation of partial liver grafts obtained from living donors, most commonly relatives of the recipients, has been increasingly utilized.
Keywords:
Liver resection, Donor, Liver transplantation, Surgical anatomy
Cite this paper: Sardorbek A. Sultanov, Azam Kh. Babadzhanov, Clinical and Surgical Aspects of Donor Liver Resection in Adult Transplantation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3605-3610. doi: 10.5923/j.ajmms.20251510.70.
1. Relevance
Rapid development of transplantology and the continuously increasing demand for orthotopic liver transplantation (OLT) have resulted in a serious medical and social challenge—an acute shortage of postmortem donor organs. [2,3,4,8].A key factor in favor of living-related transplantation is the well-founded preliminary assessment of the balance between donor risk and the likelihood of a favorable outcome and recovery for the recipient. The most critical step in organizing living-related liver transplantation is donor selection, since the probability of complications largely depends on the initial health status and morphofunctional characteristics of the donor’s liver. [10,11,13]. Potential donors are recommended to be selected among the recipient’s genetic relatives over the age of 18 years, who demonstrate a high level of emotional readiness, as well as good physical and mental health. [6,12,15].The most relevant aspect of living-related partial liver transplantation is donor safety. Therefore, initiation of such programs is only feasible in specialized surgical centers with extensive experience in liver resections, along with well-developed laboratory and imaging infrastructure. The efficiency and quality of living donor selection are directly linked to the availability of qualified specialists in diagnostic imaging, functional assessment, and laboratory testing. [5,13].Irreversible chronic diseases of organs and systems, refractory to conservative or surgical treatment and leading to persistent impairment of physical or mental health, are universally recognized contraindications to living donor liver resection. [4,7,11]. These include all forms of chronic and blood-borne infections. Conversely, conditions such as acute respiratory viral infections, gastritis, uncomplicated gastric and duodenal peptic ulcers, chronic calculous cholecystitis, inguinal hernia, and nodular goiter without malignant transformation respond successfully to conservative or radical treatment and therefore are not considered contraindications to donation. [5,6,9,12,14].
2. Materials and Methods
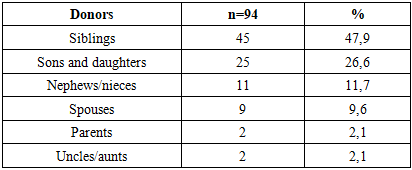
The study was based on an analysis of donor right lobe liver resections performed in 94 living-related donors (LDs). Of these, 78 procedures were carried out at the Department of Hepatobiliary Surgery and Liver Transplantation No. 2 of the Republican Specialized Center of Surgery named after Academician V. Vakhidov between April 2022 and January 2025, and 16 at the Department of Endovisual Surgery of the National Medical Center between February and June 2025. During the preoperative preparation stage, a range of diagnostic tests was conducted, including clinical laboratory evaluations and imaging studies, notably multislice computed tomography (MSCT), angiography of the abdominal cavity. The cohort included 52 males (55.3%) and 42 females (44.7%). Donors ranged in age from 18 to 51 years, with a mean age of 32.9 ± 0.9 years; 87 donors (92.6%) were between 20 and 49 years old. The distribution of donors according to their degree of kinship is shown in Table 1.Table 1. Distribution of donors by degree of kinship
 |
| |
|
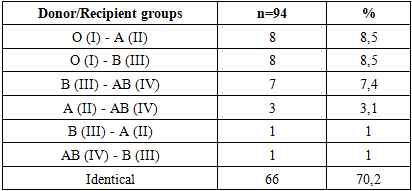
Selection of potential donorsAt the clinical and laboratory evaluation stage, determination of blood group compatibility according to the ABO system, Rh factor, and viral hepatitis markers was performed. If compatibility was confirmed (Table 2) and hepatitis was excluded, further testing was carried out. This included complete blood count and urinalysis with sediment microscopy, biochemical blood tests, coagulation profile, HIV testing, TORCH panel, among others.Table 2. ABO blood group compatibility between donors and recipients
 |
| |
|
All potential donors underwent consultations with multiple specialists, including a physician, urologist, cardiologist, otolaryngologist, dentist, nephrologist, gynecologist (for female donors), pulmonologist, narcologist, and psychiatrist.A mandatory and primary imaging modality was MSCT angiography of the abdominal cavity performed with a wide-detector CT scanner “Aquilion One – 640” (GENESIS edition). The liver’s anatomical structures were assessed, including qualitative and quantitative parenchymal evaluation, steatosis assessment, volumetric parameters, and exclusion of focal lesions. Three-dimensional reconstructions of hepatic vascular angioarchitecture were obtained, with measurements of arterial and venous diameters. The most commonly used clinical parameter for evaluating graft adequacy was the graft-to-recipient weight ratio (GRWR). [5]. In all cases, right lobe hepatectomy was planned. The graft volume was calculated relative to the middle hepatic vein, with an offset of 8–10 mm to the right. Parallel assessment of the abdominal and retroperitoneal organs was also performed to exclude additional pathologies. It should be noted that MSCT findings regarding hepatic arterial and venous anatomy were confirmed intraoperatively in all cases. Contraindications for donation included a right hepatic artery supplying segment IV, insufficient graft volume (GRWR < 0.6), and residual liver volume of less than 30%.To obtain more precise information on biliary anatomy, MR cholangiography was performed as a noninvasive alternative to traditional intraoperative cholangiography. Despite continuous improvements in MR cholangiography technology, allowing for accurate depiction of bile duct anatomy in most donors, discrepancies with intraoperative findings were noted in 6 cases (6.3%). These involved the identification of two right hepatic ducts intraoperatively. The presence of more than two bile ducts is not considered a contraindication for donation (Fig. 1). In our series, 12 donors (12.7%) had three bile ducts. In 7 (7.4%) of them, a single stump was formed on the back table by suturing the medial walls of two ducts, followed by a biliobiliary end-to-end anastomosis in the recipient. In the remaining 5 (5.3%) cases, due to a large distance (≥1.0 cm) between ducts and inability to create a common stump, two separate end-to-end biliobiliary anastomoses were performed, one of which utilized the recipient’s cystic duct for anastomosis with the donor’s accessory duct. We believe that the presence of three or more right hepatic ducts, as well as drainage of segment IV ducts into the right anterior or posterior ducts above the main biliary confluence (based on preoperative cholangiography), should be considered criteria for excluding donors from eligibility. 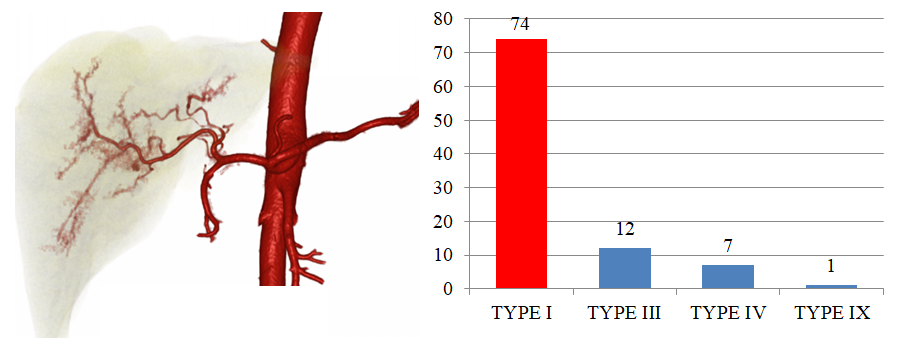 | Figure 1. Arterial anatomy according to the classification of arterial blood supply variants by N. Michels |
Surgical technique of liver resectionIn all living donors, right lobe hepatectomy was performed under preserved hepatic blood supply.To ensure optimal conditions for resection, a right subcostal incision was employed, leaving a J-shaped scar and traversing all abdominal wall muscles on the right side. After laparotomy, the round ligament of the liver was ligated and divided, and a Sigal-type retractor was placed to provide sufficient exposure.The first step following laparotomy was cholecystectomy. The cystic duct and artery were mobilized in the region of the gallbladder neck, ligated separately twice, and then divided. A longer cystic duct stump was intentionally left for performing a white test to assess the integrity of the right hepatic duct stump closure. The gallbladder was removed in a subserosal plane, starting either from the neck or the fundus. After dissection of the anterior layer of the hepatoduodenal ligament along the cystic artery, the right hepatic artery was identified and isolated. Verification of hepatic arterial anatomy was carried out according to Michels’ classification (1962). Based on this system, four types were identified among the 94 donors: Type I in 74 donors (78.7%), type III in 12 donors (12.7%), type IV in 7 donors (7.4%), rare Type IX in 1 donor (1.1%) (Fig. 1).The right branch of the portal vein and the right hepatic duct were also dissected, along with their left counterparts. The right hepatic duct was mobilized for approximately 1 cm to preserve its blood supply and minimize postoperative biliary complications such as bile leakage, biloma, or stricture. In cases of high anatomical variations or technical difficulty during duct mobilization (4 donors, 4.3%), the right hepatic duct was identified only at the final stage of parenchymal transection. This led to a modification of the surgical approach, with subsequent mobilization of the right hepatic duct performed only after transection of the liver parenchyma down to the biliary plate, ensuring better visualization of small accessory ducts not detected on MR cholangiography.Liver mobilization proceeded by dividing the falciform, coronary, and triangular ligaments. Sharp and blunt dissection of the coronary ligament exposed the right hepatic vein at its junction with the inferior vena cava (IVC). By elevating the right lobe medially, the parietal peritoneum was incised and the right adrenal gland separated from the liver, providing access to the retrohepatic segment of the IVC. Using bipolar forceps and a dissector, retrohepatic veins draining into the IVC were isolated. Veins ≥6 mm in diameter were preserved for hemodynamic assessment during back table graft perfusion, while veins ≤5 mm were clipped with titanium clips (Ligaclip Ethicon LT-100, LT-200, LT-300) and divided. Veins ≤1 mm were divided after bipolar coagulation. Following mobilization of the right lobe from the IVC, a vascular sling was passed around the right hepatic vein, retrohepatic veins (if present), the right portal vein, the right hepatic artery, and the right hepatic duct to facilitate a “hanging maneuver.” The resection line was defined using intraoperative Doppler ultrasonography. Anatomical landmarks included the interval between the middle and right hepatic veins at the caval hilum and the gallbladder fossa. These points were connected by a line drawn 1 cm lateral and parallel to the course of the middle hepatic vein within the parenchyma, as visualized with Doppler. The line continued through the gallbladder fossa to the hepatic hilum, where the biliary confluence served as a landmark. Parenchymal transection was performed with a CUSA Clarity ultrasonic dissector, supplemented by bipolar electrocautery with saline irrigation. Vessels encountered during dissection were ligated or clipped and divided. Veins ≥5 mm were preserved as potentially hemodynamically significant until graft flushing at the back table. Functionally active veins were reconstructed using polytetrafluoroethylene (PTFE) vascular grafts of appropriate diameter for subsequent anastomosis to the recipient’s IVC. During posterior surface transection, both ends of the previously placed sling were elevated to maintain traction, thereby minimizing the risk of injury to the IVC and left lobe hepatic veins.After completing parenchymal transection, the connective tissue biliary plate and the right hepatic duct were divided (Fig. 2). The ducts were probed with a fine metal bougie to confirm the entry site of the left duct and detect any small accessory ducts not visualized on MR cholangiography. Only then was the right hepatic duct definitively transected. In 6 cases (6.4%), such accessory ducts 1–2 mm in diameter were identified intraoperatively.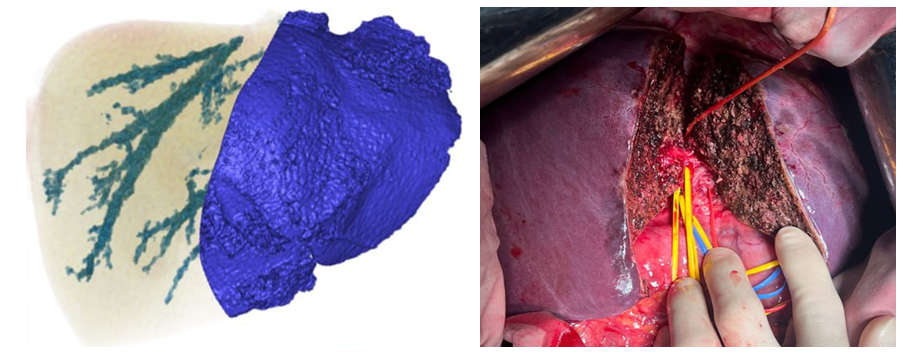 | Figure 2. Reconstruction of the hepatic veins (MSCT) and the completed stage of liver resection (intraoperative photo) |
Upon graft retrieval, donor vascular stumps were closed: the right portal vein stump was sutured transversely with continuous Prolene 6-0 to prevent narrowing or kinking; IVC defects were repaired longitudinally with continuous Prolene 5-0; accessory veins with Prolene 6-0; and the right hepatic duct stump was closed transversely with continuous PDS 7-0. White test (injection of propofol diluted 1:1 with normal saline through the cystic duct after clamping the distal common bile duct) was performed to confirm biliary stump integrity. If no leakage was observed, the cystic duct stump was doubly ligated. Final hemostasis and biliostasis were confirmed. The raw liver surface was reinforced with Surgicel Fibrillar. The falciform ligament was sutured to prevent torsion of the left lobe and compression of hilar structures. The donor operation concluded with drainage of the right subdiaphragmatic space and layered closure of the abdominal wall.
3. Results
Among all examined donors, blood group I predominated (36.2%, see Table 2). Donors with blood group II accounted for 28.7%, group III for 30.8%, and group IV for 4.3%. The majority, 88 donors (93.6%), had a positive Rh factor. Of the 6 donors (6.4%) with Rh-negative blood, 5 livers were transplanted into Rh-positive recipients, while in 1 case (1.0%) both donor and recipient were Rh-negative.The mean cold ischemia time was 40.2 ± 0.7 minutes, depending on the number and presence of accessory veins requiring anastomosis with PTFE grafts at the back table stage. In 15 cases (16%), veins from segments V and VIII were sutured into a single prosthesis using end-to-end or end-to-side techniques. In 11 cases (11.7%), segment V veins, and in 3 cases (3.2%), segment VIII veins were independently reconstructed into prostheses by end-to-end anastomosis. In 2 cases (2.1%), a segment VIII vein, located less than 1 cm from the right hepatic vein, was incorporated into its medial margin, forming a common stump. In another 2 cases (2.1%), portal vein trifurcation was identified on MSCT, and given the short distance (~1 cm) between branches, the veins were unified at the back table, creating a single stump (Fig. 3).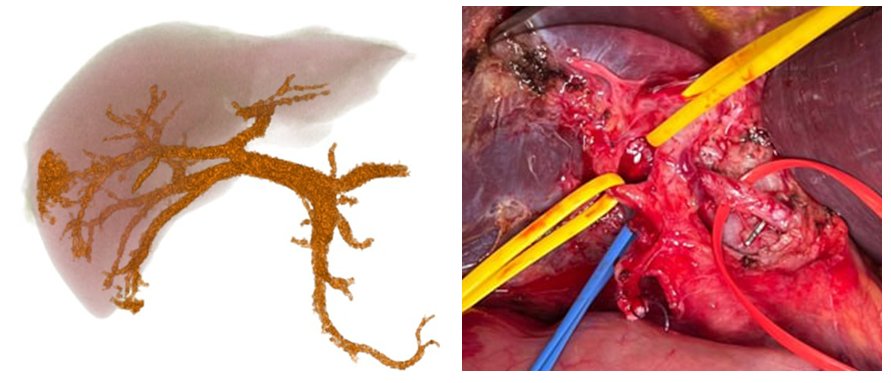 | Figure 3. Trifurcation of the portal vein. (CT scan and intraoperative photo) |
Portal vein anatomy was classified according to T. Nakamura et al. (2002). Among 94 donors, three types were identified: Type A in 89 donors (94.6%), type B in 3 donors (3.1%), type C in 2 donors (2.2%) (Fig. 4).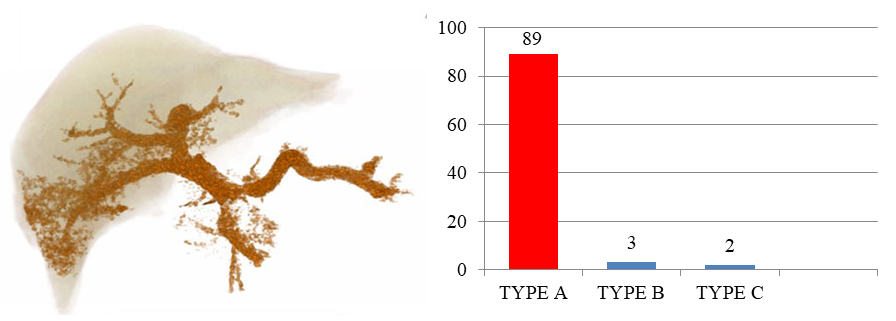 | Figure 4. Distribution of portal anatomy according to the classification of T. Nakamura et al. (2002) |
Retrohepatic veins were detected in 18 donors (19.1%), of which 8 (8.5%) were found to be functionally significant during graft perfusion and preserved for anastomosis with the recipient’s IVC.Donor complicationsAs with any surgical procedure, donor hepatectomy carries inherent risks of complications. Reported complication rates in different transplant centers vary widely (0–67%), largely due to differences in donor selection criteria and the absence of a standardized classification system for donor complications. In this study, complications were categorized using the modified Clavien classification.On postoperative day 1, all donors demonstrated mild hyperbilirubinemia (total bilirubin 35–45 μmol/L) and moderate elevation of transaminases (ALT and AST 110–140 U/L), which normalized by day 5. In 3 cases (3.1%), bilomas of the right subdiaphragmatic space were detected on ultrasound between days 7 and 10 postoperatively, manifesting as pain. All 3 donors underwent percutaneous drainage, followed by endoscopic retrograde cholangiography, which showed no extravasation of contrast. The bilomas were attributed to bile leakage from the resection surface. In the first case, the donor was discharged on day 12 with a drainage tube, which was later removed in an outpatient setting after 2 weeks. In the other two cases, 350–400 mL of biloma fluid was evacuated, with no recurrence, and drains were removed after 2–3 days. In 1 donor (1.0%), biliary stricture developed at the stump of the right hepatic duct on postoperative day 8, presenting with obstructive jaundice. Relaparotomy was performed with Roux-en-Y hepaticojejunostomy. The donor was discharged in satisfactory condition. In 1 donor (1.0%), intra-abdominal bleeding was noted on postoperative day 4. Percutaneous drainage evacuated old hemorrhagic fluid. Since no active bleeding was observed, relaparotomy was not required, and the patient was discharged on day 10 after drain removal. In 1 donor (1.0%), right-sided hydrothorax was diagnosed on postoperative day 7, and approximately 400 mL of clear fluid was evacuated by thoracentesis.In the long-term period, 1 donor (1.0%) developed a ventral incisional hernia one year after surgery, associated with lifting heavy weights. The patient underwent successful allohernioplasty.
4. Discussion and Conclusions
Donor safety is the most critical factor in living-related partial liver transplantation. Therefore, the implementation of such programs is feasible only in specialized surgical centers with extensive experience in liver resections and a well-developed diagnostic and instrumental infrastructure.A critically important stage of the procedure is the precise identification and meticulous dissection of hepatic arteries, portal vein branches, and segmental bile ducts. The degree of anatomical accuracy and surgical technique at this stage directly determines both the preservation of the donor’s remnant liver and the safety of the donor, as well as the functional autonomy and viability of the graft.It should be emphasized that living-related liver transplantation continues to expand globally, reflecting its sustained growth and development. This trend is driven not only by the organizational, legal, and social challenges of cadaveric organ donation but also by several advantages of living donation. These include sufficient time for thorough preoperative preparation of both donor and recipient, minimization of cold ischemia time, the possibility of close genetic compatibility (reducing the risk of rejection), and the opportunity to lower both the dosage and duration of immunosuppressive therapy.
References
| [1] | Voskanyan S.E., Kolyshev I.Yu., Bashkov A.N., et al. Efferent blood supply to the right lobe of the liver in terms of its transplantation from a living donor: variant anatomy, classification. Part 1. Annals of surgical hepatology. 2023. Vol. 28. No. 1. P 10-24. |
| [2] | Gauthier S.V., Monakhov A.R., Gallyamov E.A., et al. Laparoscopic collection of liver fragments from a living related donor for transplantation to children // Annals of surgical hepatology. - 2018. |
| [3] | Granov A.M., Granov D.A., Zherebtsov F.K., et al. Liver transplantation at the Russian Scientific Center of Radiology and Surgery. Experience of 100 operations // Bulletin of Transplantology and Artificial Organs - 2012. -Vol. XIV - №4. - P. 11-16. |
| [4] | Dzhanbekov TA Use of "large" grafts of the left lateral sector of the liver in children with low body weight: diss. ... Cand. of Medicine / Dzhanbekov TA - Moscow, 2015. - 122 p. |
| [5] | Devyatov AV et al. Instrumental diagnostics of hepatic encephalopathy in patients with liver cirrhosis before and after portosystemic shunting // Bulletin of Experimental and Clinical Surgery. - 2011. - V. 4. - No. 3. - P. 431-435. |
| [6] | Kim EF, Bekbauov SA, Ashuba TM, Bogdanov-Berezovsky AA et al. Clinical and surgical issues of intravital donation of liver fragments // Transplantology. – 2009. No. 1. P. 5-12. |
| [7] | Malinovskaya Yu. O. Preparation for transplantation. Brochure for candidates for organ transplantation. Moscow, 2023. p. 33. |
| [8] | Monakhov A. R. Living donation of liver fragments for transplantation to children: diss. ... Cand. Sci. (Medicine) / A. R. Monakhov. – Moscow, 2015. – 156 p. |
| [9] | Nazirov F. G. et al. Features of the development and course of complications of portal hypertension in patients with HBV- and HCV-etiology of the liver cirrhosis // Bulletin of Surgery named after I. I. Grekov. – 2011. – Vol. 170. – No. 1. – P. 22-29. |
| [10] | Semash K. O. Robotic surgery in terms of liver transplantation // Transplantology. – 2024. Volume 16. No. 3. P. 373-382. |
| [11] | Sultanov S. A. и др. Instrumental diagnostics of hepatic encephalopathy at patients with liver cirrhosis before and after portosystemic shunting // Journal of Experimental and Clinical Surgery. – 2011. – Т. 4. – №. 3. – С. 431-435. |
| [12] | Ali Deeb A, Settmacher U, Fritsch J, Dondorf F, Rohland O, Rauchfuß F. Sarcopenic obesity may predict worse liver regeneration after right graft living donor liver transplantation. Liver Transpl. 2024 Apr 1; 30(4): 412-420. doi: 10.1097/LVT.0000000000000238. Epub 2023 Aug 7. PMID: 37548548. |
| [13] | Anılır E, Oral A, Atasoy A, Civan HA, Topçu FS, Bayramoğlu M, Şahin E, Dirican A, Ünal B. A Single-Center's Early Surgical Outcomes of Living Donor Liver Transplantation. Transplant Proc. 2023 Jun; 55(5): 1209-1213. doi: 10.1016/j.transproceed.2023.03.028. Epub 2023 Apr 28. PMID: 37121859. |
| [14] | Broering DC, Raptis DA, Elsheikh Y. Pioneering fully robotic donor hepatectomy and robotic recipient liver graft implantation – a new horizon in liver transplantation. Int J Surg. 2024; 110(3): 1333–1336. PMID: 38181111 https://doi.org/10.1097/JS9.0000000000001031. |
| [15] | Babadjanov A. K., Sultanov S. A., Ibrohimov S. S. Features of the variant anatomy of the vascular and biliary liver architectonics in related donors // International Journal of Humanities and Natural Sciences. – 2025. – №. 1-3 (100). – С. 28-33. |
| [16] | Babadjanov A. et al. Features of surgical technique of donor explantation of the right lobe of the liver // science. – 2025. – Т. 4. – №. 1-4. – С. 51-58. |
| [17] | Cheah YL, Yang HY, Simon CJ, Akoad ME, Connor AA, Daskalaki D, Han DH, Brombosz EW, Kim JK, Tellier MA, Ghobrial RM, Gaber AO, Choi GH. The learning curve for robotic living donor right hepatectomy: Analysis of outcomes in 2 specialized centers. Liver Transpl. 2025 Feb 1; 31(2): 190-200. doi: 10.1097/LVT.0000000000000480. Epub 2024 Oct 24. PMID: 39441028; PMCID: PMC11732260. |
| [18] | Nazirov F. et al. Resection techniques in related liver transplantation // Science and innovation. – 2024. – Т. 3. – №. D6. – С. 71-77. |
| [19] | Nazirov F. G. et al. The Probability of Applying Splenosuprarenal Anastomosis Subject to Angio-architectonics of Lineal and Left Renal Basin Vessels // American Journal of Medicine and Medical Sciences. – 2018. – Т. 8. – №. 2. – С. 31-36. |
| [20] | Nazirov F. G. et al. Angioarchitectonics and histostructure of the vessels of splenal and left renal basins in patients with portal hypertension // Journal of gastroenterology and hepatology. – 111 river st, hoboken 07030-5774, nj usa: wiley-blackwell, 2012. – Т. 27. – С. 228-228. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML