-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3600-3604
doi:10.5923/j.ajmms.20251510.69
Received: Sep. 21, 2025; Accepted: Oct. 16, 2025; Published: Oct. 29, 2025

Contemporary Principles of Diagnosis and Treatment for Pleural Empyema
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRadzhabov Doston O`ktamovich
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Radzhabov Doston O`ktamovich, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction. Diagnosis and treatment of pleural empyema remains an urgent problem in surgery. The term pleural empyema or pyothorax is considered to be limited or widespread inflammation of the visceral and parietal pleura, occurring with the accumulation of pus in the pleural cavity and accompanied by signs of purulent intoxication. The purpose of the study – to examine the principal causes and factors associated with purulent pleuritis, and to develop tactical and technical approaches to improve the efficacy of comprehensive treatment for pleural empyema using modern technologies. Materials and research methods: A total of 102 patients with pleural empyema, aged between 20 and 80 years, were observed; 79 (78%) were men and 23 (22%) were women. 89 (88%) of the participants were residents of rural areas. There were 12 patients, comprising 11% of urban dwellers. The results of the study and their discussion. The study's results indicated a rise in pleural empyema instances, increasing from 8 cases in 2021 to 2025. In recent years, patients have frequently been admitted in critical condition due to a prevalent form of the disease, particularly following the rupture of a suppurative echinococcal cyst, cystic cavities, and lung abscesses into the pleural cavity. Based on the location of fluid accumulations in the pleural cavity, we have classified the following forms of pleural empyema among our patients. Conclusion. The examination of treated cases indicates a rise in the number of patients with pleural empyema, escalating from 8 instances in 2021 to 26 in 2025. The utilization of computed tomography, ultrasonography, and videothoracoscopy has markedly enhanced the identification of pleural empyema, particularly in cases of blocked forms.
Keywords: Pleural empyema, Clinic, Diagnostic, Combined treatment
Cite this paper: Radzhabov Doston O`ktamovich, Contemporary Principles of Diagnosis and Treatment for Pleural Empyema, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3600-3604. doi: 10.5923/j.ajmms.20251510.69.
Article Outline
1. Introduction
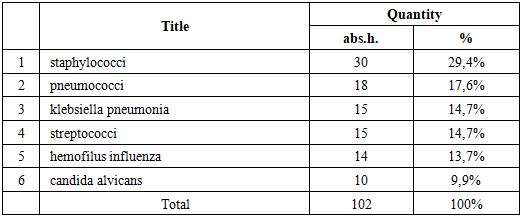
- Diagnosis and treatment of pleural empyema remains an urgent problem in surgery. The term "pleural empyema" or "pyothorax" is considered to be limited or widespread inflammation of the visceral and parietal pleura, occurring with the accumulation of pus in the pleural cavity and accompanied by signs of purulent intoxication [1]. According to a number of authors, in almost 90% of patients, pleural empyema occurs as a result of complications of the purulent-inflammatory process in the lungs (against the background of acute pneumonia, 4%, lung abscess – 9-11%, with lung gangrene – 80-95%) [2,3]. As a result of wounds and injuries to the chest organs – 6-12%, the main cause is illiquid post-traumatic pleurisy and hemothorax [1,4,5]. Postoperative pleural empyema accounts for 2 to 28% of the cause, and most often occurs after pneumonectomy [5,8]. During bacteriological examination of the contents Gram-negative flora occurs in 20-30% of cases in the oral cavity. Gram-positive flora is sown in 30-40%, mainly S. aureus, S. pneumoniae, S. pyogenes. In 20-30%, the flora is mixed, combined with non-clostridial anaerobes [5-7].The purpose of the study – to examine the principal causes and factors associated with purulent pleuritis, and to develop tactical and technical approaches to improve the efficacy of comprehensive treatment for pleural empyema using modern technologies.
2. Materials and Research Methods
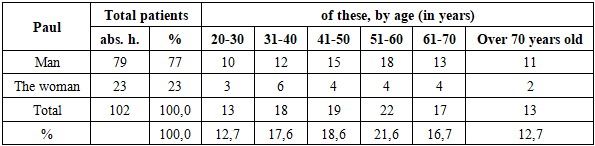
- A total of 102 patients with pleural empyema, aged between 20 and 80 years, were observed; 79 (78%) were men and 23 (22%) were women (Table 1). 89 (88%) of the participants were residents of rural areas. There were 12 patients, comprising 11% of urban dwellers.
|
3. The Results of the Study and Their Discussion
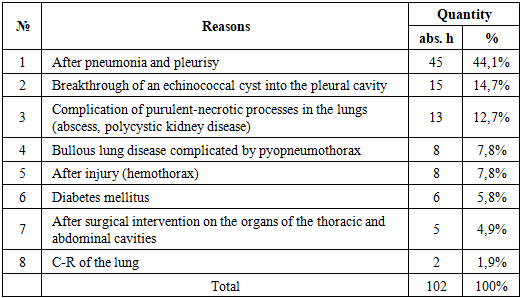
- The study's results indicated a rise in pleural empyema instances, increasing from 8 cases in 2021 to 2025. In recent years, patients have frequently been admitted in critical condition due to a prevalent form of the disease, particularly following the rupture of a suppurative echinococcal cyst, cystic cavities, and lung abscesses into the pleural cavity. Based on the location of fluid accumulations in the pleural cavity, we have classified the following forms of pleural empyema among our patients.In our study of 45 patients, we found that pleural empyema occurred in 53.8% of cases due to pneumonia complicated by pleurisy of various origins, resulting from infection entering the pleural cavity via lymphogenic or hematogenic routes. In 21 instances, suppuration of pleural effusion was associated with the emergence of necrotic foci in the pulmonary parenchyma, resulting in the establishment of a bronchopleural fistula.In 15 cases (11.5%), patients were admitted due to the rupture of a suppurative echinococcal cyst into the pleural cavity, resulting in the development of a pyopneumothorax. Thirteen patients (12.7%) with polycystic lung disease experienced pyopneumothorax due to the rupture of one or more subpleurally situated abscesses or purulent cysts into the pleural cavity.Factors contributing to pleural empyema are extensive and complex, resulting in the development of a bronchopleural fistula.Pleural empyema developed in 8 cases (7.8%) due to the suppuration of hemothorax associated with rib fractures. In 8 individuals (7.8%), the etiology of empyema was an abrupt rupture of pulmonary air cysts. In 6 (5.8%) diabetic individuals with diabetic nephropathy, hydrothorax was worsened by pleural empyema. Following surgery on the thoracic and abdominal organs, 5 individuals (4.9%) experienced recurrent pleural cavity infections, resulting in pleural empyema. In 2 individuals (1.9%), pleural empyema developed due to the collapse of a lung tumor. Our observations indicate that the existence of a bronchopleural fistula consistently serves as both a contributory and exacerbating element in the purulent-inflammatory process within the pleural cavity, resulting in a protracted course of pleural empyema. Patients were categorized into two groups based on the disease onset and the duration of the inflammatory process. The initial cohort with acute pleural empyema comprised 41 patients who had experienced 8-12 weeks after the disease's onset. The second cohort with a chronic disease trajectory comprised 61 individuals who had experienced symptoms for over 12 weeks following disease onset. The synchronization of the acute process was induced by multiple variables. Frequent inadequate management of acute pulmonary suppuration, accompanied by pyopneumothorax, resulted in chronic empyema.Our observations indicate that the clinical presentations of pleural empyema, irrespective of etiology, predominantly exhibited common symptoms. The patients primarily expressed concerns with the following symptoms: cough with purulent sputum, dyspnea, pleuritic chest discomfort, fever, and indications of intoxication.Persistent and recurrent coughing episodes accompanied by substantial sputum production suggested the existence of a bronchopleural fistula. In the early phases of the disease, individuals with complete and subtotal empyema experience significant discomfort and dyspnea. They frequently adopted a constrained semi-sitting posture. In cases of minor empyema that were delimited (lumped), the pain condition was less prominent.Upon inspection of the chest, the compromised side was noted to lag during respiration. The intercostal gaps were enlarged and flattened as a result of exudate pressure. The presence of exudate in the pleural cavity was marked by diminished or absent vocal tremors and respiratory sounds.In individuals with pleural cavities containing only exudate, the upper boundary of dullness aligned with the Ellis-Damoiseau-Sokolova line, which extends laterally and superiorly from the spine to the posterior axillary lines, then descends anteriorly to the mid-clavicular line.Typically, when a significant volume of pus accumulates in the pleural cavity, patients exhibit displacement of the mediastinal organs towards the unaffected side and compression of the healthy lung. In individuals with pyopneumothorax, a dull percussive sound was observed under the upper horizontal boundary indicating pus collection, while a tympanic sound was noted above the area of air accumulation. Auscultation was used to assess the reduction or near-total absence of respiratory sounds and heightened bronchophony in the region of exudate buildup. In the context of a bronchopleural fistula and an adequately drained bronchial cavity, heightened bronchial respiration (amphoric) was seen. Concurrently, patients had abundant purulent sputum accompanied by an offensive odor. Multiple organ failure was found in 25 cases among our patients at the clinic.The analyses indicated that alterations in the overall clinical parameters of blood and urine in pleural empyema were consistent with those observed in other severe purulent diseases.The general blood test indicates high leukocytosis (exceeding 10×10^9/l), a pronounced leftward shift in leukocyte count, and elevated ESR. Anemia was frequently noted. The plasma protein content diminished, primarily attributable to albumin. Albuminuria and the presence of granular and hyaline casts were identified in the urine. The cytological and histological analysis of pleural cavity contents is crucial for diagnosis and guiding antibiotic selection.
|
|
4. Conclusions
- The examination of treated cases indicates a rise in the number of patients with pleural empyema, escalating from 8 instances in 2021 to 26 in 2025. The utilization of computed tomography, ultrasonography, and videothoracoscopy has markedly enhanced the identification of pleural empyema, particularly in cases of blocked forms. An appropriate amalgamation of intricate etiopathogenetic therapy, prompt drainage of the pleural cavity, and timely radical surgical surgery has markedly enhanced treatment outcomes in both acute and chronic forms of pleural empyema. The management of pleural empyema, seen as a polyetiological condition, must be thorough.