Ergasheva N. N.
Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Ergasheva N. N., Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent State Medical University, Tashkent, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The article presents an “analysis of our clinical data on the diagnosis and treatment results of 321 patients: 156(48.6%) boys and 165(51.4%) girls aged from one day to 18 years with latent spinal dysraphism of various forms in combination to spinal malformations. Spinal hernias were detected in 219(68.2%); spina bifida occulta - in 102(31.8%): in association patients with anorectal and urogenital anomalies-in 51 (50 %), urogenital anomalies-in 13 (12,75%); 30(29,41%) patients with pathology of the large intestine and in 8 (7.84%) - in an isolated form. The paper confirms the need for a comprehensive approach to diagnosis with the determination of combined anomalies of the spine, spinal cord and the causes of neurological disorders.
Keywords:
Spinal dysraphism, Spinal cord hernias, Spina bifida occulta, Anorectal and urogenital anomalies, MSCT, MRI
Cite this paper: Ergasheva N. N., Combined Latent Spinal Dysraphism within the Structure of Myelodysplasia and Its Role in the Development of Coloproctological and Urogenital Abnormalities in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3574-3579. doi: 10.5923/j.ajmms.20251510.62.
1. Introduction
Spinal dysraphism is manifested by open spina bifida with the formation of a cystic spinal hernia (spina bifida cystica uverta) (spina bifida aperta); closed form (spina bifida occulta); Spina bifida with soft tissue involvement and spinal cord extension along its entire length or only in a certain segment (rhachischiasis totalis et partialis) [2,12].The lumbosacral spine accounts for 87% of various forms of latent spinal dysraphism (SSD), the frequency of which is 0.05-0.25 cases per 1000 newborns (A. A. Arendt, 1968; A. G. Pritko et al., 1999; Warder D. E., 2001 José Murillo B. Netto, MD, PhD André N. Bastos, MD 2010). Some authors considered this condition as a variant of the norm, since it is more often asymptomatic and is detected accidentally during X-ray examination of the spine [4]. The detected changes caused increased attention of specialists to this pathology. Neurosurgeons considered expedient surgical treatment with the appearance of signs of pathology [1,5]. With this anomaly, more often there are no obvious symptoms. However, some patients show symptoms of loss, irritation of the nervous system in the form of lumbosacral pain, hyperesthesia, paresthesia in the lower extremities. With typical localization of spinal dysraphism in the lumbosacral region, various vertebral anomalies occur, combined with anorectal, urogenital anomalies and pathology of the colon with pelvic organ dysfunction [3]. There is still no consensus on the frequency of latent spinal dysraphism. [7,8]. In the United States, the level of Spina bifida did not decrease below 3.4 cases per 10,000 live births, despite the use of folic acid and other preventive measures to eliminate possible causative factors (Boulet S. L. et al., 2015, Kondo A. et al., 2012). Many publications are devoted to the diagnosis of malformations of the caudal parts of the neural tube. MRI, CT, ultrasound and neurophysiological diagnostic methods play an important role in the complex of examinations of patients with manifestations of spinal dysraphism [9,10]. The disadvantages of diagnostic and treatment methods require further research.Spinal dysraphism is a collective concept that combines pathologies with a common mechanism of development, diverse in the form of incomplete overgrowth of medially located mesenchymal, bone and nerve structures; often with hidden clinical and neurological disorders of the musculoskeletal system, pelvic organs and other systems. Severe neurological symptoms are observed when the dural sac is compressed through a bone defect, roots or spinal cord parts are fixed [4].The aim of the study was to improve the diagnosis, treatment results, and methods of social adaptation of children with latent spinal dysraphism in combination to other osteoneural malformations and functional disorders of other organs and systems.
2. Material and Methods of Research
The study is based on the analysis of the diagnosis and treatment results of 321 patients (156(48.6%) boys and 165 (51.4%) girls) aged from one day to 18 years with latent spinal dysraphism of various forms in combination to other types of spinal malformations. Spinal hernias were detected in 219(68.2%); spina bifida occulta - in 102(31.8%): in association with anorectal - in 51 (50 %), urogenital - in 13(12.75%) anomalies, in 30 (29.41%) patients - with colon pathology and in 8 (7.84%) - in an isolated form, accompanied by disorders of the act of defecation and urination. The patients were treated in the Department of elective Surgery of the State Clinical Hospital No. 2 in Tashkent and in the children's department of the National Research Center of National Economy of the Ministry of Health of Uzbekistan. They were divided into two groups. The comparison group consisted of 77 (24%) patients observed in 2016-2018. Examinations were carried out according to generally accepted diagnostic methods. The main group included 244 (76%) patients who were followed up in 2020-2023. Spinal pathology was verified by taking into account the data of functional and instrumental studies: ultrasound, MSCT, MRI of the brain, spinal cord, and spinal column; electroneuromyography (ENMG) of the muscles of the lower extremities. To assess the anatomical and functional state of the colon and genitourinary system, ultrasound, irrigography, and intravenous urography were performed using a digital X - ray machine or MSCT. The condition of the vertebrae, the structure and location of the spinal cord cone, and the terminal thread were evaluated; additional formations were identified.When studying the initial neurological status of children, special attention was paid to assessing the functions of the spinal cord with the definition of motor, sensory, trophic disorders; disorders of urination and defecation.
3. Results and Their Discussions
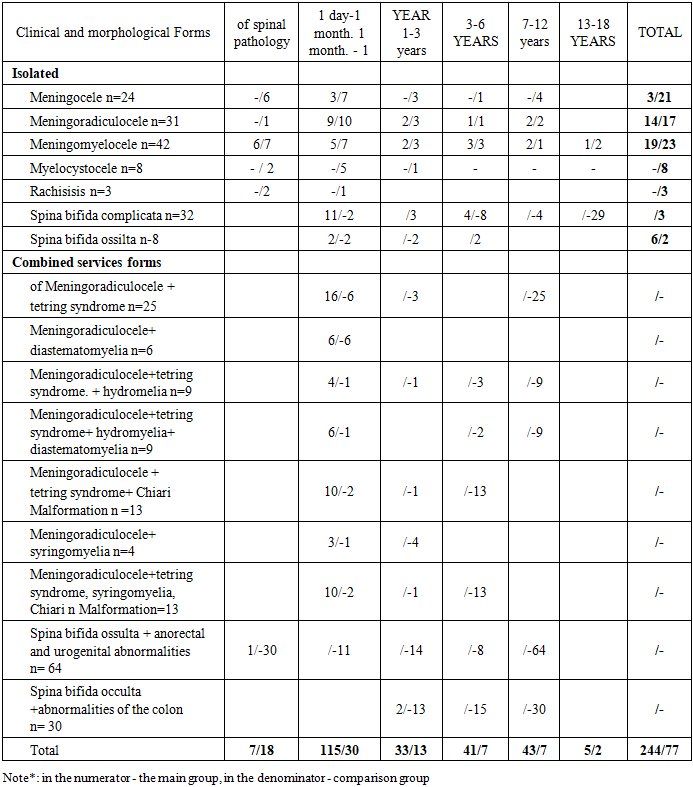
The distribution of patients by age, gender and nosological forms is presented in Table 1. Table 1. Distribution of patients by age, gender, and nosological forms of myelodysplasia
 |
| |
|
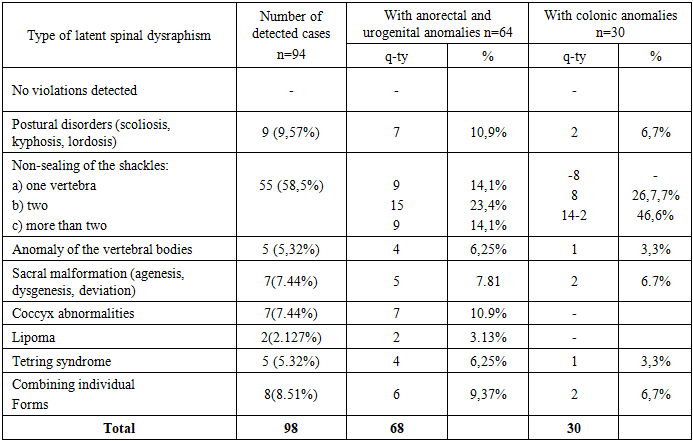
As can be seen from the table, in 219 (68.2%) patients, variants of latent spinal dysraphism were observed in various clinical and morphological forms of spinal hernia. These patients have a combination of osteoneural abnormalities in the form of such spinal pathologies and spinal malformations as diastematomyelia, spinal lipomas, syringomyelia, and hydromyelia separately or in various combinations, usually leading to fixed spinal cord syndrome. It should be emphasized that out of 69 patients with SPSM, the origin (primary or secondary) of these disorders in 15(21.74%) remained unclear, since they did not undergo MRI and MSCT studies before surgery. In 37 (53.62%) patients, these phenomena were diagnosed before surgery; in 17(24.64%), they appeared after surgery at the stages of conservative therapy and rehabilitation due to the progression of residual neurological phenomena and pelvic organ dysfunction. Delayed detection of latent dysraphism in these cases is associated with incomplete examination of patients in the comparison group using highly informative diagnostic methods (MSCT, MRI) or surgical intervention in connection with complications that required emergency tactics. Thus, the syndrome of secondary spinal cord fixation in the postoperative period can be caused by various reasons: failure to eliminate hidden spinal malformations during surgery, pathological fixation and/or the occurrence of these forms of myelodysplasia after surgery. The inclusion of 94 (29.3%) patients with spinal dysraphism combined with abnormalities of other organs and systems is explained by the fact that in recent years the number of patients admitted to the pediatric surgical clinic with anorectal, urogenital anomalies, and congenital malformations of the colon has significantly increased. A comprehensive examination revealed violations of colon motility and functional disorders of the pelvic organs with a normal and satisfactory anatomical structure. Some patients did not have any positive effect after surgical treatment at all or had a low unstable positive effect. These findings prompted further investigation into spinal abnormalities among children with these pathologies aimed at identifying concomitant spinal pathology in order to determine the appropriate treatment together with neurologists. The patients in this group were dominated by bone disorders in the form of lumbosacral dysraphism against the background of rare variants of spinal malformation. The analysis of our observations showed that the clinical manifestations of latent spinal dysraphism are polymorphic and non-specific. In severe forms of spinal hernias in combination to primary spinal malformations (diastematomyelia, lipoma, hydromyelia, syringomyelia) of 79 patients, 55 (69.6%) had neurological disorders in the form of disorders of the act of urination and defecation, paresis of the lower extremities, sensitivity disorders in the perineum and lower extremities, as well as trophic disorders in some patients they were noticeable during the newborn and infancy period. In 24 (30.4%) patients, these phenomena were observed in the form of progression of residual neurological symptoms in the immediate and long-term periods after surgery. According to their parents, these children showed restlessness and irritability when moving. 8 (10.1 %) patients older than 7 years complained of a headache in the lumbar region. Nocturnal enuresis was observed in 12 (15.2 %) patients. The revealed objective data and subjective feelings in patients can be regarded as a manifestation of the latent dysraphism of the fixed spinal cord syndrome (SPS), which develops independently of the specific form, and the variability of clinical manifestations depends on the severity of this disorder.The clinical significance of latent spinal dysraphism was identified in 51 (15.89%) patients with anorectal abnormalities, in 13(4.05%) with urogenital abnormalities, and in 30(9.34%) children who underwent surgery for the nature of the established pathology deserve attention. According to the results of preoperative complex studies, the frequency of latent spinal dysraphism was also different by the nature of the detected disorders (Table 2).Table 2. Combined lumbosacral dysraphism in anorectal, urogenital, and coloproctological anomalies in children (n = 94)
 |
| |
|
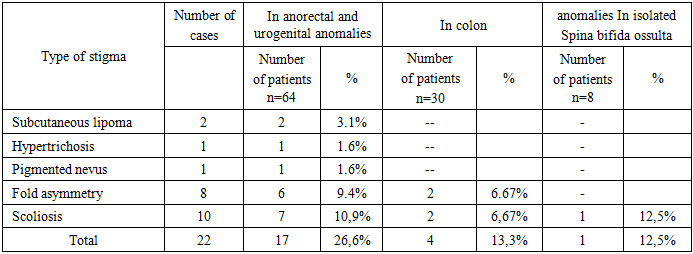
Digital spondylography was performed in 22 (34.4%) of 64 patients with anorectal and urogenital abnormalities. The method was not sensitive enough to detect certain types of SSD. The remaining patients underwent spinal MSCT. According to radiological methods, in 7 (10.9%) patients of this group, changes in the spinal column of patients were manifested by scoliosis. In 12 patients (54.5%), abnormalities of the sacrum and coccyx were detected. 7 of them - hypoplasia and agenesis of the coccyx, and 5 - abnormalities of the sacrum. 33 (51.6%) patients were diagnosed with non-narrowing of the vertebral arches mainly of the lumbosacral localization covering one (9), two or more vertebrae (24). 6 (6.25%) children had a combination of separate forms of spinal anomalies in the form of non-narrowing and agenesis in various parts. Localization of the terminal thread in the spinal cord structure were detected on MSCT in 6 cases. 4 (6.25%) patients had tetring syndrome, 2 (3.13%) had intradural lipoma. In 30 children with coloproctological anomalies, 2 (6.7%) children had posture disorders, 2(6.7%) children had sacral malformations, and 1 had vertebral body anomalies localized in the lumbosacral region. 22 (73.3%) patients were diagnosed with non-occlusion of the vertebral arches in the lumbosacral region covering two vertebral arches. (8) and more vertebrae (14). 1 (3.3%) patient was diagnosed with tetring syndrome.As can be seen from Table 2, 64(68%) patients with anorectal and urogenital anomalies and 30 (32%) patients with colonic anomalies had SS in the form of associated anomalies with a predominance of sacro-vertebral dysraphism (CPD) – 91 (96.8%) over neuro-spinal (NSD) -7 (7.44%). By the nature and frequency of the lesion, the established disorders were pronounced in anorectal and urogenital anomalies,more than in pathology of the colon. The difference in causal factors in the genesis of functional disorders causes a radical difference in the intensity and nature of neurological disorders. This is confirmed by the presence of somatic, neurological and vegetative disorders in anorectal and urogenital anomalies and the predominance of vegetative disorders with moderate or no somatic, neurological symptoms in patients with anomalies of the colon.Isolated Spina bifida okkulta, detected in 8 patients, was the most common type of latent spinal dysraphism. Non-occlusion of the arches of one vertebra (mainly lumbar) was noted only in 1 case. In 7 patients, non-narrowing of the arches was observed over several vertebrae: with localization in the lumbar region in 2, sacral - in 3, and simultaneously within the specified localizations-in 2 patients. As a rule, with malformations of the sacrococcygeal spine, the development of the sacral plexus suffers, the branches of which innervate the sphincter apparatus of the bladder and rectum. what can cause a decrease in tactile sensitivity of the perineum and functional disorders of various dynamics. Pelvic organ dysfunction alone or in combination (persistent constipation-30, chronic constipation with paradoxical fecal incontinence-14, fecal and urinary incontinence-38, urinary incontinence-20) without pronounced anatomical disorders of the anorectal zone and the predominance of extended non-inflamed arches in the lumbosacral region with coverage of "interested zones" - S I and SII do not exclude the role of neuro-spinal and lumbosacral dysraphism in the genesis of these disorders. Orthopedic disorders in SS in the form of hip dysplasia were detected in 6 patients, and asymmetry of the gluteal folds - in 8. Along with ultrasound examination, 13 (12.7%) patients with urinary system pathology additionally underwent MSCT with excretory urography, which allowed obtaining information about the anatomical and functional state of the kidneys and urinary system. Agenesis of the right kidney was found in 3 patients, ureterohydronephrosis – in 8 (one of them on both sides); incomplete doubling in 2 (one of them with ectopia of the right ureter in the perineum).MSCT and contrast irrigography performed in 30 (29.4%) patients with colon pathology made it possible to assess the condition of the colon. In patients with functional disorders of the act of defecation, latent spinal dysraphism was represented by less pronounced and rare combined forms.SS is characterized by skin stigmas of dysembryogenesis, located along the midline, more often in the lumbosacral region (Table 3).Table 3. Skin stigmas in spina bifida occulta
 |
| |
|
As can be seen from Table 3, in anorectal and urogenital anomalies, skin stigmas are often and variously observed. The data obtained correlates with the number and nature of combined anomalies in these groups. Accordingly, among patients with anoand urogenital anomalies, malformations were of various forms with more severe persistent functional disorders than in patients with elongations of various parts of the colon, accompanied by chronic colostasis.The dynamics of neurological manifestations at different stages of treatment is of interest. Latent spinal dysraphy (spina bifida occulta) were detected in 102 (31.8%) patients. Of these, 58 (56.9%) had no motor disorders: 8 (7.8%) had no concomitant abnormality, 20 (19.6%) had latent spinal dysraphy with colon pathology, and 20 (19.6%) had anorectal abnormalities and urological pathology with disorders of the act of defecation and urination in various manifestations and combinations. 30 (29.4%). The main neurological disorders in them were manifested by violations of the functions of the pelvic organs. 44 (43.1%) patients had motor disorders in the form of paresis (3-4 MRS scores), muscle hypotension, lower limb muscle weakness, and decreased knee reflexes. When assessing the anal reflex, 26 (59%) of them showed weakness of the rectal sphincter apparatus. 5 (11.4%) patients had signs of CNS damage associated with asphyxia and intra-natal lesions during labor; clear neurological disorders of the spinal nature: asymmetry of reflexes, sensitivity disorders, including pelvic organ dysfunction. Sensitivity disorders in 4 (9%) children were manifested by segmental, conduction and radicular changes in the lower extremities and perineum in the form of hyposthesia. All children in this group had constipation, intermittent feces, and signs of neurogenic bladder dysfunction in the form of urinary retention or incontinence. Anorectal and urogenital anomalies were presented in the form of fistulous and fistulous forms of rectal atresia; cloaca, infravesical obstruction, malformations of the kidneys and urinary tract. In all cases, these anomalies were accompanied by violations of the act of defecation or urination of varying degrees of severity in isolation or in combination. Among patients with anomalies of the colon, functional disorders in 14 (46.7%) were manifested by persistent chronic constipation, difficult to respond to conservative therapy; chronic constipation with paradoxical fecal incontinence – 2(6.7%). The causes of these disorders were congenital elongation of the sigmoid colon-dolichosigma 7(23.3%); elongation of the colon – dolichocolon 14(46.7%); elongation and expansion of the entire colon - megadolichocolon 4(13.3%) or expansion of the rectum – megarectum 5(16.7%).The presented data indicate that in the zone of segmental innervation, depending on the severity, nature and extent of latent spinal dysraphism, functional disorders are observed, often with abnormalities in the development of the corresponding organs and systems. This is confirmed by the opinions of some authors about the violation of organogenesis in the zone of segmental innervation of organs, which can be explained by the commonality of embryogenesis of these pathologies and anomalies of the distal spine [Y. Liu 2003; Tsou P.M. 1977; Lonstein J.E. 1983; A/Di Cesare 2010]. Therefore, it is necessary to purposefully examine each patient for spinal and spinal cord pathology, follow-up and treatment should be carried out jointly with a pediatric surgeon and neurologist. Early diagnosis of SSD primarily depends on the alertness of pediatricians and doctors of other specialties to this pathology. Identification of skin stigmas in the lumbosacral region, the appearance and progression of neurological symptoms, pelvic organ dysfunction, orthopedic disorders, the presence of anorectal, urogenital abnormalities and colon pathology in a child should be considered for the detection of latent spinal dysraphism. The main diagnostic methods for latent spinal dysraphism are MRI and MSCT. When making a final diagnosis, it is very important to take into account the results of electrophysiological and ultrasound studies aimed at identifying subclinical neurological disorders and structural and functional conditions of the organs concerned. Spinal dysraphism is a diverse and heterogeneous group of malformations of the spine and spinal cord, often observed in severe forms of spinal hernias, in combination to anorectal, urogenital anomalies and malformations of the colon. Pathology is manifested by disorders of the spine in the form of spinal malformations or combined osteoneural anomalies and can cause the development of functional disorders, violations of vegetative and somatic innervation of organs in the area of their segmental lesion. SSD, regardless of the type of nosological forms (spinal lipomas, syringomyelia, hydromyelia, diastematomyelia), can lead to the development of spinal cord fixation syndrome before surgery or at various times after it. The clinical manifestations of SSD are polymorphic and non-specific. Their severity depends on the extent and severity of hidden lesions of the spine and spinal cord. If a child has skin stigmas of dysembryogenesis, manifestations of coloproctological or urogenital abnormalities, studies are needed to identify latent spinal dysraphism and determine the optimal treatment strategy for the main and concomitant pathologies.
References
| [1] | Al-Absi Esmat A.M. Radiological diagnostics of malformations of the caudal spinal cord and spine in childhood: abstract of the dissertation. Candidate of Medical Sciences. - SPb., 2016. - 24 p. |
| [2] | Akhmediev Sh. R. Akhmediev M. M. Fixed brain syndrome in children with spinal dysraphy // Achievements, problems and prospects of children and adolescents ' health protection: Proceedings of the Republican Scientific and Practical Conference.Tashkent, 2014, pp. 27-29. |
| [3] | Braev A. T., Erokhin A. P., Nikolaev V. V. Diagnosis and treatment of urological complications, and approaches to the treatment of children with myelodysplasia. / "Present and future of pediatric surgery". Conference materials. Moscow. - 2018 P. 40. |
| [4] | Voronov V. G. Midlenko M. A. Sebelev K. I. Potemkina E. G. Ivanov A. A. Defects of the cranio-vertebral region-St. Petersburg State University Publishing House Center-2008. Ulyanovsk P. 35. |
| [5] | Demyanenko V. A., Kabanyan A. B. Baidakov A. P., Yerzhakov S. V. Firsov A. L. Diagnostics and treatment of types of latent spinal dysraphism (Spina bifida occulta): dorsal dermal sinus, fixed spinal cord syndrome. Kuban Scientific Medical Bulletin No. 6 (135) 2012. C / 85-87. |
| [6] | Kushel Yu. V., Zemlyansky M. Yu . Syndrome of "Secondary fixation of the spinal cord" after correction of various forms of spinal dysraphism in children NEUROSURGERY, No. 2, 2020 p. 41-46. |
| [7] | Rudakova A.V., Larionov S. N. Features of diagnosis and treatment of spinal malformations in childhood. Bulletin of the Supreme Scientific Center of the Siberian Branch of the Russian Academy of Medical Sciences, 2012, 4 (86) Part 2. p. 110-113. |
| [8] | Khachatryan V. A., Elikbaev G. M. Myelodysplasia in children. Features of diagnostics and clinic. Neurosurgery and Neurology of Kazakhstan No. 1 (14), 2019, pp. 15-23. |
| [9] | Yugay I. A. Akhmediev M. M. Makhmudov Sh. D. Vozmozhnosti magnitno-rezonansnoi tomografii pri spinalnykh disraficheskikh zabolevaniyakh [Possibilities of magnetic resonance imaging in spinal dysraphic diseases]. |
| [10] | Erhan Arslan, Kayhan Kuzeyli, Elif Acar Arslan. Intraspinal Lipomas Without Associated Spinal Disrafism. Iran Red Crescent Med J. 2014 May; 16(5): e11423. |
| [11] | José Murillo B. Netto, André N. Bastos, André A. Figueiredo, Luis M. Pérez. Spinal Dysraphism: A Neurosurgical Review for the Urologist. Rev Urol. 2014; 11(2): 71-81. |
| [12] | Ergasheva N.N. Fixed spinal cord in the genesis of neurological disorders in children with osteoneural dysplasia // Messenger of TMA. - Tashkent. - 2018. - No. 3. - P. 30–34 (14.00.00; 13). |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML